










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Public Health
versão impressa ISSN 2504-3137versão On-line ISSN 2504-3145
Port J Public Health vol.36 no.2 Lisboa 2018
https://doi.org/10.1159/000493886
ORIGINAL PAPER
Oral Health for Patients with Special Needs: Evaluative Research of the Dental Specialties Centers
Saúde bucal para pacientes com necessidades especiais: pesquisa avaliativa de Centros de Especialidades Odontológicas
Victor Pinheiro Gavinaa Nayara Silva Alves b Francielle Ribeiro Alves a Karine Laura Cortellazzi c Flávia Maia Silveira a Andréa Videira Assaf a
a Department of Specific Formation, Universidade Federal Fluminense (UFF), Nova Friburgo, Brazil
b Department of Specific Formation, Universidade Vale do Rio Doce (UNIVALE), Governador Valadares, Brazil
c Department of Social Dentistry, Piracicaba Dental School, University of Campinas (FOP-UNICAMP), Piracicaba, Brazil
ABSTRACT
The Dental Specialties Centers (CEOs) were created within the context of the National Oral Health Policy, and the main function of these establishments is to serve as units of reference in secondary oral health care in the Brazilian national health system (SUS), and they must offer at least the services of stomatology, specialized periodontology, minor oral surgery, endodontics, and attendance to patients with special needs. The aim of this study was to evaluate the quality of the CEOs in the mountain region of the Rio de Janeiro State, Brazil, in the perspective of the patients with special needs care or their companion’s satisfaction. Data were collected from 159 users by using a standardized self-applied individual semi-structured questionnaire. The results indicated a positive evaluation in most of the dimensions, except the accessibility dimension. Significant differences ( p < 0.05) were observed between the services of the following dimensions of quality: accessibility, resoluteness, technical-scientific quality, efficiency, efficacy, and acceptability. The analysis of qualitative data, through the discourse of the collective subject technique (DCS) and social representations, showed five central ideas about users’ satisfaction and dissatisfaction with CEOs services (humanized health care, resoluteness of the service, professional competence, infrastructure and organization of the service, access to the services). In conclusion, most patients with special needs care and their companions were satisfied with specialized dental centers (SDC) services, although there were significant differences among SDCs services in relation to individuals’ satisfaction.
Keywords: Patient satisfaction Quality of health care Disabled persons Oral health Unified health system Humanization of assistance -
RESUMO
Os Centros de Especialidades Odontológicas (CEOs) foram criados dentro do contexto da Política Nacional de Saúde Bucal e a principal função desses estabelecimentos é servir como unidades de referência em atenção secundária à saúde bucal no SUS, devendo oferecer pelo menos os serviços de estomatologia, periodontia especializada, cirurgia oral menor, endodontia e atendimento a pacientes com necessidades especiais. O objetivo deste estudo foi avaliar a qualidade dos Centros de Especialidades Odontológicas da região serrana do Estado do Rio de Janeiro, Brasil, por meio da satisfação dos pacientes com necessidades especiais ou de seus acompanhantes. Os dados foram coletados de 159 usuários utilizando um questionário semiestruturado individual auto-aplicado padronizado. Os resultados indicaram uma avaliação positiva na maioria das dimensões, exceto na acessibilidade. Diferenças significativas (p < 0.05) foram observadas entre os serviços nas seguintes dimensões de qualidade: acessibilidade, resolutividade, qualidade técnico-científica, eficiência, eficácia e aceitabilidade. A análise dos dados qualitativos, por meio da técnica do Discurso do Sujeito Coletivo (DSC) e das representações sociais, apresentou cinco ideias centrais sobre a satisfação e insatisfação dos usuários com os serviços dos CEOs (cuidado humanizado, resolutividade do serviço, competência profissional, infraestrutura e organização do serviço, acesso aos serviços). Em conclusão, a maioria dos pacientes com necessidades especiais e seus acompanhantes estavam satisfeitos com os serviços dos CEOs, embora houvesse diferenças significativas entre os serviços dos CEOs em relação à satisfação dos indivíduos.
Palavras-chave: Satisfação do paciente · Qualidade da assistência à Saúde · Pessoas com deficiência · Saúde bucal · Sistema Único de Saúde · Humanização da assistência
Introduction
In dentistry, patients with special needs are classified as all individuals who present physical, sensory, mental, growth, or medical limitations, whether they are transitory or permanent, and who therefore need differentiated dental treatment. This concept is broad in scope, considering the amplitude of cases that may fit into this definition 1.
According to data published by the World Health Organization (WHO), there are approximately 600 million persons with disabilities in the world; that is, 1 in every 10 persons 2. In Brazil, according to the Demographic Census of 2010, this population consists of approximately 45.6 million persons, which corresponds to approximately 23.9% of the Brazilian population. In the state of Rio de Janeiro, the population of disabled persons (3.9 million persons) represents approximately 24.4% of the total population of the state 3. In spite of this high contingent of the population, estimates have indicated that the health care needs of only 2% of the disabled population are met 4.
Health care of persons with special needs is a key element for their inclusion in the society, and consequently this inclusion reflects the equity of access to and use of public health services. Equity in the development and execution of public health policies for disabled persons consists of treating the unequal in an equal manner. Therefore, this principle in the implementation of health programs consists of favoring the neediest groups with regard to access to and use of health services, and this must be the guiding objective of public health policies 5.
