










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.26 no.2 Lisboa abr. 2019
https://doi.org/10.1159/000487963
ORIGINAL ARTICLE
Increased Risk of Spontaneous Bacterial Peritonitis in Cirrhotic Patients Using Proton Pump Inhibitors
Risco Aumentado de Peritonite Bacteriana Espontânea em Doentes Cirróticos Medicados com Inibidores da Bomba de Protões
Abdel-Naser Elzoukia,b, Nadia Neffatia, Fatma A. Rasoula, Ali Abdallaha, Muftah Othmana, Abdelkarim Wanessa
aDepartment of Medicine, Hamad General Hospital, Hamad Medical Corporation, Doha, Qatar; bWeill Cornell Medical College, Doha, Qatar
* Corresponding author.
ABSTRACT
Background: The association between bacterial infections and proton pump inhibitors (PPIs) has recently been studied with debatable results. Aim: The aim of this study was to investigate the relationship between PPIs and the development of spontaneous bacterial peritonitis (SBP) or other bacterial infections in cirrhotic patients. Materials and Methods: Consecutive cirrhotic patients hospitalized from 2007 through 2012 to Hamad General Hospital–, Doha, Qatar, were enrolled and classified as PPI users or non-users according to PPI consumption in the 90 days prior to hospitalization. Cirrhosis was clinically diagnosed by a combination ofphysical, biochemical, radiological, and endoscopic findings, or by liver biopsy. Results: A total of 333 patients were included in this study, of whom 171 (51.4%) used PPIs and 162 (48.6%) did not use PPIs. PPI users were significantly older in age (p = 0.001). There was no statistical difference between the 2 groups in sex distribution and etiology of cirrhosis (p > 0.05 for both parameters). PPI users had a significantly higher incidence of overall bacterial infection (38%) than non-PPI users (13.6%), p = 0.0001. Statistical significance is observed specifically for SBP and chest infection (p = 0.0006 and p = 0.01, respectively). In multivariate analysis, older age (> 60 years; OR = 1.246, 95% CI 1.021–08.486; p = 0.02), and PPI use (OR = 2.149, 95% CI 1.124–06.188; p = 0.01) were independent predicting factors for SBP and overall bacterial infection. Conclusion: The present study shows that PPI use, as well as older age (> 60 years), was an independent predicting factor for the development of overall infection and SBP in hospitalized cirrhotic patients. Unless it is indicated, PPI therapy should be avoided in this group of patients, particularly in those older than 60 years of age.
Keywords: Acid suppressive medications, Bacterial infection, Infection, Liver cirrhosis, Qatar
RESUMO
Introdução: A associação entre infeções bacterianas e os Inibidores da bomba de protões (IBPs) tem vindo a ser estudada com resultados discutíveis. Objetivo: O objetivo deste estudo foi investigar a relação entre IBPs e o desenvolvimento de peritonite bacteriana espontânea (PBE) ou outras infeções bacterianas em doentes cirróticos. Material e Métodos: Doentes consecutivos com cirrose hospitalizados entre 2007 e 2012 no Hamad General Hospital-Qatar foram selecionados e classificados como utilizadores ou não utilizadores de IBPs de acordo com o seu consumo nos 90 dias prévios ao internamento. A cirrose foi clinicamente diagnosticada por uma combinação de achados no exame físico, no estudo bioquímico, radiológico e endoscópico; ou por biopsia hepática. Resultados: Um total de 333 doentes foi incluído neste estudo, 171 (51.4%) medicados com IBPs e 162 não (48.6%). Os utilizadores de IBPs eram significativamente mais velhos (p = 0.001). Não se observaram diferenças estatísticas entre os dois grupos no que se refere ao sexo ou etiologia da cirrose (p > 0.05 para os dois parâmetros). A incidência global de infeções bacterianas foi significativamente superior nos utilizadores de IBPs (38%) do que nos não utilizadores (13.6%), p = 0.0001. O significado estatístico desta diferença foi observado especificamente para a PBE e para as infeções pulmonares (p = 0.0006 e p = 0.01, respetivamente). Na análise multivariada, a idade superior a 60 anos (OR = 1.246, 95% CI 1.021–08.486; p = 0.02), e a utilização de IBPs (OR = 2.149, 95% CI 1.124–06.188; p = 0.01) foram fatores preditivos independentes para PBE e para infeção bacteriana no global. Conclusão: Este estudo mostra que a utilização de IBPs, assim como a idade superior a 60 anos, são fatores preditivos independentes para o desenvolvimento de infeções bacterianas no global e para PBE nos doentes cirróticos hospitalizados. A não ser que esteja especificamente indicado a utilização de IBPs deve ser evitada neste grupo de doentes, particularmente naqueles com idade superior a 60 anos.
