










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.27 no.2 Lisboa abr. 2020
https://doi.org/10.1159/000502982
CLINICAL CASE STUDY
Extensive Refractory Perineal Pyoderma Gangrenosum Treated with Infliximab, Fecal Diversion, and Negative-Pressure Wound Therapy
Extenso pioderma gangrenoso perineal
Mafalda Sousaa, Manuel António Camposb, Ana Cristina Sousab, Jorge Lopesb, Adélia Rodriguesa, João Carvalhoa
aGastroenterology Department, Centro Hospitalar de Vila Nova de Gaia e Espinho, Vila Nova de Gaia, Portugal; bDermatology Department, Centro Hospitalar de Vila Nova de Gaia e Espinho, Vila Nova de Gaia, Portugal
* Corresponding author.
ABSTRACT
Background: Pyoderma gangrenosum (PG) is a rare and difficult-to-diagnose disease that often associates with inflammatory bowel disease. Case: We present a case of a 57-year old female with ulcerative colitis receiving 5-ASA who presented with rapidly progressive ulcers in the right foot and on the inside of the thigh, extending from the left large vaginal lip to the perianal area, compatible with PG. She was initially treated with corticosteroids with no response. After multidisciplinary consultation, it was decided to initiate infliximab 5 mg/kg, and to perform ileostomy for fecal diversion and negative-pressure wound therapy. The patient presented with marked improvement of the lesions, being discharged after 2 months and demonstrating almost complete resolution of the lesions within 4 months. Conclusion: Due to the rarity of PG, there is no evidence of the optimal management. The role of surgery is controversial as PG lesions can demonstrate pathergy and theoretically could worsen with surgical intervention. In this case it was decided based on the extent of the lesions and the experience in other septic/ulcerative perianal conditions.
Keywords: Pyoderma gangrenosum, Infliximab, Fecal diversion, Negative-pressure wound therapy
RESUMO
Introdução: O pioderma gangrenoso (PG) é uma doença rara e de difícil diagnóstico, que frequentemente se associa à doença inflamatória intestinal. Caso: Apresentamos um caso de uma mulher de 57 anos de idade com colite ulcerosa sob 5-ASA que recorreu ao serviço de urgência pelo aparecimento de úlceras rapidamente progressivas no pé direito e no interior da coxa, estendendo-se desde o grande lábio vaginal esquerdo até à área perianal, compatível com PG. A doente foi inicialmente tratada com corticosteroides, sem resposta. Após consulta multidisciplinar, optou-se por iniciar o infliximab 5 mg/kg, realizar ileostomia para desvio fecal e iniciar terapia de vácuo com pressão negativa. A doente apresentou melhoria marcada das lesões tendo tido alta após 2 meses e demonstrando resolução quase completa das lesões aos 4 meses. Conclusão: Devido à raridade do PG, não há evidências de qual a abordagem ideal. O papel da cirurgia é controverso, pois as lesões do PG podem demonstrar patergia e teoricamente poderiam piorar com a intervenção cirúrgica. Neste caso, a opção cirúrgica foi tomada com base na extensão das lesões e na experiência em outras condições perianais sépticas/ulcerativas.
Palavras-Chave: Pioderma gangrenoso, Infliximab, Ileostomia, Terapia de vácuo com pressão negativa
Introduction
Pyoderma gangrenosum (PG) is a rare ulcerating skin disease often associated with inflammatory bowel disease (IBD), with an estimated incidence of 3–10 cases per million population per year [1, 2]. The etiology of PG is poorly understood but probably involves an interplay of genetic and environmental factors with loss of innate immune regulation and altered neutrophil chemotaxis [2, 3]. Diagnosis is challenging since this condition can exhibit different clinical presentations (namely in morphology and affected sites), may overlap with other conditions, and is associated with several systemic diseases [1, 4].
Recently a group of international experts defined criteria for its diagnosis – the Delphi criteria – yielding a sensitivity and specificity of 86 and 90%, respectively. They include 1 major criterion (biopsy with neutrophilic infiltrate) and 8 minor criteria (exclusion of infection on histology; pathergy; personal history of IBD or inflammatory arthritis; papule, pustule or vesicle that rapidly ulcerates; peripheral erythema, undetermined borders, and tenderness at the site of ulceration; multiple ulcerations [at least one occurring on an anterior lower leg]; cribriform or wrinkled paper scars at healed ulcer sites; and a decrease in ulcer size after immunosuppressive treatment) [4].
Case Report
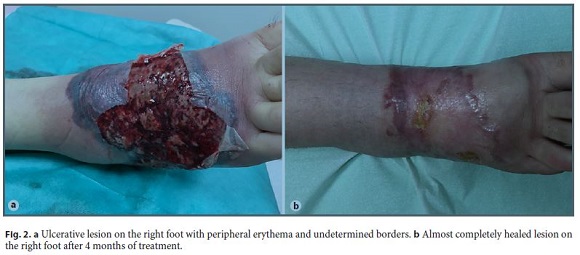
We report a case of a 57-year-old female patient receiving 5-ASA who was diagnosed with ulcerative colitis (UC) 8 years ago. She was admitted to the emergency department due to the appearance of a profound ulcer on the inside of the thigh, extending from the left large vaginal lip to the perianal area (Fig. 1a) and a rapidly progressive painful ulcer in the right foot with peripheral erythema and undetermined borders (Fig. 2a). She had two bowel movements/ day with blood in the stool, and sigmoidoscopy showed lesions compatible with Mayo 3 UC.

Biopsy of the lesion from the foot was obtained, showing neutrophilic infiltration compatible with PG. Infections were excluded by serology and skin biopsy. The patient performed a pelvic computed tomography scan that showed a perianal collection lateralized to the left with extension to the vulva with fistulization of the large left vulvar lip and the possibility of rectal fistulization.
