










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.6 Lisboa dez. 2018
https://doi.org/10.1159/000487156
REVIEW ARTICLE
Ultrasonography in Gastroenterology: The Need for Training
Ecografia na Gastrenterologia: necessidade de formação
João Pinto, Richard Azevedo, Eduardo Pereira, Ana Caldeira
Gastroenterology Department, Amato Lusitano Hospital, Castelo Branco, Portugal
* Corresponding author.
ABSTRACT
The use of ultrasonography (US) as an imaging modality in medicine has spread across almost every clinical specialty. This diffusion is based on the simplicity, accessibility, portability and affordability of the technique producing real-time high-resolution images using non-ionising radiation. On the other hand, this trend also extended the technique to settings other than healthcare, such as public facilities, private houses or remote sites. This tendency can be observed worldwide, from developing countries to prestigious medical schools and tertiary referral hospitals. Furthermore, point-of-care US (POCUS), i.e., US executed at the patients bedside to obtain real-time objective information with diagnostic and clinical monitoring purposes or to guide invasive procedures, has been incorporated in many specialties. In gastroenterology, despite the essential role of endoscopy, clinical practice is highly dependent on non-endoscopic imaging techniques. However, as in other specialties, the indications of US in gastroenterology have been increasing steadily, covering a broad range of conditions. In response to the generalised employment of US by non-radiologists, institutions such as the European Federation of Societies for Ultrasound in Medicine and Biology and the Royal College of Radiologists issued recommendations to ensure high-quality practice. These theoretical and practical requisites include performing a certain number of examinations and mandatory skills in order to achieve certification to execute unsupervised US. Therefore, there is a need for modern gastroenterology to include US as a basic skill in its clinical practice. To ensure the provision of high-quality US, adequate instruction of future specialists should be guaranteed by the gastroenterology departments and required in the residency training programme.
Keywords: Ultrasonography, Point-of-care ultrasonography, Gastroenterology, Training, Physical examination
RESUMO
A utilização em Medicina da ultrassonografia como modalidade imagiológica expandiu-se a quase todas as especialidades clínicas. Esta difusão baseou-se na simplicidade, acessibilidade, portabilidade e baixo custo para obtenção em tempo real de imagens de alta resolução utilizando radiação não-ionizante. Por outro lado, esta corrente disseminou a técnica para além das instituições de saúde, em instalações públicas, residências privadas, ou locais remotos. Esta tendência ocorre globalmente, de países subdesenvolvidos a hospitais terciários e faculdades de medicina prestigiadas. Além disso, a ecografia point-of-care (EPOC), i.e., ultrassonografia realizada à cabeceira do doente para obtenção de informação em tempo real com fins diagnósticos, de monitorização clínica ou orientação de procedimentos invasivos, tem sido assumida por muitas especialidades. Na Gastrenterologia, apesar do papel essencial da endoscopia, a prática clínica encontra-se altamente dependente de exames de imagem não-endoscópica. Contudo, como noutras especialidades, as indicações para ultrassonografia em Gastrenterologia têm crescido continuamente, cobrindo um vasto leque de patologias. No seguimento da utilização generalizada da ecografia por não-radiologistas, instituições como a European Federation of Societies for Ultrasound in Medicine and Biology e o Royal College of Radiologists publicaram recomendações para assegurar um desempenho de alta qualidade. Estes requisitos teóricos e práticos incluem números mínimos de exames e competências técnicas a alcançar para a certificação com o fim de realizar autonomamente ultrassonografia digestiva. Existe, portanto, a necessidade de a Gastrenterologia moderna incluir a ecografia como um procedimento básico na prática clínica. Para assegurar a execução de ultrassonografia de alta qualidade, a formação adequada dos futuros especialistas deve ser garantida pelos Serviços de Gastrenterologia e exigida nos Programas de Formação do Internato.