Palavras-Chave: Medicações ácido-supressoras, Infeção bacteriana, Infeção, Cirrose hepática, Qatar
Introduction
Since the introduction of proton pump inhibitors (PPIs) to the biopharmaceutical market in the late 1980s, this class of drugs has had a tremendous impact on patient care, clinical practice, and research development. Compared to other antacid drugs, PPIs were initially thought to have an excellent safety profile, resulting in their widespread use in both inpatient and ambulatory settings [1, 2]. After more than 25 years of clinical postmarketing experience, improved reporting, and closer scrutiny, several serious adverse effects associated with the long-term use of PPIs have emerged. These include increased risks of falls and fractures in postmenopausal women [3], a reduction of renal and liver function, and an increased risk of community-acquired and nosocomial pneumonia [4, 5]. PPIs are also found to be an independent risk factor for Clostridium difficile infection even with a very short-term use of 2 days in the intensive care setting [6].
The possible association between PPI use and increased risk of spontaneous bacterial peritonitis (SBP) and overall bacterial infection in cirrhotic patients is a debatable subject in the medical literature. While some authors point to a straight causative effect, others are not so sure. Furthermore, to our knowledge, this issue has never been investigated in the State of Qatar or in any other Arab country. The aim of this study is to evaluate the possible relationship between the use of PPIs and the development of bacterial infections in cirrhotic patients and whether PPI use increases the risk of SBP development in such patients at the main tertiary care center in Qatar.
Material and Methods
Study Population and Setting
Consecutive cirrhotic patients >18 years of age hospitalized from 2007 through 2012 to Hamad General Hospital were enrolled in this study. Hamad General Hospital is a 620-bed tertiary center that covers all specialties and is affiliated to Hamad Medical Corporation in Qatar. Data were collected retrospectively from the medical records using a data collection form including age, gender, etiology of liver cirrhosis, presence of other comorbidities, and the cause of hospital admission. Other characteristics of cirrhotic patients who were admitted to the medical wards and/or medical intensive care unit of the hospital included acute cirrhotic complications such as hepatic encephalopathy, variceal bleeding, SBP or other infections, refractory ascites, hepatorenal syndrome, and first diagnosis of hepatocellular carcinoma. Cirrhotic patients with active gastrointestinal bleeding, disseminated malignancies, undergoing immunosuppressive therapy, or using antibiotics in the previous 2 weeks prior to hospitalization were excluded from this study.
Acid-Suppressive Medication Exposure
To determine drug exposure, medical records were reviewed for PPI use in the 90 days prior to hospitalization, and each subject was classified as PPI user versus non-PPI user. Exposure to acidsuppressive medication was defined as any order for a prescription of PPI or histamine-2 receptor antagonists (H2RAs). The PPIs included were either pure or compound medication containing omeprazole, lansoprazole, esomeprazole, pantoprazole, or rabeprazole. H2RAs included any drugs containing ranitidine, cimetidine, or famotidine. A cumulative treatment period for ≥7 days was required for inclusion. Unexposed status was defined as no prescription or cumulative treatment period of
Statistical Analysis
Analysis used were χ2 for categorical variables expressed as number (percent) and the independent t test for continuous variables (e.g., age) expressed as the mean ± standard deviation. Multivariate logistic regression analysis was used to produce the prediction model for infections in cirrhotic patients.