The National Health Policy for Persons with Disabilities, and the Plan “Viver Sem Limites” (Live without Limits) proposed the insertion of patients with special needs across the different Ministry of Health programs, and the creation of a Network of Care for Persons with Disabilities within the scope of the Brazilian national health system (SUS). Furthermore, this policy foresees an articulation with the national coordination of oral health so that dental care for patients with special needs will be performed in the “Smiling Brazil” program in a special outpatient system, or in cases of greater need, in a hospital system 6. The WHO Convention about the Rights of Persons with Disabilities also guarantees the right to access to and use of goods and services in health to disabled persons, without there being any type of discrimination 7.
The Dental Specialties Centers (CEOs) were created within the context of the National Oral Health Policy, and the criteria, standards, and requisites for its implementation and accreditation were instituted by means of Administrative Ruling No. 599/GM. The main function of these establishments is to serve as units of reference in secondary oral health care in SUS, and they must offer at least the services of stomatology, specialized periodontology, minor oral surgery, endodontics, and attendance to patients with special needs 8. Within this perspective of a larger offer of health services to patients with special needs, financial incentives of contribution to costs were created for CEOs that adhered to the Network of Care for Persons with Disabilities by means of Administrative Ruling No. 835/GM. Therefore, it is mandatory for a CEO that adheres to this network to offer attendance to disabled persons consisting of at least 40 h per week, in a dental chair exclusively for this type of attendance 9.
Evaluation is a fundamental step when the quality of health services is to be attained, and an instrument is essential for planning, management, and reorientation of public health policies and allocation of resources, which could generate the necessary transformation for improving and enhancing these services ( 10 , 11 ).
According to the present perspectives, evaluation of quality must also be based on the users’ satisfaction 12, thus constituting a fundamental quality indicator 10, because it allows the dentist-patient relationship and humanization of dental attendance to be analyzed, and to evaluate factors such as access, waiting time, infrastructure, organization, patient satisfaction with treatment performed and service provided ( 10 , 13 , 14 ). In addition, it could collaborate with the proposals for enhancing the quality of the service 12.
In the search for a validated quantitative instrument for evaluating the oral health services, the “Questionário de Avaliação dos Serviços de Saúde Bucal (QASSaB)” (Oral health service evaluation questionnaire) was created based on the Donabedian 15 model of quality evaluation that at present comprises seven new dimensions of quality: efficacy, effectiveness, efficiency, optimization, acceptability, legitimacy, and equity 16. However, user satisfaction is a complex phenomenon, and the use of quantitative instruments only is inadequate to measure it. The use of quantitative instruments based on open questions about experiences and personal opinions of persons interviewed may be an efficient alternative for this type of evaluation 17.
In view of the foregoing, the aim of this study was to evaluate the CEOs of the mountain (serrano) region of the State of Rio de Janeiro, by means of the satisfaction of users with special needs and the persons who accompany them with the services provided in these establishments.
Introduction
Characterization of the Municipalities and Their Respective Services
The present study is of the descriptive, cross-sectional type with exploratory and evaluative characteristics of a qualitative and quantitative nature. The study was developed in the CEOs belonging to the municipalities that adhered to the intermunicipal health consortium of the mountainous (serrano) region of the State of Rio de Janeiro (CIS-Serra).
The municipalities of the State of Rio de Janeiro that adhered to the CIS-Serra up to February 2016 were: Bom Jardim; Cachoeiras de Macacu; Cantagalo; Carmo; Cordeiro; Duas Barras; Guapimirim; Macuco; Nova Friburgo; Petrópolis; Santa Maria Madalena; São José do Vale do Rio Preto; Sumidouro; and Trajano de Moraes.
Among the municipalities belonging to this consortium, only Petrópolis, Bom Jardim, Cachoeiras de Macacu, and São José do Vale do Rio Preto have the installation of a secondary care service in their oral health care network, represented by the CEOs. However, in the period during which this study was conducted, the municipality of São José do Vale do Rio Preto did not offer the specialty of attendance to patients with special needs, and therefore, the authors opted not to include the CEO of this municipality in the study. The sociodemographic characteristics of the municipalities and their respective CEOs are shown in Figure 1 .
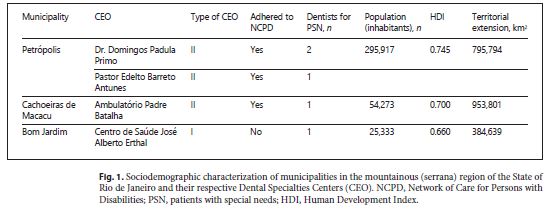
Sociodemographic characterization of municipalities in the mountainous (serrana) region of the State of Rio de Janeiro and their respective Dental Specialties Centers (CEO). NCPD, Network of Care for Persons with Disabilities; PSN, patients with special needs; HDI, Human Development Index.
Sample Selection
The sample of users with special needs and the persons who accompanied them consisted of 159 individuals, and this population was distributed as follows: CEO A ( n = 63), CEO B ( n = 41), CEO C ( n = 32), and CEO D ( n = 23). The sample was selected from among individuals with special needs who consulted the CEOs in the period of 2 months; and the total period in which the study was conducted was 8 months (July 2015 to February 2016), i.e. 2 months for each health establishment.
The inclusion criteria of this study were: all the users with special needs, who were submitted to a dental procedure (dental treatment) at least once, and who accepted to participate in the study. Individuals with any type of special needs were interviewed, with the exception of those with intellectual/cognitive disability, or those under 18 years of age. In this case, these individuals were included in the study, with the participation of the respective persons who accompanied them/guardians on the day of consultation. The exclusion criteria were: all the individuals who refused to sign the Term of Free and Informed Consent, or Term of Free and Informed Assent; individuals who refused to participate in the research; and individuals who did not fulfill the inclusion criteria.