Palavras-Chave: Ultrassonografia, Ecografia point-of-care, Gastroenterologia, Formação, Exame físico
Introduction
Since the first report of the application of ultrasonography (US) as a medical imaging modality by Dr. Tussik in 1942 [1], this technique has spread across almost every clinical specialty. This global acceptability can be explained by the unique properties of US as an imaging modality. Being a simple and accessible technique, it produces high-resolution images, providing a true real-time anatomic and functional observation. Furthermore, the readiness of the technique, combined with affordability and the safety of using non-ionising radiation, permits its repetitive utilisation in many clinical scenarios [2–4].
The dissemination of US started in medical specialties, such as neurology [1], cardiology [5, 6] or obstetrics/gynaecology [7], whose physicians discovered the convenience of using US on demand to guide their clinical decisions several decades ago. Hence, these medical areas eventually reached a state of specialised clinical US.
In the past couple of decades, the development of smaller, portable and less expensive devices has generalised the access to US from primary to intensive care, from home-based palliative medicine to operating rooms and emergency departments. Moreover, this trend can be observed worldwide, from rural areas in developing countries to top-quality medical schools and tertiary referral hospitals [8–17].
Point-of-Care US
In this context, diverging from the classical comprehensive US evaluation, the concept of point-of-care US (POCUS) was created to define a new way of using US in medicine [2, 3, 15]. In this modality, clinicians perform US at the patients bedside to obtain immediate answers to concrete questions concerning the diagnosis, evolution of the disease or response to therapy. On the other hand, the realtime localisation of structures with POCUS is also used to guide diagnostic and therapeutic interventions. Examples include the protocol of Extended-Focused Assessment with Sonography for Trauma (E-FAST) [18–21] or using US to guide the placement of a central venous catheter [22–27]. The clinical settings where POCUS can be applied are almost unlimited and include healthcare venues (clinics, wards, emergency departments or intensive care units), private houses, public facilities or remote places, such as airplanes, oil platforms or space stations [4, 23, 28–34].
Given all these developments, and following the paradigm of specialties such as cardiology or obstetrics/gynaecology, other areas of medical care have included US in their clinical practice according to their requirements [10, 26–28, 30, 35–37]. We can define 3 broad subtypes of US performed by non-radiologists [38]:
− diagnostic/descriptive(routine echocardiography or morphological examination of the foetus);
− clinical observation (E-FAST, evaluation of the intravascular volume status to adjust resuscitation procedures);and
− interventional(to guide a central catheter insertion or peripheral nerve blockade).
The Role for US in Gastroenterology
In gastroenterology, the endoscopic visualisation of the mucosa of the digestive tract has always been one of the key components in the training and practice of clinicians. Concurrently, up-to-date care in this specialty is obligatorily supported by multiple imaging modalities. Nevertheless, the previously stated trend for the use of US by non-radiologists has found great adherence in gastroenterology, and US is increasingly seen as a basic skill among gastroenterologists [2, 39–43].
For us, essentially clinicians, the possibility of using this affordable and non-invasive technique for the realtime evaluation of structures ranging from solid organs to hollow viscera or surrounding structures is of great interest. For instance, in some cases, the origin of abdominal symptoms lies in thoracic, abdominal or pelvic nondigestive organs. Furthermore, US allows a real-time dynamic and interactive observation of the motility of the digestive tract. This evaluation has almost no effect on the function of the organ, in contrast with endoscopic examinations or motility tests that require the insertion of luminal probes.
Already common practice in many countries [41, 42, 44], this change of paradigm is ultimately related to the concept of digestive US. This patient-centred approach is carried out by the gastroenterologist who, while performing US, integrates the visual information obtained under a clinical perspective with the known medical history, symptoms and signs of that concrete patient. The doctor following the patient is the most suitable intervenient to use this abdominal palpation guided by US as an extension of the physical examination and clinical history.
