










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Public Health
versão impressa ISSN 2504-3137versão On-line ISSN 2504-3145
Port J Public Health vol.36 no.3 Lisboa 2018
https://doi.org/10.1159/000495804
RESEARCH ARTICLE
Effect of Mode of Delivery on Early Oral Colonization and Childhood Dental Caries: A Systematic Review
Efeito do tipo de parto na colonização oral e cárie dentária nas crianças: Revisão sistemática da literatura
Celeste Antão a Cristina Teixeira a b Maria José Gomes a
a Polytechnic Institute of Bragança, Bragança, Portugal
b EPI Unit, Instituto de Saúde Pública da Universidade do Porto, Porto, Portugal
ABSTRACT
This review investigated whether mode of delivery influences the colonization of infant’s oral cavity and the risk of early childhood caries (ECC). The search strategy included systematic searching of electronic databases (Web of Science and PubMed) for articles published (1995-2015) and hand searching of references lists. Outcomes of interest were the presence of oral cariesrelated microorganisms, oral species considered protective against caries, and dental caries. Other outcomes included severity of dental caries, dental claims, and age at first dental visit. Study quality was assessed using the EPHPP tool. For each study, we present odds ratios and respective 95% confidence intervals for the association between these outcomes and the mode of delivery. Fourteen studies were identified. In 5 out of 8 studies addressing oral colonization, children born by cesarean section were less likely to harbor cariesrelated microorganisms as well as protective bacteria against caries and acquired cariesrelated microorganisms earlier, when compared with vaginally delivered children. No consistent results were obtained for the association between mode of delivery and dental caries. Although there were differences in oral colonization by mode of delivery, it seems that other determinants rather than mode of delivery could be major contributors to the development of ECC.
Keywords: Childhood Colonization Dental caries Cesarean section
RESUMO
Esta revisão investigou se o tipo de parto influencia a colonização da cavidade oral do bebé e o risco de cárie precoce na infância (CPI). A estratégia de pesquisa incluiu a pesquisa sistemática em bases de dados eletrónicas (Web of Science e PubMed) para artigos publicados (1995-2015) e a pesquisa manual de listas de referências. Os principais resultados apontaram para a presença de microrganismos relacionados com a cárie oral, espécies orais consideradas protetoras contra a cárie e a cárie dentária. Outros resultados obtidos incluíram a gravidade da cárie dentária, as reclamações odontológicas e a idade na primeira consulta odontológica. A qualidade do estudo foi avaliada usando a ferramenta EPHPP. Para cada estudo apresentamos oddsratio (OR) e respetivos intervalos de confiança de 95% (IC 95%) para a associação entre esses desfechos e o tipo de parto. Foram identificados catorze estudos. Em cinco de oito estudos abordando a colonização oral, as crianças nascidas por cesariana foram menos propensas a abrigar microrganismos relacionados com a cárie, bem como bactérias protetoras contra a cárie e microorganismos relacionados com cárie adquirida anteriormente, quando comparadas com crianças nascidas de parto vaginal. Não foram obtidos resultados consistentes para a associação entre o tipo de parto e a cárie dentária. Embora houvesse diferenças na colonização oral por tipo de parto, parece que outros determinantes, em vez do tipo de parto, podem ser os principais fatores que contribuem para o desenvolvimento da CPI.
Palavras-chave: Infância · Colonização oral · Cáries dentárias · Cesariana
Introduction
Early childhood caries (ECC) has been defined as the presence of decayed tooth surfaces among children up to 6 years old and is the most common chronic childhood disease 1. ECC is related to oral pain which has adverse effects on children such as lost sleep, eating problems, behavioral problems, and reduction in preschool or school attendance (1 , 2 ). Moreover, advanced forms of ECC usually require general anesthesia for treatment 2. Therefore, ECC emerges as an important public health issue with significant economic impact 3, and it deserves particular attention with regard to the factors that define the risk profile of children.
The presence of cariogenic microorganisms on tooth surfaces plays an essential role in the occurrence of dental caries (4 6 ). Streptococcus mutans and Streptococcus sobrinus (often considered a group called mutans streptococci), have been considered the most common acid producers associated with the carious lesion (4 , 6 9 ). These bacterial species along with Streptococcus salivarius were associated with caries 8, particularly among young children (6 , 8 , 9 ).