Thus, in 60 interviews, the patients themselves responded to the questionnaire, and in the 99 remaining interviews, the persons who accompanied them/guardians responded to the same questionnaire due to the criteria previously established for participation in the study.
Pilot Study and Interviewer Training
The pilot study was conducted to evaluate the level of understanding of the questions by the interviewees ( n = 10) and make the possible changes in the semi-structured questionnaire.
Training consisted of preparing the interviewer for applying the questionnaire. This preparation was made by a researcher with previous experience in this type of research, by means of conducting some interviews ( n = 10) with a duration of 8 h.
Qualitative and Quantitative Measurement Instrument
Data were collected by one previously trained researcher, in reserved rooms at the respective CEOs, preserving the privacy of the interviewees. The instrument used for this collection consisted of semi-structured questionnaires made up of two parts. The first part consisted of closed questions, with information about the socioeconomic and demographic characteristics of the interviewees, and the integrality of the oral health services. The second part of the questionnaire consisted of open and closed questions, based on the Oral Health Service Evaluation Questionnaire (Aqsa), a validated instrument for assessing services, widely used for evaluating oral health services 15.
In this study, the Aqsa covered the following quality dimensions: (1) Accessibility; (2) Resoluteness; (3) Physical Environ ment – Cleanliness; (4) Human Relations; (5) Technical-Scientific Quality; (6) Efficiency; (7) Efficacy; (8) Equity; (9) Acceptability.
The qualitative part of this study consisted of evaluation, by means of an open question, with the purpose of verifying the main reasons for satisfaction and dissatisfaction with the services provided by the CEOs (“What is the reason why you are dissatisfied or satisfied with the services provided by the CEO?”). All the interviews were recorded after obtaining authorization from the interviewees. These were later transcribed; however, when the interviewees did not authorize recording, the researcher transcribed the speeches during the course of the interview.
Manner of Analyzing the Results
The quantitative data were first digitized on an Excel spreadsheet, and afterwards exported to the Program R, version 3.2.5. Initially, a descriptive analysis was made by means of frequency of distribution of the sample among the study variables. Afterwards the χ 2 and exact Fisher statistical tests were used, with a level of significance of 5%, to evaluate whether there were any differences in the study variables among the different CEOs.
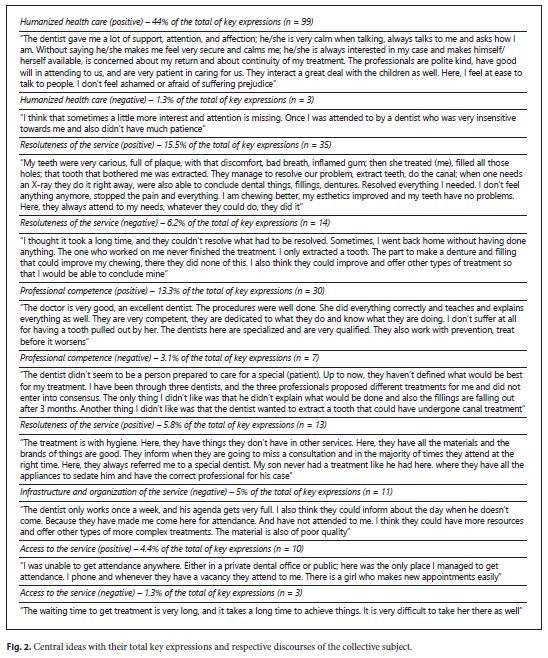
The content of the qualitative data was analyzed by means of the discourse of the collective subject 18 for interpreting the interviewees’ responses, performed by two trained researchers. The researchers read, transcribed, and identified the topics that arose in the data of each interview. The phrases, words, or expressions that referred to satisfaction or dissatisfaction with the services provided by the CEOs were underlined in the transcription. The level of agreement between the examiners during categorization was good (85.7%). This was calculated based on the selection of key expressions contained in the interviewees’ responses, and their respective classification according to the central ideas (Figure 2 ).
Results
Social Characterization and Types of Special Needs
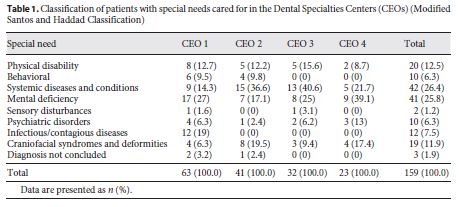
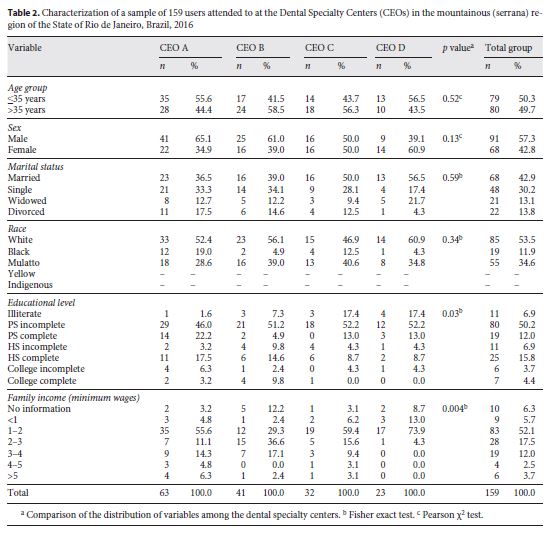
With the use of the modified Santos and Haddad classification 19, the results showed that the systemic conditions or diseases and metal deficiency were the most prevalent, with 26.4 and 25.8% of the total number of individuals interviewed at the CEOs, respectively (Table 1 ). Sociodemographic characterization of the sample is shown in Table 2 , in which significant differences were observed among the CEOs relative to educational level ( p = 0.03) and family income ( p = 0.004).