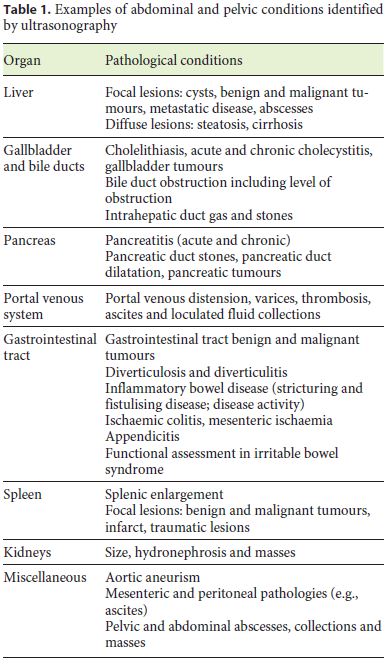
Using this methodology, as in other specialties, the fields of application encompass the above-mentioned 3 aspects of diagnosis, clinical monitoring or interventional guidance. These include, for example, screening for hepatocellular carcinoma in cirrhotic patients (diagnostic/descriptive) [45–48], monitoring of inflammatory bowel disease (IBD) activity (clinical monitoring) [49–55] or percutaneous therapy of hepatocellular carcinoma (interventional guidance) [56–58]. Regarding some of the abdominal and pelvic conditions that can be identified by digestive US, an abridged list is presented in Table 1 [2, 40, 43, 59, 60].
Furthermore, the development of new ancillary ultrasonographic techniques has broadened the indications for US, shifting from a mostly morphological description to a more physiological evaluation. In recent years, these advances in areas such as contrast-enhanced US (CEUS) or elastography have been particularly relevant to areas such as hepatology and IBD.
For instance, the use of micro-bubble ultrasound contrast agents has allowed, among other indications, the characterisation of focal liver lesions in cirrhotic and non-cirrhotic patients according to the patterns of vascularisation, the study of portal vein thrombosis or the monitoring of the effects of ablative therapies for hepatocellular carcinoma [44, 61–63]. On the other hand, nonhepatic indications for CEUS include the management of IBD (estimation of disease activity, distinction between fibrous and inflammatory strictures, characterisation of suspected abscesses or to confirm and follow the route of fistulas) or pancreatic diseases (to characterise pancreatic focal lesions or to depict necrotic areas in the context of acute pancreatitis) [43, 50, 51, 53, 54, 63–65].
Likewise, the use of elastography or the representation of the elasticity of tissues according to the observed deformation that occurs in response to an applied force has several validated indications in clinical US [66–68]. Concerning hepatology, the evaluation of the degree of hepatic fibrosis by a non-invasive method, such as ultrasound elastography, is probably the most disseminated utilisation [67, 69–71]. Conversely, in IBD, elastography has been used to distinguish between fibrotic and inflammatory strictures [49, 52–54, 64, 66, 67, 70, 72–74].
The Importance of Training in US
Given the increasing interest of so many clinicians from several medical specialties in using US examination in daily practice, there is a concern to ensure high-quality US services in every setting. Consequently, several national and European training boards have issued recommendations regarding training and certification of nonradiologists executing US-based procedures [38, 59, 75]. These documents include standards for theoretical knowledge and practical skills, including performing a certain number of examinations and mandatory skills in order to execute unsupervised US.
The learning process in US starts with the theoretical knowledge of anatomical structures, pathological entities and the technique, followed by an evolving ability to perform the examination itself from supervised to independent practice [40]. The recommendations concerning US practice usually comprehend progressive degrees of expertise, ranging from level 1 practitioners, who are able to perform unsupervised common US explorations, to level 3 practitioners, reserved to experts dedicated to teaching and research in US.
Training Curriculum for Gastroenterology and Hepatology
The Blue Book or Speciality Training Programme and Curriculum for Gastroenterology and Hepatology was created by the European Section and Board of Gastroenterology and Hepatology (ESBGH) with the objective of defining a standard of training for European gastroenterology residents [75]. The document defines a common core curriculum with theoretical and practical requirements to practice autonomously as a gastroenterologist and hepatologist.
The ESBGH, while recognising that, concerning US, there are different realities throughout Europe, defines it as a basic competence of gastroenterologists, who should undergo training in order to use it with a diagnostic purpose and to guide interventional procedures, such as paracentesis or liver biopsy. For this reason, the document states that training centres should ensure that there is equipment for performing US and US-guided hepatic biopsy. The Blue Book also includes an advanced training module in US related to endoscopic ultrasound [75].