Successful colonization by mutans streptococci depends on the number of other commensal bacteria already present in the oral cavity because they need to compete for nutrients (7 , 10 ). Therefore, as the density of other pioneer oral microbiota increases, the chance of successful colonization by mutans streptococci will decrease. Furthermore, a number of common plaque microorganisms such as Streptococcus sanguinis and Streptococcus gordonii are able to catabolize the amino acid arginine to ammonia favoring a pH rise (8 , 10 , 11 ) which could counteract the harmful effect of low pH on the tooth surface. Therefore, bacterial colonization in a child’s mouth is the most important event underlying the pathogenesis of ECC.
Oral colonization starts at birth by vertical transmission from mother to child 12. The birth canal presents a high density of microorganisms which might be acquired by vaginally delivered babies 13. By comparison, the exposure to maternal microorganisms is dramatically weakened among newborns delivered by cesarean section resulting in atypical oral microbiota. Accordingly, it has been postulated that babies born by cesarean section are vulnerable to early oral colonization by cariogenic microorganisms and they will present increased risk of ECC 14.
There has been a dramatic rise in rates of cesarean section over recent decades 15. In a public health perspective, it seems important to know whether infants delivered by cesarean section should be considered a risk group for ECC in order to intensify preventive measures against dental caries among these children.
Therefore, the aim of this study was to present a systematic review of evidence on whether mode of delivery has an impact on colonization of infant’s oral cavity and on the risk of childhood dental caries.
Methods
Search Strategy
Our systematic review was performed according to the procedures of the Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA) 16. However, the protocol of the study was not registered. A comprehensive electronic search of relevant literature was conducted in Web of Science (Thomson Reuters) and PubMed databases for articles published over the last two decades (January 1995 - March 2016). We used keywords for each of the following items: (1) population (“infant,” “child*,” “newborn”); (2) exposure (“mode of delivery,” “delivery mode,” “surgical delivery,” “cesarean delivery,” “caesarean delivery,” “cesarean section,” “caesarean section,” “csection,” “birth,” “childbirth”); and (3) outcome (“streptococ*,” “lactobacil*,” “bacteria*,” “oral health,” “dental health,” “caries” OR “dental caries,” “dental decay,” “tooth decay,” “teeth decay,” “decayed tooth,” “decayed teeth,” “decayedmissingfilledteeth,” “dmft,” “early childhood caries,” “oral bacteria,” “oral bacterial community,” “oral biota,” “oral pioneer community,” “oral micro*,” “oral acquisition,” “oral colonization”).
Eligibility Criteria
We included all types of observational (cohort, crosssectional, and casecontrol) studies reporting results about the effect of mode of delivery on early oral colonization and ECC among children 6 years old or younger. The exposure of interest was the mode of delivery defined as cesarean section versus vaginal delivery. Our outcomes of interest were: (1) prevalence of cariesassociated species: S. mutans , S sobrinus , and S. salivarius ; (2) prevalence of microbial protective factors against caries: S. sanguinis and S. gordonii ; (3) prevalence of dental caries; (4) severity of dental caries assessed by the mean of decayedmissingfilled tooth (DMFT) and decayedmissingfilled tooth surface (DMFS) index; (6) other outcomes included dental claims and time of first dental caries.
Studies were eligible if they presented the results using measures of association (odds ratio (OR), relative risk, or hazard ratio) between the mode of delivery and the outcomes of interest, or raw data were available in order to compute them, or information about differences between groups by mode of delivery for outcomes of interest were provided throughout the paper.
We excluded case report studies, literature reviews, letters to the editor, study protocols, and studies in languages other than English, Portuguese, French, and Spanish.
Study Selection
The titles and abstracts of all references obtained were scrutinized and the full text of potentially eligible citations was retrieved for further assessment. Two authors (C.A. and C.T.) screened titles and abstracts to exclude citations beyond the scope of this review. Abstracts reporting the association between perinatal factors (birthweight, gestational age, pregnancy or delivery factors, and breastfeeding) and outcomes of interest were considered potentially eligible citations. A further selection was conducted by all the authors who independently reviewed the full text of the abstracts identified as potentially eligible citations. Disagreements were settled by consensus discussion.
Additionally, the reference lists of selected citations were screened to identify further relevant studies using the same inclusion criteria.