Based on the diagnosis of PG, the patient was started on corticosteroids (oral prednisolone 1 mg/kg/day followed by endovenous hydrocortisone 400 mg/day) with no significant clinical improvement. Taking into account the extent of the perineal lesions and after multidisciplinary consultation (gastroenterology, dermatology, and surgery) it was decided to initiate infliximab 5 mg/ kg and to perform derivation ileostomy and negative-pressure wound therapy (NPWT). There was marked improvement of the lesions, and the patient was discharged after 2 months. At 4 months, there was almost complete resolution of the lesions (Fig. 1b, Fig. 2b).
Considering the excellent evolution of the lesion with complete healing and also the healing of the colonic mucosa on follow-up colonoscopy, the patient was proposed for reconstruction of the intestinal transit, which was uneventful.
b>Discussion
PG algorithm treatment is controversial and remains poorly characterized due to limited knowledge of its pathophysiology combined with its rarity [1, 2, 5].
It is generally based on wound care, analgesia, topical or intralesional therapy with corticosteroids, and systemic therapy with corticosteroids, cyclosporine, or anti-TNF agents. A randomized, placebo-controlled study found that infliximab had a beneficial clinical response in 69% of the patients and a remission rate of 21% at week 6 [6]. A systematic review with 60 cases found that 92% of the patients had response to anti-TNF [5].
The role of surgical treatment in PG is controversial as 25–50% of the PG lesions demonstrate pathergy and theoretically could worsen with surgical intervention [3].
Nevertheless, NPWT has demonstrated efficacy in the treatment of chronic wounds in a variety of circumstances. The rational of the use of subatmospheric pressure therapy includes increased tissue perfusion, control of the advancing ischemic process, production of a healthy granular wound bed, reduced bacterial load, and pain relief. Some reports show its safety and efficacy in PG, but only if combined with proper immunosuppression.[7–10].
Ileostomy for fecal diversion as in other perianal septic and ulcerative conditions (such as perianal Crohns disease or Fourniers gangrene) is also controversial but was made to decrease wound contamination and to promote faster wound healing, especially taking into account the possibility of fistulization to the rectum [11].
In this study, we show an extensive perineal PG in a patient with UC that was successfully treated with infliximab, derivation ileostomy, and NPWT.
References
1 Plumptre I, Knabel D, Tomecki K. Pyoderma Gangrenosum: A Review for the Gastroenterologist. Inflamm Bowel Dis. 2018 Nov;24(12):2510–7.
2 Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018 Mar;14(3):225–33.
3 Ahronowitz I, Harp J, Shinkai K. Etiology and management of pyoderma gangrenosum: a comprehensive review. Am J Clin Dermatol. 2012 Jun;13(3):191–211.
4 Maverakis E, Ma C, Shinkai K, Fiorentino D, Callen JP, Wollina U, et al. Diagnostic Criteria of Ulcerative Pyoderma Gangrenosum: A Delphi Consensus of International Experts. JAMA Dermatol. 2018 Apr;154(4):461–6.
5 Agarwal A, Andrews JM. Systematic review: IBD-associated pyoderma gangrenosum in the biologic era, the response to therapy. Aliment Pharmacol Ther. 2013 Sep;38(6):563–72.
6 Brooklyn TN, Dunnill MG, Shetty A, Bowden JJ, Williams JD, Griffiths CE, et al. Infliximab for the treatment of pyoderma gangrenosum: a randomised, double blind, placebo controlled trial. Gut. 2006 Apr;55(4):505–9.
7 Geller SM, Longton JA. Ulceration of pyoderma gangrenosum treated with negative pressure wound therapy. J Am Podiatr Med Assoc. 2005 Mar-Apr;95(2):171–4.
8 Fraccalvieri M, Fierro MT, Salomone M, Fava P, Zingarelli EM, Cavaliere G, et al. Gauzebased negative pressure wound therapy: a valid method to manage pyoderma gangrenosum. Int Wound J. 2014 Apr;11(2):164–8.
9 Pichler M, Thuile T, Gatscher B, Tappeiner L, Deluca J, Larcher L, et al. Systematic review of surgical treatment of pyoderma gangrenosum with negative pressure wound therapy or skin grafting. J Eur Acad Dermatol Venereol. 2017 Feb;31(2):e61–7.
10 Pichler M, Larcher L, Holzer M, Exler G, Thuile T, Gatscher B, et al. Surgical treatment of pyoderma gangrenosum with negative pressure wound therapy and split thickness skin grafting under adequate immunosuppression is a valuable treatment option: case series of 15 patients. J Am Acad Dermatol. 2016 Apr;74(4):760–5.
11 Lin HC, Chen ZQ, Chen HX, He QL, Liu ZM, Zhou ZY, et al. Outcomes in patients with Fourniers gangrene originating from the anorectal region with a particular focus on those without perineal involvement. Gastroenterol Rep (Oxf). 2019 Jun;7(3):212–7.
Statement of Ethics
Informed patient consent was obtained for publication of the case details.
Disclosure Statement
The authors have no conflicts of interest.
* Corresponding author.
Mafalda Sousa
Gastroenterology Department, Centro Hospitalar de
Vila Nova de Gaia e Espinho, Rua Conceição Fernandes, s/n
PT–4434-502 Vila Nova de Gaia (Portugal)
E-Mail mafalda_m_p_sousa@hotmail.com
Received: June 6, 2019; Accepted after revision: July 27, 2019
Author Contributions
M.S. wrote the manuscript, M.A.C., A.C.S., J.L., A.R., and J.C. reviewed the manuscript and followed the patient.