Objectives of Training in US in Gastroenterology
The Royal College of Radiologists (RCR) Ultrasound Training Recommendations for Medical and Surgical Specialties [38] and the European Federation of Societies for Ultrasound in Medicine and Biologys (EFSUMB) Minimum Training Recommendations for the Practice of Medical Ultrasound [59] both recommend specific training milestones and objectives for gastroenterologists performing US. Before enrolling into practical training, trainees should undergo introductory theoretical instruction on anatomy, physics and artefacts, equipment characteristics and imaging modalities, examination techniques and methods. Usually, this preparation is accomplished through formal courses [59].
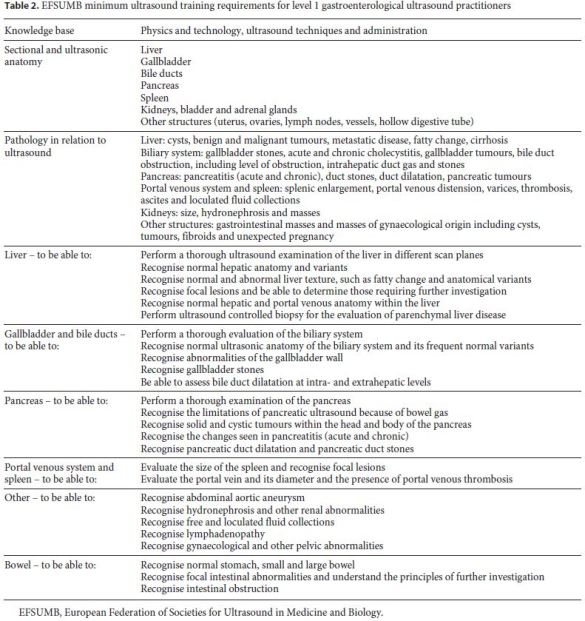
According to the EFSUMB document [59], gastroenterologists should execute 5–10 examinations per week, reaching a minimum of 300 examinations before performing US unsupervised in practice, although different learning rates will be accomplished by each trainee. The training activity frequency could be intermittent, although interruptions longer than 3 months should be avoided and a yearly minimum of 100 procedures is suggested. These examinations should be supervised by a level 2 practitioner (or a level 1 practitioner with at least 2 years of experience). At this level, to become competent to perform unsupervised digestive US examinations, they should be capable of observing the normal abdominal anatomy, of recognising anatomical variants and most of the pathological conditions and of acknowledging the need for a second opinion or further investigation. The specific necessary aptitudes defined by the EFSUMB are specified in Table 2 [59].
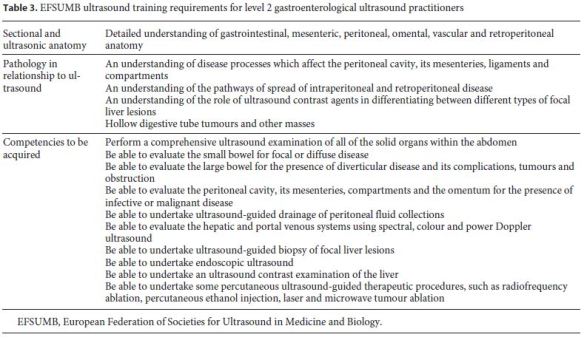
To perform US as a level 2 practitioner, gastroenterologists should have at least 1 year of experience as level 1 clinicians and complete a set of a further 500 examinations. This practice should be supervised by a level 3 practitioner (or a level 2 practitioner with at least 2 years of experience). Besides mastering the pathological conditions required for level 1, at this level, they should accept and manage referrals from level 1 practitioners and perform teaching activities (undergraduate level and supervision of level 1 practice). Therefore, level 2 clinicians should recognise and correctly diagnose almost all conditions and should thus identify also changes and conditions of structures that are more challenging to evaluate by US. Additionally, level 2 practitioners should become competent in more advanced ultrasonographic techniques and interventional procedures. Table 3 presents the skills that should be accomplished at this level according to the RCR and EFSUMB recommendations [38, 59].
In level 3, experts controlling all the requisites for level 1 and 2 should be mostly or fully dedicated to advanced US, training, research and development of new areas.