Integrality of the Oral Health Care Network
As far as this parameter was concerned, a frail system of reference and counter reference was observed, considering that in the total group, approximately 82.5% of the patients arrived at the CEOs without having been referred or referenced by primary oral health care professionals. There were significant differences between the CEOs in this variable ( p < 0.01), with CEO D presenting the best results relative to the integrality of the oral health care network (Table 3 ).
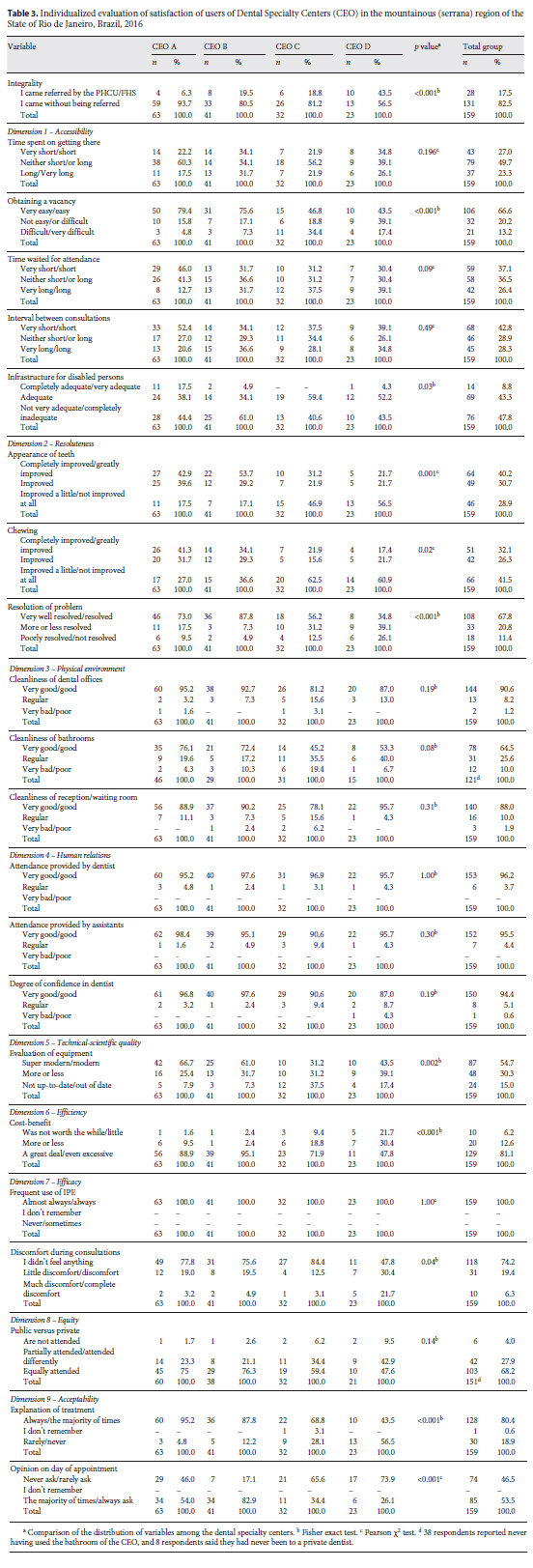
Quantitative Evaluation of Quality Dimension by the Total Group
The results of the quality dimensions in the total group and per CEO are shown in Table 3 .
Positive evaluations were observed in all the variables of the quality dimensions, with the exception of the dimension accessibility, which presented a negative evaluation for the variables “time spent on arriving at the CEO,” “waiting for attendance,” and “interval between consultations.” However, this same dimension revealed positive results for the variables “obtaining a vacancy” and “infrastructure for disabled persons,” with 66.6 and 52.1% respectively, of the interviewees providing positive evaluation of the service. The variable “infrastructure for disabled persons” was evaluated positively when the responses “Completely adequate/very adequate” and “Adequate” were totaled.
However, in the dimension “resoluteness,” all the variables (appearance of the teeth, chewing, and resolution of the problem) presented positive evaluations in the total group. The variables “appearance of the teeth” and “chewing” demonstrated 70.9 and 58.4% of favorable responses (“Completely improved/much improved” and “Improved”), respectively.
Regarding the physical environment dimension – cleaning, all the variables also showed positive evaluations (very good/good) by the majority of the interviewees. The variables cleaning of the dental offices, bathrooms, reception/waiting room were found to present positive evaluation in 90.6, 64.5, and 88% of the study participants, respectively.
Within this same trend towards positive evaluation of the service, the authors could find that in the human relations dimension, the variables “attendance provided by the dentist,” “attendance provided by the assistant,” and “degree of confidence in the dentist” were evaluated as “very good/good” by 96.2, 95.5, and 94.4% of the individuals participating in this study, respectively.
Generally speaking, the technical-scientific quality dimensions of the equipment, efficiency, efficacy, equity, and acceptability followed this trend towards positive evaluation with, for example, 74.2% of the patients reporting that they felt no discomfort whatever during the course of the consultation; 68.2% of the respondents declaring they had their needs equally met in the public and private service; 80.4% saying that the dentist always, or in the majority of times, explained the proposed treatment; and 53.5% of the individuals reporting that the CEO team always or in the majority of times asked for their opinion relative to the best day for making the appointment for the consultation, among other variables.