Methodological Quality Assessment
For quality assessment, we used the Quality Assessment Tool for Quantitative Studies developed by the Effective Public Health Practice Project (QATEPHPP) (17 , 18 ). This tool assesses the strength of the studies across six methodological items (selection bias, study design, confounders, blinding, data collection methods, and withdrawals/dropouts). Studies are rated weak, moderate, or strong on each methodological item, and a global rate for each study is obtained as follows: strong (if no weak ratings), moderate (if one weak rating), and weak (if the study presents 2 or more weak ratings) 18. We intended to include all studies reporting results about the effect of the mode of delivery on the outcomes of interest, independent of the main objective presented by the authors. Therefore, for some studies the mode of delivery could appear as one of several determinants or as a potential confounder rather than the exposure of interest. Taking into account such circumstance, we did not consider the item of QATEPHPP asking about confounders. However, we retrieved information on adjusted measures of association or whether groups by mode of delivery have similar distribution of potential confounding factors.
Two reviewers (C.A. and C.T.) independently assessed the methodological quality of studies. Any discrepancies between reviewers concerning the item ratings were resolved through discussion and, when necessary, a third reviewer (M.J.G.) was consulted.
Data Extraction
Authors independently extracted information from each eligible study based on the following data: first author, publication year, sample size, type of study, age of participants, outcome of interest, criteria to define outcome of interest, and estimates of measures of association between mode of delivery and outcomes of interest.
Data Synthesis
Due to large differences of the included studies with regard to the study design, methods for sample recruitment and particularly age of children evaluated, metaanalysis was not performed. For each study, the OR and respective 95% confidence interval (95% CI) for the association between mode of delivery and the outcome of interest were obtained. Vaginally delivered children were considered the reference group. When necessary, the equivalent of OR and respective 95% CI were computed. When measures of association were not provided by the authors, OR and 95% CI were computed from raw data retrieved from tables or from the text. Thus, the number of positive and negative outcomes for each group by mode of delivery was extracted from studies, and the OR and respective 95% CI were computed. Moreover, mean and respective standard deviation for DMFT, DMFS and the age at S. mutans acquisition were retrieved from studies. All results were stratified according to the age of children as provided by the authors.
Results
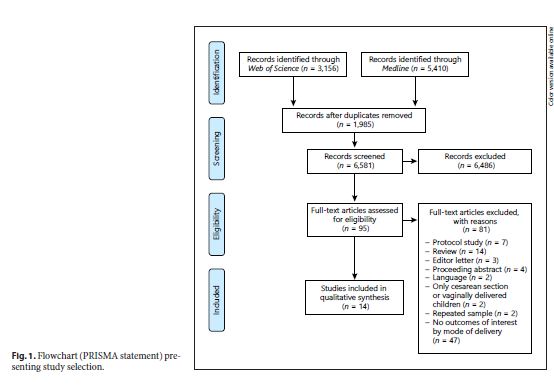
As described in detail in the flowchart (Fig. 1), the search strategy yielded 14 studies meeting the established criteria. The main characteristics of the studies including the outcomes assessed are described in Table 1. According to the methodological quality assessment, 5 studies were classified as strong (19
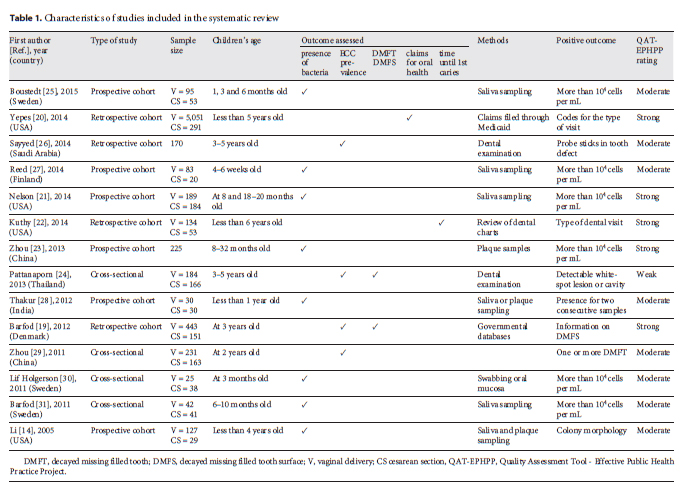
23 ), 1 study as weak 24, and the remaining studies were considered moderate (14 , 25 31 ).