Competency Assessment
In spite of the goal to provide high-quality services, digestive US practitioners still lack clear quality indicators or performance measures, in contrast to other areas, such as gastrointestinal endoscopy [76, 77]. The requisites for the 3 levels of expertise defined by the RCR and EFSUMB are fairly broad boundaries that state what is expected of these clinicians [38, 59]. Still, they should not aim merely to fulfil the required minimum levels but rather to enrol into a lifelong learning process according to the individual context (areas of dedication, prevalence of disorders, etc.) [40].
Maintenance of Skills
Despite achieving competency in digestive US, clinicians should have regular ultrasonographic activity to maintain practical skills. According to the RCR Ultrasound Training Recommendations for Medical and Surgical Specialties, level 1 practitioners should perform at least 250 scans annually [38]. At all levels of expertise, clinicians should audit their practice, attend regular multidisciplinary meetings, keep up with the latest published evidence and participate in courses and congresses [59].
The Portuguese Reality in US Training
As in other European countries [41, 42, 44], in Portugal there is a positive trend towards digestive US performed by gastroenterologists. Nevertheless, it seems that there is still some distance to go. Currently, few gastroenterology departments ensure regular high-quality US services, much less regular training in US. The Portuguese curriculum requires, besides the training in the radiology departments, only a minimum of 50 clinical US examinations, and the specific period of training in clinical US is optional.
The Portuguese Group of Ultrasound in Gastroenterology (GRUPUGE) has played a determinant role in the divulgation of US among gastroenterologists. The initiatives include, among others, the implementation of hands-on courses, such as the annual 2-day course of introduction to US, the pre-congress course at the National Congress Semana Digestiva and other more specific courses on IBD or liver elastography. On the other hand, there are incentives such as prizes for the works on US or the creation of grants to promote investigation in this area.
Conclusion
There is a considerable amount of evidence to support the use of US by gastroenterologists [2, 4, 21, 44, 60], and an increasing number of statements and guidelines support this practice [2, 38, 43, 56–59, 62, 63, 66–69, 71, 75]. In spite of the recommendations in the Blue Book of the ESBGH regarding training in US, there is a heterogeneous distribution of the utilisation of this basic skill by European gastroenterologists.
The Portuguese reality has been marked by a very positive trend towards a more frequent routine utilisation of US, based on adequate training and research in this technique. Nonetheless, maybe it is time to adjust the requirements of the Portuguese curriculum of gastroenterology to guarantee this need for training in US. However, for that, far more departments competent in digestive US education are needed.
References
1 Shampo MA, Kyle RA: Karl Theodore Dussik – pioneer in ultrasound. Mayo Clin Proc 1995;70:1136. [ Links ]
2 Dietrich CF, Goudie A, Chiorean L, Cui XW, Gilja OH, Dong Y, Abramowicz JS, Vinayak S, Westerway SC, Nolsoe CP, Chou YH, Blaivas M: Point of care ultrasound: a WFUMB position paper. Ultrasound Med Biol 2017;43:49–58. [ Links ]
3 Moore CL, Copel JA: Point-of-care ultrasonography. N Engl J Med 2011;364:749–757. [ Links ]
4 Greiner L: Ultrasonography in abdominal emergencies: quick and easy and safe decision making. Crit Ultrasound J 2009;1:23–24. [ Links ]
5 Coman IM, Popescu BA: Shigeo Satomura: 60 years of Doppler ultrasound in medicine. Cardiovasc Ultrasound 2015;13:48. [ Links ]