Quantitative Evaluation of the Quality Dimension per Dental Specialty Center
The comparative results among the CEOs showed that in general, significant differences were found among them with regard to the following dimensions/variables: accessibility/obtaining a vacancy ( p < 0.001), accessibility/infrastructure for disabled persons ( p = 0.03), resoluteness/appearance of the teeth ( p = 0.001), resoluteness/chewing ( p = 0.02), resoluteness/resolution of the problem ( p < 0.001), technical-scientific quality of the items of equipment/equipment ( p = 0.002), efficiency/cost-benefit ( p < 0.001), efficacy/discomfort during consultations ( p = 0.04), and acceptability/explanation of treatment and opinion about the day for making the appointment ( p < 0.001). In general, CEO B presented the worst evaluation in the variable infrastructure for disabled persons of the dimension accessibility. CEO C presented the worst results in the dimensions/variables: accessibility/obtaining a vacancy; resoluteness/appearance of the teeth and chewing; technical-scientific dimension/dental office equipment, and acceptability/opinion about making the appointment for consultation. In CEO D, the authors observed the worst performance of user satisfaction in the following dimensions/variable: resoluteness/appearance of the teeth and chewing; resoluteness/resolution of the problem; technical-scientific dimension/dental office equipment; efficiency/cost-benefit; efficacy/discomfort during consultations; acceptability/explanation of treatment and opinion about making the appointment for consultation.
~Qualitative Evaluation of the CEOs by the Total Group
After analysis and interpretation of the qualitative data, the central ideas that arose for expressing satisfaction or dissatisfaction with the services provided by the CEOs were the following: humanized health care; resoluteness of the service; competence of the professionals; infrastructure and organization of the service; and access to the service (Figure 2 ). Transcription of the 159 interviews presented a total of 225 key expressions containing positive (83.6%) or negative (16.4%) connotations, and that fitted in with the central ideas of evaluation of the services.
The central ideas most frequently mentioned by the respondents to express their satisfaction with the services were the following: humanized health care (44% of the responses), followed by resoluteness of the services (16% of the responses). The most frequent central ideas for expressing dissatisfaction with the services were the following: resoluteness (5.8% of the responses), followed by infrastructure and organization of the services (5% of the responses).
Analysis of the results per establishment showed that in all the CEOs the most frequent central ideas for users’ satisfaction were humanized health care and resoluteness of the services. This trend was not observed only in CEO C because the most frequent central ideas in this establishment were humanized health care and competence of the professionals.
In CEOs A and B, the authors also observed that all the central ideas presented a higher percentage of positive than negative evaluations, differently from CEOs C and D. In CEO C, the negative evaluations exceeded the positive in the central ideas of infrastructure and organization of the services, and access to the services. In CEO D, the central ideas competence of the professionals and infrastructure, and organization of the services also presented more negative than positive evaluations. The DCS of each central idea is shown in Figure 2 .
The authors found that the qualitative results corroborated the quantitative results of this study.
Discussion
From the foregoing results shown, the authors were able to verify that in general, there was a high degree of satisfaction with the services provided by the CEOs belonging to CIS-Serra among the patients with special needs or the persons who accompanied them.
Relative to the integrality of the system of reference and counter reference of the oral health care network of the studied municipalities, frail articulation was observed between primary and secondary care. Possible justifications for this finding may be pointed out as being: lack of knowledge of primary care professionals as regards the Ministry of Health protocols for referral of patients with special needs to secondary care, deficient professional training of the general clinician for attending to this type of patient, and the very lack of information by the users about how the oral health care network functions, seeing that they use the CEO as a port of entry to SUS in the majority of occasions. This fact deserves to be emphasized, seeing that the users’ port of entry into SUS should be primary care, in which the individual receives assistance, guidance, and referral to secondary or tertiary care in case of need. This integrality within the health care network allows a rational distribution of the users in the different services, thereby avoiding overload at any level of care by SUS 20. However, the study of Casotti et al.21. revealed the existence of reference and counter reference protocols for referring patients to the CEOs in approximately 62.7% of the oral health teams in the southeastern regions, which counted on this service in their oral health care network. This could suggest that these protocols are perhaps not being duly used by the professionals.
Here, the high prevalence of patients with systemic conditions and diseases being cared for by the CEOs should also be emphasized. Although this group of patients present the need for special care, they should preferably be attended to in primary care, and only when necessary, must they be referred to the CEO with a professional report from primary care, justifying this referral. Moreover, the list of basic procedures for the care of patients with special needs stated in Administrative Ruling 1464/GM of 2011 is destined exclusively for those patients who do not cooperate with having treatment performed and those who are severely compromised. It is mandatory for these patients to be attended to by a specialist 1.