Results
Study Population and Use of PPIs
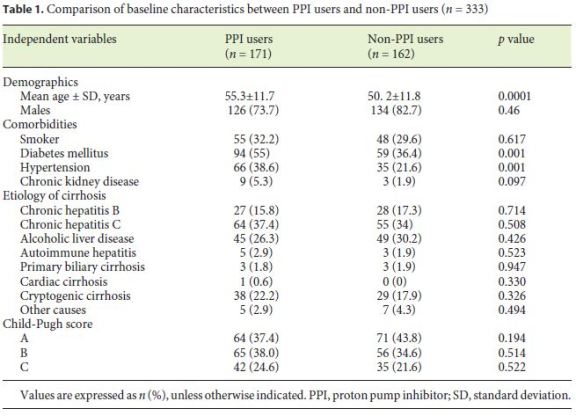
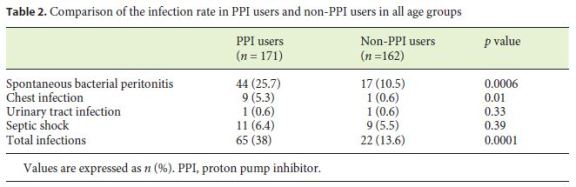
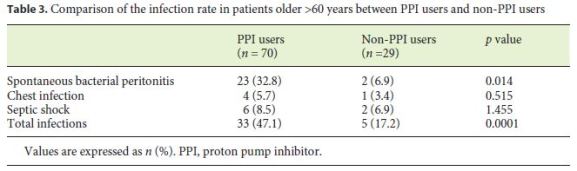
A total of 333 cirrhotic patients were included in this study, and 78.1% of them were male. Hepatitis C infection (35.7%), alcohol abuse (20.1%), and hepatitis B infection (16.5%) were the main etiologies of cirrhosis. The presence of SBP was detected in 61 (18.3%) patients, and the severity of liver disease according to the Child-Pugh score was significantly associated with the risk of SBP development (HR = 1.9, 95% CI: 1.21–3.80, p = 0.01 in ChildPugh B patients and HR = 4.10, 95% CI: 1.87–7.86, p = 0.001 in Child-Pugh C patients). There were 171 (51.4%) patients using PPIs and 162 (48.6%) not using PPIs. Only 4 patients in the PPI-user group had a history of a prior consumption of H2RAs. Specific indication for PPI use was not documented in 143 (43%) of our patients. Table 1 shows the comparison of demographic and clinical data between the 2 groups. PPI users were significantly older in age (p = 0.0001), and there was no statistical difference between the 2 groups in gender distribution, etiology of cirrhosis, and Child-Pugh score (p > 0.05 for all parameters). As shown in Table 2, PPI users had a significantly higher incidence of overall bacterial infection rate (38%) than non-PPI users (13.6%; p = 0.0001). Statistical significance is observed specifically for SBP and chest infection (p = 0.0006 and p = 0.01, respectively). In a subgroup analysis for patients older than 60 years of age, PPI users had a significantly higher overall bacterial infection rate (47.1%) than non-PPI users (10.3%; p = 0.0001). For SBP, the rate in PPI users was also higher (32.8%) than in non-PPI users (6.9%; p = 0.0014) (Table 3).
Multivariate Analysis
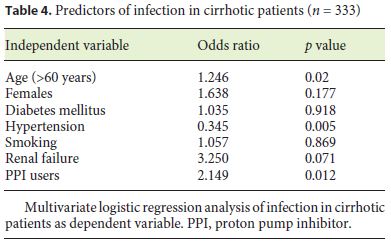
On the multivariate analysis, age >60 years (OR = 1.246, 95% CI 1.021–08.486; p = 0.02) and PPI use (OR = 2.149, 95% CI 1.124–6.188; p = 0.012) were independent predicting factors for SBP and overall bacterial infection (Table 4).
Discussion
The present study has shown that the use of PPIs in patients with liver cirrhosis is an independent risk factor for overall infection and SBP development, hence support an association between PPI use and SBP. PPIs have been widely used worldwide since their introduction around 3 decades ago. A growing list of their adverse effects is being compiled. In an early study, acid-activated omeprazole was documented to inhibit in vitro human neutrophil phagocytosis and phagolysosome acidification [10]. Another small study (blood samples from 10 healthy subjects) documented the impairment of reactive oxygen intermediates by human neutrophils after omeprazole administration. This finding possibly alludes to the bactericidal activity of reduced neutrophils [11].
Patients with liver cirrhosis usually suffer from a poor synthetic function with a decreasing albumin production. There is a growing body of evidence that they suffer from a complex and not fully understood cirrhosis-associated immune dysfunction syndrome [12]. The evolving explanation for this impaired immunity includes: a decrease in T-helper cells and phagocytic potential of both monocytes and neutrophils [13], an increased level of cyclooxygenase-derived eicosanoid prostaglandin E2 [14], and a decreased HLA-DR expression on monocytic cells defined as immune paralysis [15].