Prevalence of Children Who Present Cariogenic-Related Species
Eight studies (14 , 21 , 23 , 25 , 27 , 28 , 30 , 31 ) showed results on differences between groups by the mode of delivery in the prevalence of children with S. mutans (or mutans streptococci) and/or S. salivarius. Results were stratified according to the children’s age and summarized in Table 2. The prevalence of children with positive status varied across studies, ranging from 4.8 30 to 79.9% 25 for S. mutans and from 53.3 25 to 67.5% 31 for S. salivarius.
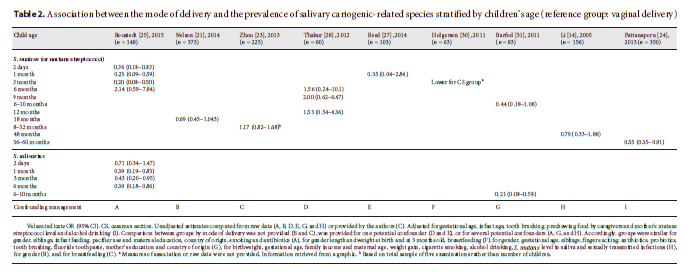
With regard to the colonization by S. mutans, there were no consistent results across studies. Three studies rated weak 24 to moderate (25 , 30 ) in quality assessment reported significant lower frequency of S. mutans detection among infants born by cesarean section compared with those vaginally delivered but only among younger groups (2 days, 1 month, and 3 months old). Instead, 6 studies that were considered to have moderate (14 , 27 , 28 , 31 ) to strong (21 , 23 ) methodological quality reported no significant differences in prevalence of oral colonization by S. mutans between groups by mode of delivery (Table 2).
Two studies (25 , 31 ) rated as moderate in quality assessment provided data on prevalence of salivary S. salivarius by mode of delivery. In both studies, cesarean section appeared as a protective factor against presence of S. salivarius in saliva for children aged between 1 and 10 months (Table 2).
Prevalence of Children Who Present Protective Species against Caries
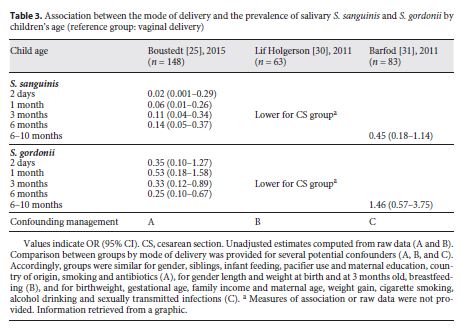
Three studies that scored moderate (25 , 30 , 31 ) in methodological quality assessed the association between mode of delivery and the prevalence of both salivary S. sanguinis and S. gordonii. The prevalence of salivary microorganisms varied across studies ranging from 6.4 30 to 65% 31 for S. sanguinis and from 4.8 30 to 30.0% 31 for S. gordonii.
In 2 studies (25 , 30 ), salivary S. sanguinis and S. gordonii were detected less frequently from cesarean section compared with vaginally born infants, although differences in S. gordonii detection lose their statistical significance among infants aged 2 days and 1 month. However, the third study 31 reported no significant differences in oral colonization pattern of S. sanguinis and S. gordonii by mode of delivery (Table 3).
Prevalence of Dental Caries
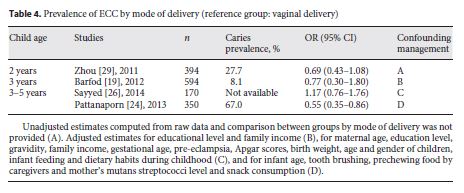
Four studies presented results on caries prevalence by mode of delivery (19 , 24 , 26 , 29 ). The prevalence of caries varied across studies, ranging from 8.1 19 to 67.0% 24. A study that scored weak 24 reported significant differences in prevalence of dental caries by mode of delivery among children aged 3-5 years such that children born by cesarean section presented lower odds of dental caries than those vaginally delivered. Three studies that scored moderate (26 , 29 ) to strong 19 reported no differences in dental caries prevalence between groups by mode of delivery (Table 4).
Severity of Dental Caries
Two studies compared groups by mode of delivery with regard to DMFT and DMFS; one reported results about children aged 3 years 19, and the other presented stratified results at age 3 and 5 years 24.