In the quality dimensions evaluated, accessibility was the variable that presented the worst results in the total group of this study. This quality dimension is extremely important, seeing that the factor that most influences the satisfaction of users with the services is adequate access to these services 22. The variable “time spent to arrive at the CEO” presented negative results; however, this finding was expected, and could not be considered bad, because, considering that the CEOs are centers of reference, they must not necessarily be close to the population’s residences. Their geographical localization must take into account only the question of economy of scale. Obtaining a vacancy for attendance consists of one of the main means for the user to have adequate access and first contact with the health services, and this must be considered in the organization and evaluation of these services 23. The time spent waiting for attendance was also one of the obstacles found by users and was reported in the study of Franco and Campos 11. In this sense, this aspect deserves special attention, considering that the population of this study consisted of patients with special needs who, in some cases, had different needs (food, hygiene) in comparison with the general population 24. Another factor to be pointed out for better integration into and access to health services by the population under study is the existence of infrastructure of these establishments with conditions of safety and use, in addition to complete independence by persons with disabilities or reduced mobility. Law decree No. 5.296/2004, which regulates Laws No. 10.048/2000 and 10.098/2000, guarantees priority attendance to persons with disability or reduced mobility in public offices and institutes general rules and basic criteria for the promotion of accessibility to these establishments by these individuals 25. The infrastructure geared for the attendance to disabled persons in the CEOs was considered satisfactory by the majority of individuals in this study, with the exception of CEO B. These results corroborated the findings of the study of Machado and Nogueira 26 who revealed the absence of problems related to accessibility by users with disabilities, in relation to the infrastructure of a physical therapy clinic. Thus, all the factors related above deserve to be taken into consideration in the management and organization of the studied CEOs.
The data of this study pointed out a high degree of resoluteness in CEOs A and B, which may be observed in the discourse with reference to the central ideas, with the second most mentioned being in relation to satisfaction, and the first in relation to dissatisfaction with the services, which is in agreement with the quantitative results of the studies of Lima et al.27 and Magalhães et al. 28.
The human relations between professionals and users of the CEOs were also reasons for satisfaction by the participants of this research, both quantitatively and qualitatively, as was the case in other studies using the same instruments of evaluation ( 27 29 ). The basis for patient satisfaction consists of the manner in which the user is treated in the health services. Cold, dehumanized relations distance patients from professionals and make it difficult for them to adhere to treatment. The establishment of ties between professionals and patients and their families presupposes the development of harmonious and humanized relations between the two parties, as well as the appreciation of the subjective being, taking into consideration psychosocial aspects in their treatment, and not only traditional scientific knowledge based only on the biological dimension of the health-disease process. These findings were clearly shown in the study, seeing that approximately 44% of the key expressions contained in the discourses for expressing satisfaction of the interviewees with the service were related to the central idea of “humanized health care.” This same trend was strongly observed in the quantitative part of the study, in which the evaluation of the dimension/variable “human relations/attention provided by the dentist” was positively evaluated by 96.2% of the users/and those who accompanied them. This being so, the human dimension of treatment must be appreciated as much as the technical dimension ( 14 , 30 ).
Relative to the dimension efficiency, the authors observed a high percentage of individuals judging that it was worthwhile to seek the CEO to have their dental treatment performed, or that of the persons who accompanied them. According to Magalhães et al.28, these data may be explained by the fact that the secondary care services offer more complex, expensive treatments to which a large part of the population find difficulty in gaining access.
Another dimension that deserved emphasis in this study was that of equity. This showed that the majority of individuals considered that their needs were met equally when the public service (CEO) was compared with private service. This is extremely positive, seeing that the Brazilian media frequently tries to propagate the idea that the public health services present a worse level of quality than the private services 31.
The present study demonstrated the importance of professional interaction with users, taking into consideration their needs and choices, placing value on their independence in health care and exchange of knowledge between the social actors involved in this process 32. This finding could be proved in the findings of the dimension accessibility, in which the majority of the individuals interviewed reported that the dentist always, or the majority of the times explained the proposed treatment, and the question about what the best day and time were for making the appointment for consultations. This quality dimension has a concept that is broad in scope, requiring greater depth of the instruments for evaluating it.
The authors also found greater satisfaction of the users with special needs in the CEOs that adhered to the Network of Care for Persons with Disabilities (NCPD), which could be related to a more mature and organized management of these municipalities, and that for this reason, they seek state and federal resources to promote improvement in the offer of their services. These findings reinforce the need for greater stimulus on the part of the State Government and State and Regional Bipartite Interactive Committees to realize the regionalization of secondary oral health care and adhesion to public health policies for persons with disabilities in the municipalities belonging to CIS-Serra ( 33 , 34 ).
The present study had some possible inherent limitations regarding the evaluation of quality of public health services through users’ perception. The level of satisfaction was high in the large portion of the CEOs, and some factors may have influenced these results. Among these are the reluctance of users to suffer reprisals due to a negative evaluation of the service 35 and gratitude (gratitude bias) ( 36 , 37 ) for the attendance received and access to the services, seeing that the population of patients with special needs have difficulty in gaining access to the services, for either socioeconomic, geographic, or organizational reasons 24. This difficult access makes it impossible for individuals to have their dental needs adequately met.
However, the positive points may also be considered, seeing that this study was probably the first to evaluate the services of secondary care in relation to the attendance to patients with special needs in Brazil; and the first study to evaluate quality through the perception of users in the Dental Specialty Centers in the mountainous (serrano) region of the State of Rio de Janeiro, Brazil. Moreover, the dropout of participants from the study was very small; therefore, the sample was representative.
Lastly, the authors point out the relevance of this study for understanding the dimensions of the quality of Brazilian dental services in secondary care from the perception of users with special needs. The incentive provided by this evaluation to the managers and health teams for improvement and enhancement of their services is a trend followed by one of the main national programs to evaluate the quality of public health services (PMAQ-CEO) ( 38 ).
The CEOs of the mountainous (serrano) region of the State of Rio de Janeiro are services that present particularities and differences when they are evaluated individually.