The use of PPIs in patients with cirrhosis may further degrade their already compromised immune system. Garcia-Martinez and coworkers have recently demonstrated that PPIs significantly decrease granulocyte and monocyte cellular oxidative burst in patients afflicted with cirrhosis; a pathogenic finding that possibly explains the reported high rates of bacterial infections in these patients [16]. The most common infection is SBP [17]. The mechanism of development of SBP in cirrhotic patients is not fully explicated; however, increased intestinal permeability, altered intestinal motility, and increased small intestinal bacterial overgrowth may play an important role in facilitating bacterial translocation [18, 19]. PPIs have been identified as an important factor for increased small intestinal bacterial overgrowth [20].
In the clinical setting, the role of PPIs in the pathogenesis of SBP in cirrhotic patients has been hotly debated for the last decade. When it comes to PPI use and SBP association, we can clearly identify 2 opposite groups. The first one is made of authors who concluded that there is no causative effect. An example is the 2008 case-control study by Campbell et al. [21] that included 116 consecutive cirrhotic patients. A second retrospective study by Mandorfer et al. [22] that enrolled a larger number of subjects (607 consecutive patients) reported no association between PPI use and SBP or other infections or mortality. Another large prospective study involved 770 decompensated cirrhotic consecutive patients in 23 hospitals in Argentina and failed to demonstrate an association between PPI therapy and an increased risk of SBP [23]. In a more recent retrospective cohort study that enrolled 307 cirrhotic patients with a previous SBP in Korea, the incidence of second SBP did not statistically differ between PPI users and non-PPI users who were followed up for 5 years [24]. Furthermore, a more recent cohort study conducted in southern Brazil that enrolled 258 cirrhotic patients with ascites did not confirm the high risk of SBP development in PPI users compared to PPI-non users [25].
The second group of authors claims the opposite view. They advocate a direct correlation between PPI use and the increased risk of developing SBP. Their number has been increasing recently, and their evidence is growing stronger. We identified many studies in this respect, including 3 meta-analyses. The first one, conducted in 2011, included 4 studies involving 772 patients. It found a significant association between PPI use and the development of SBP (OR 2.77, 95% CI 1.82–4.23) [26]. In 2013, a second meta-analysis that reviewed 8 studies was conducted. It examined the association between acidsuppressive therapy (PPI and H2RAs) in cirrhotic patients and the risk of developing SBP. This risk was greater in subjects on PPI treatment (n = 3,815; OR 3.15, 95% CI 2.09–4.74) compared to those taking H2RAs (n = 562; OR 1.71, 95% CI 0.97–3.01). Authors concluded that patients with cirrhosis receiving PPIs have approximately 3 times the risk of developing SBP compared with those not taking these medications [27]. More recently, in 2015, a third meta-analysis reviewed 17 studies published between 2008 and 2014 (12 journal articles and 5 conference abstracts) involving 8,204 patients. These studies were conducted with North American (8 studies), European (4 studies), South East Asian (4 studies), and South American (1 study) populations; none of them examined the Arabic population. The result showed that PPI use in cirrhotic patients was significantly associated with an increased risk of SBP (OR 2.17, 95% CI 1.46– 3.23) and an overall risk of bacterial infection (OR 1.98, 95% CI 1.36–2.87) [28]. Many other investigations in the medical literature confirm this association. A large Korean study (1,140 patients) by Kwon et al. [29] confirmed that PPI use (within 30 days) in cirrhotic patients having ascites increased their risk of developing SBP, especially in the elderly and in patients with a high model for endstage liver disease score on admission. Further, the mortality risk was also found to be higher in this group of patients. Another recent Taiwanese case-control study published in 2015 identified a total of 947 patients among 86,418 patients with advanced liver cirrhosis using acid suppression. It further confirmed the risk of developing SBP with higher cumulative days of gastric acid suppression being associated with a higher risk of infection (p < 0.0001) [19]. In a more recent study, the use of PPIs has been found to be a risk factor for developing hepatic encephalopathy and SBP in cirrhotic patients with ascites [30].
The present study included 333 cirrhotic patients between 2007 and 2012. It further solidified the argument that PPI use and older age (>60 years) are independent risk factors for the development of SBP in these patients. We side with all prior authors that further trials (especially prospective comparative ones) will probably shed more light on all potential adverse effects of PPIs in patients with liver cirrhosis. We also recommend that adequate precautions are taken to utilize such treatment in cirrhotic patients only when benefit may outweigh potential harm.
In conclusion, the evidence that PPIs pose health risks in certain patient populations is expanding. Cirrhotic patients receiving this form of therapy seem to have a higher risk of developing SBP. The present study shows that PPI use, as well as older age (>60 years), was an independent predicting factor for the development of bacterial infection including SBP in hospitalized cirrhotic patients. Further studies are needed to settle the current debate between supporters and opponents of these conclusions. We recommend that unless it is clearly indicated, PPI therapy should be avoided in patients using PPIs, in particular those who are older than 60 years of age.