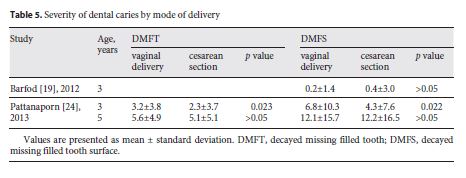
Among children aged 3 years, there were no consistent results between studies. A study rated strong reported a DMFS mean twice as high among children born by cesarean section in comparison with vaginally delivered children (0.4 ± 3.0 vs. 0.2 ± 1.4) 19, although with no statistical significance. Instead, a study 24 rated as weak reported statistically significant lower DMFS mean (4.3 ± 7.6 vs. 6.8 ± 10.3) and lower DMFT mean (2.3 ± 3.7 vs. 3.2 ± 3.8) among children born by cesarean section when compared with their vaginally delivered counterparts. The same study also 24 reported data on dental caries prevalence among children aged 5 years, and no differences were found between groups by mode of delivery, neither for DMFS nor for DMFT (Table 5).
Other Outcomes
A study rated as strong in quality assessment 20 provided data on dental claims among children of 5 years old that indirectly reflects ECC. After adjusting for birth weight, age at first dental visit and mother’s ethnicity, no significant differences were found by mode of delivery neither for restorative (OR = 1.25; 95% CI: 0.86-1.66) nor emergency (OR = 1.25; 95% CI: 0.90-1.66) claims. A moderate quality study reported that mode of delivery was significantly associated with earlier S. mutans acquisition 14, so that children born by cesarean section acquired S. mutans at a younger age than vaginally delivered children (mean age in months: 17.1 ± 1.8 vs. 28.8 ± 1.8; p = 0.038). This association remained significant even after adjustment for maternal factors (age, education level, income, regular cigarette smoking and alcohol drinking, use of antibiotics during pregnancy, caries status, and S. mutans level in saliva). Instead, another moderate quality study 22 reported no significant differences for time to first dental caries by mode of delivery (hazard ratio = 1.31 95% CI: 0.78-2.18; cesarean section is the reference group).
Discussion
According to this review, oral colonization is different between groups by mode of delivery. In 5 out of 8 studies addressing oral colonization, children born by cesarean section were less likely to harbor cariesrelated microorganisms as well as protective bacteria against caries and acquired cariesrelated microorganisms earlier when compared with vaginally delivered children. However, no consistent results were obtained for the association between mode of delivery and dental caries.
The human oral cavity harbors a large range of microorganisms, Streptococci being the most abundant bacteria detected in oral habitats of healthy individuals 32. Although there is evidence for presence of microorganisms in placenta, umbilical cord and amniotic fluid, the first exposure of children to microorganisms occurs at birth 12. It has been reported that the mother’s vaginal microbiota provides a natural microbial exposure to the vaginally delivered newborn (13 , 33 ). By contrast, among children born by cesarean section, the first microbial communities reflect the human skin microbiota 13. Therefore, differences in the mode of delivery may lead to differences in the pattern of microbial acquisition in the gut 34 and other body habitats, such as oral cavity (13 , 33 ), which could have longlasting health effects with clinical relevance.
Our findings are in accordance with previous research reporting higher counts of oral microorganisms among vaginally delivered children in comparison with those born by cesarean section (13 , 30 ). We found that vaginally delivered children are more likely to harbor S. mutans and S. salivarius which are cariesrelated microorganisms, but also S. sanguinis and S. gordonii considered protective bacteria against caries. However, we also observed that such differences are not consistent across studies.
Infant’s oral colonization could be influenced by other factors beyond the mode of delivery. Previous research showed the influence of perinatal factors, such as prolonged rupture of membranes 35, maternal antibiotic treatment 35, and maternal sexually transmitted disease experience 14, on the establishment of oral microflora. Also, oral health behaviors including the frequency of eating sweets and toothbrushing (28 , 29 , 36 , 37 ), bottle feeding and breastfeeding (23 , 28 ), including duration of breastfeeding 38, have been reported as determinants of oral levels of S. mutans. In addition, the parent’s socioeconomic status (28 , 37 ) has been associated with differences in early oral colonization by S. mutans. High levels of maternal salivary mutans streptococci have been also related to an increase in the risk of ECC 39. Another issue that has been reported refers to the differences in the breast milk microbiota according to the mode of delivery, which will have an impact on early oral colonization of breastfed children (35 , 40, 41 42 ). This large set of factors could explain why the association between mode of delivery and oral colonization by cariesrelated microorganisms and by protective microorganism against caries is not consistent across studies. Indeed, there are multiple factors that interact over time in order to determine the establishment of oral microflora. Large differences exist between studies with regard to factors other than the mode of delivery which could interact in different ways to determine oral microflora among children. This means that we should not exclude a potential role of the mode of delivery in the establishment of cariesrelated microorganisms and protective microorganisms against caries. Moreover, the level of mutans streptococci is a strong indicator of ECC 5. Therefore, all factors related to oral colonization other than the mode of delivery will have an impact on the prevalence of dental caries among children.