The results of this research emphasized the importance of human relations between professionals and patients in the quality of health care of individuals with special needs, seeing this as one of the main reasons for the satisfaction of these users.
In view of this, it is possible to conclude that there is a constant need for managers and health teams to perform quality evaluation of their services from the users’ perception, thus enabling social participation in SUS, a principle recommended by Brazilian sanitary reform.
This research was approved by the Research Ethics Committee of the “Universidad Federal Fluminense” – Nova Friburgo complex, and obtained a report favorable to conducting the study, by means of Protocol CAEE No. 51509015.2.0000.5626, and was in compliance with Resolution 466/12 of the National Health Council.
REFERENCES
1 Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde bucal. Brasília: Ministério da Saúde; 2008 . (Cadernos de Atenção Básica, 17).
2 World Health Organization . The World Oral Health Report 2003: continuous improvement of oral health in the 21st century: the approach of the WHO Global Oral Health Programme . Geneva : WHO/NMH/NPH/ORH ; 2003 . [ Links ]
3 IBGE . Características gerais da população . Censo demográfico 2000 . Rio de Janeiro : IBGE ; 2003 . [ Links ]
4 Brasil. Ministério da Saúde. Programa Nacional de Assistência Odontológica Integrada ao Paciente Especial. Brasília: Ministério da Saúde, SNAS; 1992 . [ Links ]
5 Carneiro N Junior , Silveira C . Organização das práticas de atenção primária em saúde no contexto dos processos de exclusão/inclusão social . Cad Saude Publica . 2003 ; 19 ( 6 ): 1829 – 35 . http://dx.doi.org/10.1590/S0102-311X2003000600026
6 Chagas AM . Avanços e impedimentos para a construção de uma política social para pessoas com deficiência ( dissertação de mestrado ) Brasília : Universidade de Brasília ; 2006 .
7 Decreto Legislativo nº 186, de 09 de julho de 2008: Decreto nº 6.949, de 25 de agosto de 2009. Brasil. Convenção sobre os Direitos das Pessoas com Deficiência: Protocolo Facultativo à Convenção sobre os Direitos das Pessoas com Deficiência: 4ª ed., rev. e atual. Brasília: Secretaria de Direitos Humanos; 2010 .
8 Portaria nº. 599. Ministério da Saúde. Define a implantação de especialidades odontológicas (CEO) e de laboratórios regionais de próteses dentárias (LRPDs) e estabelece critérios, normas e requisitos para seu credenciamento. Diário Oficial da União. 2006 ; 24 março.
9 Portaria nº. 835. Ministério da Saúde. Institui incentivos financeiros de investimento e de custeio para o componente atenção especializada da rede de cuidados à pessoa com deficiência no âmbito do Sistema Único de Saúde. Diário Oficial da União. 2012 ; 25 abril.
10 Franco SC , Campos GW . Acesso a ambulatório pediátrico de um hospital universitário . Rev Saude Publica . 1998 a Aug ; 32 ( 4 ): 352 – 60 . http://dx.doi.org/10.1590/S0034-89101998000400007
11 Franco SC , Campos GW . Avaliação da qualidade de atendimento ambulatorial em pediatria em um hospital universitário . Cad Saude Publica . 1998 b Apr ; 14 ( 1 ): 61 – 70 . http://dx.doi.org/10.1590/S0102-311X1998000100014
12 Kloetzel K , Bertoni AM , Irazoqui MC , Campos VP , Santos RN . Controle de qualidade em atenção primária à saúde. I A satisfação do usuário . Cad Saude Publica . 1998 Jul-Sep ; 14 ( 3 ): 623 – 8 . http://dx.doi.org/10.1590/S0102-311X1998000300020
13 Assunção MC , Santos Id , Gigante DP . Atenção primária em diabetes no Sul do Brasil: estrutura, processo e resultado . Rev Saude Publica . 2001 Feb ; 35 ( 1 ): 88 – 95 . http://dx.doi.org/10.1590/S0034-89102001000100013
14 Ramos DD , Lima MA . Acesso e acolhimento aos usuários em uma unidade de saúde de Porto Alegre, Rio Grande do Sul, Brasil . Cad Saude Publica . 2003 Jan-Feb ; 19 ( 1 ): 27 – 34 . http://dx.doi.org/10.1590/S0102-311X2003000100004
15 Fernandes LMAG : Validação de um instrumento para avaliação da satisfação dos usuários, com os serviços públicos de saúde bucal (tese de doutorado). Camaragibe: Faculdade de Odontologia. Universidade de Pernambuco; 2002 .
16 Donabedian A . The seven pillars of quality . Arch Pathol Lab Med . 1990 Nov ; 114 ( 11 ): 1115 – 8 .
17 Edwards C , Staniszewska S . Accessing the user’s perspective . Health Soc Care Community . 2000 Nov ; 8 ( 6 ): 417 – 24 . http://dx.doi.org/10.1046/j.1365-2524.2000.00267.x
18 Lefèvre F , Lefèvre AM , Teixeira JJ . O discurso do sujeito coletivo: uma nova abordagem metodológica em pesquisa qualitativa . Caxias do Sul : EDUCS ; 2000 . [ Links ]
19 Santos MT , Haddad AS . Quem são os pacientes com necessidades especiais? In: Cardoso RJ , Machado ME , editors . Odontologia: arte e conhecimento . São Paulo : Artes Médicas ; 2003 . pp. 263 – 8 .