References
1 Durand C, Willett KC, Desilets AR: Proton pump inhibitor use in hospitalized patients: is overutilization becoming a problem? Clin Med Insights Gastroenterol 2012;5:65–76. [ Links ]
2 Rotman SR, Bishop TF: Proton pump inhibitor use in the U.S. ambulatory setting, 2002– 2009. PLoS One 2013;8:e56060. [ Links ]
3 Lewis JR, Barre D, Zhu K, Ivey KL, Lim EM, Hughes J, Prince RL: Long-term proton pump inhibitor therapy and falls and fractures in elderly women: a prospective cohort study. J Bone Miner Res 2014;29:2489–2497. [ Links ]
4 Thomson AB, Sauve MD, Kassam N, Kamitakahara H: Safety of the long-term use of proton pump inhibitors. World J Gastroenterol 2010;16:2323–2330. [ Links ]
5 Miano TA, Reichert MG, Houle TT, MacGregor DA, Kincaid EH, Bowton DL: Nosocomial pneumonia risk and stress ulcer prophylaxis: a comparison of pantoprazole versus ranitidine in cardiothoracic surgery patients. Chest 2009;136:440–447. [ Links ]
6 Barletta JF, Sclar DA: Proton pump inhibitors increase the risk for hospital-acquired Clostridium difficile infection in critically ill patients. Crit Care 2014;18:714. [ Links ]
7 O’leary JG, Reddy KR, Wong F, Kamath PS, Patton HM, Biggins SW: Long-term use of antibiotics and proton-pump imhibitors predict development of infections in patients with cirrhosis. Clin Gastroenterol Hepatol 2015;13:753–759.
8 Bajaj SC, O’leary JG, Reddy KR, Wong F, Olson JC, Subramanian RM, Brown G, et al: Second infections independently increase mortality in hospitalized patients with cirrhosis. North American consortium for the study of end-stage of liver disease (NACSELD) experience. Hepatology 2012:56:2328–2335.
9 Churpek MM, Snyder A, Sokol S, Pettit NN, Edelson DP: Investigating the impact of different suspicion of infection criteria on the accuracy of quick sepsis-related organ failure assessment, systemic inflammatory response syndrome, and early warning scores. Crit Care Med 2017;45:1805–1812. [ Links ]
10 Agastya G, West BC, Callahan JM: Omeprazole inhibits phagocytosis and acidification of phagolysosomes of normal human neutrophils in vitro. Immunopharmacol Immunotoxicol 2000;22:357–372. [ Links ]
11 Zedtwitz-Liebenstein K, Wenisch C, Patruta S, Parschalk B, Daxböck F, Graninger W: Omeprazole treatment diminishes intra- and extracellular neutrophil reactive oxygen production and bactericidal activity. Crit Care Med 2002;30:1118–1122. [ Links ]
12 Sipeki N, Antal-Szalmas P, Lakatos PL, Papp M: Immune dysfunction in cirrhosis. World J Gastroenterol 2014;20:2564–2577. [ Links ]
13 Lagadinou M, Solomou EE, Velissaris D, Theodorou GL, Karakatza M, Gogos CA: Alterations in T-lymphocyte subpopulations in patients with complicated liver cirrhosis. Diagn Microbiol Infect Dis 2013;75:348–356. [ Links ]
14 O’Brien AJ, Fullerton JN, Massey KA, Auld G, Sewell G, James S, Newson J, et al: Immunosuppression in acutely decompensated cirrhosis is mediated by prostaglandin E2. Nat Med 2014;20:518–523.