There is a strong limitation to this review. There are few studies reporting prevalence of dental caries, prevalence of cariesrelated microorganisms, or prevalence of protective microorganisms against dental caries according to mode of delivery. However, to the best of our knowledge this is the first systematic review providing results on the influence of the mode of delivery on such oral health indicators among children.
In summary, according to the results of our systematic review, mode of delivery seems to shape early oral colonization but other factors could modify its effect. Further research should be conducted to give insights on multiple interactions between factors in order to disentangle the role of mode of delivery from the influence of other factors on the oral colonization by cariesrelated microorganisms and dental caries. Professionals should be able to identify children at high risk for dental caries in providing anticipatory guidance to families. Evidencebased policies and practice are essential for dental care quality and are important for highlighting research needed in pediatric dental health 1. Such an approach will have longterm effects on oral health with positive outcomes along life cycle, including an increase in oral health-related quality of life among older people 43.
REFERENCES
1 Rowan-Legg A ; Canadian Paediatric Society, Community Paediatrics Committee. Oral health care for children - a call for action. Paediatr Child Health. 2013 Jan ; 18 (1): 37 - 50. [ Links ]
2 Jankauskiene B , Virtanen JI , Kubilius R , Narbutaite J. Oral health-related quality of life after dental general anaesthesia treatment among children: a follow-up study. BMC Oral Health. 2014 Jul ; 14 (1): 81. [ Links ]
3 Jin LJ , Lamster IB , Greenspan JS , Pitts NB , Scully C , Warnakulasuriya S. Global burden of oral diseases: emerging concepts, management and interplay with systemic health. Oral Dis. 2016 Oct ; 22 (7): 609 - 19. [ Links ]
4 Law V , Seow WK , Townsend G. Factors influencing oral colonization of mutans streptococci in young children. Aust Dent J. 2007 Jun ; 52 (2): 93 - 100. [ Links ]
5 Parisotto TM , Steiner-Oliveira C , Silva CM , Rodrigues LK , Nobredos Santos M. Early childhood caries and mutans streptococci: a systematic review. Oral Health Prev Dent. 2010 ; 8 (1): 59 - 70. [ Links ]
6 Nyvad B , Crielaard W , Mira A , Takahashi N , Beighton D. Dental caries from a molecular microbiological perspective. Caries Res. 2013 ; 47 (2): 89 - 102. [ Links ]
7 Marsh PD. Dental plaque as a biofilm and a microbial community implications for health and disease. BMC Oral Health. 2006 Jun ; 6 Suppl 1 : S14. [ Links ]
8 Gross EL , Beall CJ , Kutsch SR , Firestone ND , Leys EJ , Griffen AL. Beyond Streptococcus mutans: dental caries onset linked to multiple species by 16S rRNA community analysis. PLoS One. 2012 ; 7 (10): e47722. [ Links ]
9 Li Y , Argimón S , Schön CN , Saraithong P , Caufield PW. Characterizing diversity of lactobacilli associated with severe early childhood caries: a studprotocol. Adv Microbiol. 2015 Jan ; 5 (1): 9 - 20. [ Links ]
10 Rogers AH. Why be down in the mouth? Three decades of research in oral microbiology. Aust Dent J. 2005 Mar ; 50 (1): 2 - 5. [ Links ]
11 Caufield PW , Dasanayake AP , Li Y , Pan Y , Hsu J , Hardin JM. Natural history of Streptococcus sanguinis in the oral cavity of infants: evidence for a discrete window of infectivity. Infect Immun. 2000 Jul ; 68 (7): 4018 - 23. [ Links ]
12 Zaura E , Nicu EA , Krom BP , Keijser BJ. Acquiring and maintaining a normal oral microbiome: current perspective. Front Cell Infect Microbiol. 2014 Jun ; 4 : 85. [ Links ]