20 Pucca JR . Por um Brasil sorridente . Rev ABO Nac . 2004 ; 12 : 73 – 9 .
21 Casotti E , Contarato PC , Fonseca AB , Borges PK , Baldani MH . Atenção em saúde bucal no Brasil: uma análise a partir da Avaliação Externa do PMAQ-AB . Saúde Debate . 2014 ; 38 special : 140 – 57 . http://dx.doi.org/10.5935/0103-1104.2014S011
22 Bamise C , Bada T , Bamise F , Ogunbodede E . Dental care utilization and satisfaction of residential university students . Libyan J Med . 2008 Sep ; 3 ( 3 ): 140 – 3 . http://dx.doi.org/10.3402/ljm.v3i3.4778
23 Frenk J . El concepto y la medición de accesibilidad . Salud Publica Mex . 1985 Sep-Oct ; 27 ( 5 ): 438 – 53 .
24 Castro SS , Lefèvre F , Lefèvre AM , Cesar CL . Acessibilidade aos serviços de saúde por pessoas com deficiência . Rev Saude Publica . 2011 ; 45 ( 1 ): 99 – 105 . http://dx.doi.org/10.1590/S0034-89102010005000048
25 Decreto nº 5.296 de 02 de dezembro de 2004. Brasil. DOU de 03/12/ 2004 . Acesso em: 20 out. 2005.
26 Machado NP , Nogueira LT . Avaliação da satisfação dos usuários de serviços de Fisioterapia . Rev Bras Fisioter . 2008 ; 12 ( 5 ): 401 – 8 . http://dx.doi.org/10.1590/S1413-35552008000500010
27 Lima AC , Cabral ED , Vasconcelos MM . Satisfação dos usuários assistidos nos Centros de Especialidades Odontológicas do Município do Recife, Pernambuco, Brasil . Cad Saude Publica . 2010 May ; 26 ( 5 ): 991 – 1002 . http://dx.doi.org/10.1590/S0102-311X2010000500021
28 Magalhães BG , Oliveira RS , Góes PS , Figueiredo N . Avaliação da qualidade dos serviços prestados pelos Centros de Especialidades Odontológicas: visão dos usuários . Cad Saude Colet . 2015 ; 23 ( 1 ): 76 – 85 . http://dx.doi.org/10.1590/1414-462X201500010013
29 Marcinowicz L , Chlabicz S , Grebowski R . Patient satisfaction with healthcare provided by family doctors: primary dimensions and an attempt at typology . BMC Health Serv Res . 2009 Apr ; 9 ( 1 ): 63 . http://dx.doi.org/10.1186/1472-6963-9-63 [ Links ]
30 Backes DS , Koerich MS , Rodrigues AC , Drago LC , Klock P , Erdmann AL . O que os usuários pensam e falam do Sistema Unico de Saúde? Uma análise dos significados à luz da carta dos direitos dos usuários . Cien Saude Colet . 2009 May-Jun ; 14 ( 3 ): 903 – 10 . http://dx.doi.org/10.1590/S1413-81232009000300026
31 Souza EM . A satisfação dos idosos com os serviços de saúde: um estudo de prevalência e de fatores associados em Taguatinga, Distrito Federal ( dissertação de mestrado ) Brasília : Faculdade de Ciências da Saúde. Universidade de Brasília ; 1997 .
32 Pinto BM , Machado CJ , Sá EO . Características necessárias de um profissional de saúde que trabalha com pacientes portadores de necessidades especiais: um contraste de visões de profissionais e alunos de odontologia, pais e cuidadores . Belo Horizonte : Faculdade de Odontologia, Universidade Federal de Minas Gerais ; 2004 .
33 Nicoletto SC , Cordoni L Jr , Costa NR . Consórcios Intermunicipais de Saúde: o caso do Paraná, Brasil . Cad Saude Publica . 2005 Jan-Feb ; 21 ( 1 ): 29 – 38 . http://dx.doi.org/10.1590/S0102-311X2005000100004
34 Neves LA , Ribeiro JM . Consórcios de saúde: estudo de caso exitoso . Cad Saude Publica . 2006 Oct ; 22 ( 10 ): 2207 – 17 . http://dx.doi.org/10.1590/S0102-311X2006001000027
35 Andrade KL , Ferreira EF . Avaliação da inserção da odontologia no Programa de Saúde da Família de Pompéu/MG: a satisfação do usuário . Cien Saude Colet . 2006 ; 11 ( 1 ): 123 – 30 . http://dx.doi.org/10.1590/S1413-81232006000100020
36 Traverso-Yépez M , de Morais NA . Reivindicando a subjetividade dos usuários da Rede Básica de Saúde: para uma humanização do atendimento . Cad Saude Publica . 2004 Jan-Feb ; 20 ( 1 ): 80 – 8 . http://dx.doi.org/10.1590/S0102-311X2004000100022
37 Vaitsman J , Andrade GR . Satisfação e responsividade: formas de medir a qualidade e a humanização da assistência à saúde . Cien Saude Colet . 2005 ; 10 ( 3 ): 599 – 612 . http://dx.doi.org/10.1590/S1413-81232005000300017
38 Portaria nº 1.599. Ministério da Saúde. Dispõe sobre o Programa de melhoria do acesso e qualidade dos centros de especialidades odontológicas (PMAQ-CEO). Diário Oficial da União 2015 ; 30 set.
Received: July 24, 2018. Accepted: September 15, 2018
The authors declare that there are no known conflicts of interest associated with the publication of this manuscript and there has been no significant financial support for this work that could have influenced its outcome. Indeed, the authors declare that this research was developed with own financial resources.