15 Lin CY, Tsai IF, Ho YP, Huang CT, Lin YC, Lin CJ, Tseng SC, et al: Endotoxemia contributes to the immune paralysis in patients with cirrhosis. J Hepatol 2007;46:816–826. [ Links ]
16 Garcia-Martinez I, Francés R, Zapater P, Giménez P, Gómez-Hurtado I, Moratalla A, Lozano-Ruiz B, et al: Use of proton pump inhibitors decrease cellular oxidative burst in patients with decompensated cirrhosis. J Gastroenterol Hepatol 2015;30:147–154. [ Links ]
17 Min WY, Lim KS, Min BH, Gwak GY, Paik YH, Choi MS, Lee JH, et al: Proton pump inhibitor use significantly increases the risk of spontaneous bacteria peritonitis in 1965 patients with cirrhosis and ascites: a propensity score matched cohort study. Aliment Pharmacol Ther 2014;40:695–704. [ Links ]
18 von Vlerken LG, Huisman EJ, van Hoek B, Renooij W, Felix W, Siersema PD, van Erpecum KJ: Bacterial infections in cirrhosis: role of proton pump inhibitors and intestinal permeability. Eur J Clin Invest 2012;42:760–767. [ Links ]
19 Chang SS, Lai CC, Lee MT, Lee YC, Tsai YW, Hsu WT, Lee CC: Risk of spontaneous bacterial peritonitis associated with gastric acid suppression. Medicine (Baltimore) 2015;94:e944. [ Links ]
20 Parkman HP, Urbain JL, Knight LC, Brown KL, Trate DM, Miller MA, Maurer AH, et al: Effect of gastric acid suppressant on human gastric motility. Gut 1998;42:2043–2050. [ Links ]
21 Campbell MS, Obstein K, Reddy KR, Yang YX: Association between proton pump inhibitor use and spontaneous bacterial peritonitis. Dig Dis Sci 2008;53:394–398. [ Links ]
22 Mandorfer M, Bota S, Schwabl P, Bucsics T, Pfisterer N, Summereder C, Hagmann M, et al: Proton pump inhibitor intake neither predisposes to spontaneous bacterial peritonitis or other infections nor increases mortality in patients with cirrhosis and ascites. PLoS One 2014;9:e110503. [ Links ]
23 Terg R, Casciato P, Garbe C, Cartier M, Stieben T, Mendizabal M, Niveyro C, et al: Proton pump inhibitor therapy does not increase the incidence of spontaneous bacterial peritonitis in cirrhosis: a multicenter prospective study. J Hepatol 2015;62:1056–1060. [ Links ]
24 Kim JH, Lim KS, Min YW, Lee H, Min BH, Rhee PL, Kim JJ, et al: Proton pump inhibitors do not increase the risk for recurrent spontaneous bacterial peritonitis in patients with cirrhosis. J Gastroenterol Hepatol 2017;32:1064–1070. [ Links ]
25 Miozzo SAS, John JA, Appel-da-Silva MC, Dossin IA, Tovo CV, Mattos AA. Influence of proton pump inhibitors in the development of spontaneous bacterial peritonitis. World J Hepatol 2017;9:1278–1285. [ Links ]
26 Trikudanathan G, Israel J, Cappa J, O’Sullivan DM: Association between proton pump inhibitors and spontaneous bacterial peritonitis in cirrhotic patients – a systematic review and meta-analysis. Int J Clin Pract 2011;65:674–678.
27 Deshpande A, Pasupuleti V, Thota P, Pant C, Mapara S, Hassan S, Rolston DD, et al: Acidsuppressive therapy is associated with spontaneous bacterial peritonitis in cirrhotic patients: a meta-analysis. J Gastroenterol Hepatol 2013;28:235–242. [ Links ]
28 Xu HB, Wang HD, Li CH, Ye S, Dong MS, Xia QJ, Zhang AQ, et al: Proton pump inhibitor use and risk of spontaneous bacteria peritonitisin cirrhotic patiens: a systematic review and meta analysis. Genet Molecular Research 2015;14:7490–7501. [ Links ]
29 Kwon JH, Koh SJ, Kim W, Jung YJ, Kim JW, Kim BG, Lee KL, et al: Mortality associated with proton pump inhibitors in cirrhotic patients with spontaneous bacterial peritonitis. J Gastroenterol Hepatol 2014;29:775–781. [ Links ]
30 Dam G, Vilstrup H, Watson H, Jepsen P: Proton pump inhibitors as a risk factor for hepatic encephalopathy and spontaneous bacterial peritonitis in patients with cirrhosis with ascites. Hepatology 2016;64:1265–1272. [ Links ]
Statement of Ethics
The ethical approval for this study was obtained from the Institutional Research Review Board at Hamad Medical Corporation, Qatar (research approval No. 13246/2013).
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Prof. Abdel-Naser Elzouki
Department of Medicine, Hamad General Hospital
Hamad Medical Corporation, P.O. Box 3050
Doha 3050 (Qatar)
E-Mail nelzouki_1999@yahoo.com
Received: November 28, 2017; Accepted after revision: February 23, 2018