13 Dominguez-Bello MG , Costello EK , Contreras M , Magris M , Hidalgo G , Fierer N , et al. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci USA. 2010 Jun ; 107 (26): 11971 - 5. [ Links ]
14 Li Y , Caufield PW , Dasanayake AP , Wiener HW , Vermund SH. Mode of delivery and other maternal factors influence the acquisition of Streptococcus mutans in infants. J Dent Res. 2005 Sep ; 84 (9): 806 - 11. [ Links ]
15 World Health Organization. Regional Office for Europe: European health for all database (HFA-DB). Accessed 12.01. 2017. Available at https://gateway.euro.who.int/en/datasets/europeanhealthforalldatabase/ [ Links ]
16 Moher D , Liberati A , Tetzlaff J , Altman DG ; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009 Jul ; 6 (7): [ Links ]
17 Effective Public Health Practice Project. Quality assessment tool for quantitative studies. Hamilton (ON) : Effective Public Health Practice Project ; 2015. [ Links ]
18 Thomas BH , Ciliska D , Dobbins M , Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. 2004 ; 1 (3): 176 - 84. [ Links ]
19 Barfod MN , Christensen LB , Twetman S , Lexner MO. Caries prevalence in Danish preschool children delivered vaginally and by caesarean section. Acta Odontol Scand. 2012 May ; 70 (3): 190 - 3. [ Links ]
20 Yepes JF , Bush HM , Li HF , Talbert J , Nash DA. Antenatal and intrapartum risk factors for use of emergency and restorative Medicaid dental services for children. Pediatr Dent. 2014 SepOct ; 36 (5): 405 - 10. [ Links ]
21 Nelson S , Albert JM , Soderling E , Malik A , Curtan S , Geng C , et al. Increased number of teeth predict acquisition of mutans streptococci in infants. Eur J Oral Sci. 2014 Oct ; 122 (5): 346 - 52. [ Links ]
22 Kuthy RA , Jones M , Kavand G , Momany E , Askelson N , Chi D , et al. Time until first dental caries for young children first seen in Federally Qualified Health Centers: a retrospective cohort study. Community Dent Oral Epidemiol. 2014 Aug ; 42 (4): 300 - 10. [ Links ]
23 Zhou Y , Yang JY , Zhi QH , Tao Y , Qiu RM , Lin HC. Factors associated with colonization of Streptococcus mutans in 8 -to 32-month-old children: a cohort study. Aust Dent J. 2013 Dec ; 58 (4): 507 - 13. [ Links ]
24 Pattanaporn K , Saraithong P , Khongkhunthian S , Aleksejuniene J , Laohapensang P , Chhun N , et al. Mode of delivery, mutans streptococci colonization, and early childhood caries in three to five-year-old Thai children. Community Dent Oral Epidemiol. 2013 Jun ; 41 (3): 212 - 23. [ Links ]
25 Boustedt K , Roswall J , Dahlén G , Dahlgren J , Twetman S. Salivary microflora and mode of delivery: a prospective case control study. BMC Oral Health. 2015 Dec ; 15 (1): 155. [ Links ]
26 Sayyed T , Kandil M , Bashir O , Alnaser H. The relationship between term pre-eclampsia and the risk of early childhood caries. J Matern Fetal Neonatal Med. 2014 Jan ; 27 (1): 62 - 5. [ Links ]
27 Reed SG , Cunningham JE , Latham TN , Shirer SC , Wagner CL. Maternal oral mutans streptococci (MS) status, not breastfeeding, predicts predentate infant oral MS status. Breastfeed Med. 2014 Nov ; 9 (9): 446 - 9. [ Links ]
28 Thakur R , Singh MG , Chaudhary S , Manuja N. Effect of mode of delivery and feeding practices on acquisition of oral Streptococcus mutans in infants. Int J Paediatr Dent. 2012 May ; 22 (3): 197 - 202. [ Links ]
29 Zhou Y , Lin HC , Lo EC , Wong MC. Risk indicators for early childhood caries in 2-year-old children in southern China. Aust Dent J. 2011 Mar ; 56 (1): 33 - 9. [ Links ]
30 Lif Holgerson P , Harnevik L , Hernell O , Tanner AC , Johansson I. Mode of birth delivery affects oral microbiota in infants. J Dent Res. 2011 Oct ; 90 (10): 1183 - 8. [ Links ]
31 Nelun Barfod M , Magnusson K , Lexner MO , Blomqvist S , Dahlén G , Twetman S. Oral microflora in infants delivered vaginally and by caesarean section. Int J Paediatr Dent. 2011 Nov ; 21 (6): 401 - 6. [ Links ]
32 Li K , Bihan M , Methé BA. Analyses of the stability and core taxonomic memberships of the human microbiome. PLoS One. 2013 May ; 8 (5): e63139 [ Links ]
33 Gonzales-Marin C , Spratt DA , Millar MR , Simmonds M , Kempley ST , Allaker RP. Identification of bacteria and potential sources in neonates at risk of infection delivered by Caesarean and vaginal birth. J Med Microbiol. 2012 Jan ; 61 (Pt 1): 31 - 41. [ Links ]
34 Biasucci G , Rubini M , Riboni S , Morelli L , Bessi E , Retetangos C. Mode of delivery affects the bacterial community in the newborn gut. Early Hum Dev. 2010 Jul ; 86 Suppl 1 : 13 - 5. [ Links ]
35 Keski-Nisula L , Kyynäräinen HR , Kärkkäinen U , Karhukorpi J , Heinonen S , Pekkanen J. Maternal intrapartum antibiotics and decreased vertical transmission of Lactobacillus to neonates during birth. Acta Paediatr. 2013 May ; 102 (5): 480 - 5. [ Links ]
36 Liu M , Ge L , Zheng S , Yuan C , Zhang B , Xu T. Short-term effect of mechanical plaque control on salivary mutans streptococci in preschool children. Oral Health Prev Dent. 2014 ; 12 (3): 219 - 24. [ Links ]
37 Corrêa-Faria P , Martins-Júnior PA , Vieira-Andrade RG , Marques LS , Ramos-Jorge ML. Factors associated with the development of early childhood caries among Brazilian preschoolers. Braz Oral Res. 2013 Jul-Aug ; 27 (4): 356 - 62. [ Links ]
38 Chaffee BW , Feldens CA , Vítolo MR. Association of long-duration breastfeeding and dental caries estimated with marginal structural models. Ann Epidemiol. 2014 Jun ; 24 (6): 448 - 54. [ Links ]
39 Chaffee BW , Gansky SA , Weintraub JA , Featherstone JD , Ramos-Gomez FJ. Maternal oral bacterial levels predict early childhood caries development. J Dent Res. 2014 Mar ; 93 (3): 238 - 44. [ Links ]
40 Martín R , Heilig GH , Zoetendal EG , Smidt H , Rodríguez JM. Diversity of the Lactobacillus group in breast milk and vagina of healthy women and potential role in the colonization of the infant gut. J Appl Microbiol. 2007 Dec ; 103 (6): 2638 - 44. [ Links ]
41 Cabrera-Rubio R , Carmen Collado M , Laitinen K , Salminen S , Isolauri E , Mira A. Figure S1: Bacterial taxonomic composition of human breast milk. In: CabreraRubio R, Carmen Collado M, Laitinen K, Salminen S, Isolauri E, Mira A. The human milk microbiome changes over lactation and is shaped by maternal weight and mode of delivery. Am J Clin Nutr. 2012 ; 96 (3): 547.
42 Khodayar-Pardo P , Mira-Pascual L , Collado MC , Martínez-Costa C. Impact of lactation stage, gestational age and mode of delivery on breast milk microbiota. J Perinatol. 2014 Aug ; 34 (8): 599 - 605. [ Links ]
43 Gomes MJ , Teixeira MC , Paçô MT. Preditores clínicos da qualidade de vida relacionada com a saúde oral em idosos diabéticos. Rev Enferm Ref. 2015 ; IV : 81 - 9. [ Links ]
Received: August 23, 2016. Accepted: September 21, 2018
Authors declare no conflict of interest.
C.A. and C.T. conceived the study. C.T. and C.A. conducted the systematic search of the relevant literature. All authors contributed to the review of citations and retrieved relevant information from selected articles. All authors contributed to the interpretation of results, commented on drafts and approved the final version.