6 Wells PN, Liang HD: Medical ultrasound: imaging of soft tissue strain and elasticity. JR Soc Interface 2011;8:1521–1549. [ Links ]
7 Donald I: Clinical application of ultrasonic techniques in obstetrical and gynaecological diagnosis. J Obstet Gynaecol Br Emp 1962;69:1036. [ Links ]
8 Serrao G, Tassoni M, Magenta-Biasina AM, Mantero AG, Previtera A, Turci MC, Biganzoli EM, Bertolini EAM: Virtual dissection by ultrasound: probe handling in the first year of medical education. Ultrasound Int Open 2017;3:E156–E162. [ Links ]
9 Blackstock U, Munson J, Szyld D: Bedside ultrasound curriculum for medical students: report of a blended learning curriculum implementation and validation. J Clin Ultrasound 2015;43:139–144. [ Links ]
10 So S, Patel RM, Orebaugh SL: Ultrasound imaging in medical student education: impact on learning anatomy and physical diagnosis. Anat Sci Educ 2017;10:176–189. [ Links ]
11 Heinzow HS, Friederichs H, Lenz P, Schmedt A, Becker JC, Hengst K, Marschall B, Domagk D: Teaching ultrasound in a curricular course according to certified EFSUMB standards during undergraduate medical education: a prospective study. BMC Med Educ 2013;13:84. [ Links ]
12 Galusko V, Khanji MY, Bodger O, Weston C, Chambers J, Ionescu A: Hand-held ultrasound scanners in medical education: a systematic review. J Cardiovasc Ultrasound 2017;25:75–83. [ Links ]
13 Rempell JS, Saldana F, DiSalvo D, Kumar N, Stone MB, Chan W, Luz J, Noble VE, Liteplo A, Kimberly H, Kohler MJ: Pilot point-of-care ultrasound curriculum at Harvard Medical School: early experience. West J Emerg Med 2016;17:734–740. [ Links ]
14 Patel SG, Benninger B, Mirjalili SA: Integrating ultrasound into modern medical curricula. Clin Anat 2017;30:452–460. [ Links ]
15 Solomon SD, Saldana F: Point-of-care ultrasound in medical education – stop listening and look. N Engl J Med 2014;370:1083–1085. [ Links ]
16 Baltarowich OH, Di Salvo DN, Scoutt LM, Brown DL, Cox CW, DiPietro MA, Glazer DI, Hamper UM, Manning MA, Nazarian LN, Neutze JA, Romero M, Stephenson JW, Dubinsky TJ: National ultrasound curriculum for medical students. Ultrasound Q 2014;30:13–19. [ Links ]
17 Dinh VA, Frederick J, Bartos R, Shankel TM, Werner L: Effects of ultrasound implementation on physical examination learning and teaching during the first year of medical education. J Ultrasound Med 2015;34:43–50. [ Links ]
18 Lingawi SS, Buckley AR: Focused abdominal US in patients with trauma. Radiology 2000; 217:426–429. [ Links ]
19 McGahan JP, Wang L, Richards JR: From the RSNA refresher courses: focused abdominal US for trauma. Radiographics 2001;21(Spec No):S191–S199. [ Links ]
20 Dolich MO, McKenney MG, Varela JE, Compton RP, McKenney KL, Cohn SM: 2,576 ultrasounds for blunt abdominal trauma. J Trauma 2001;50:108–112. [ Links ]
21 McGahan JP, Rose J, Coates TL, Wisner DH, Newberry P: Use of ultrasonography in the patient with acute abdominal trauma. J Ultrasound Med 1997;16:653–662;quiz 663–654. [ Links ]
22 Troianos CA, Hartman GS, Glas KE, Skubas NJ, Eberhardt RT, Walker JD, Reeves ST; Councils on Intraoperative Echocardiography and Vascular Ultrasound of the American Society of Echocardiography; Society of Cardiovascular Anesthesiologists: Special articles: guidelines for performing ultrasound guided vascular cannulation: recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. Anesth Analg 2012;114:46–72. [ Links ]
23 Levy JA, Noble VE: Bedside ultrasound in pediatric emergency medicine. Pediatrics 2008;121:e1404–e1412. [ Links ]
24 Lalu MM, Fayad A, Ahmed O, Bryson GL, Fergusson DA, Barron CC, Sullivan P, Thompson C; Canadian Perioperative Anesthesia Clinical Trials Group: Ultrasoundguided subclavian vein catheterization: a systematic review and meta-analysis. Crit Care Med 2015;43:1498–1507. [ Links ]
25 Stolz LA, Stolz U, Howe C, Farrell IJ, Adhikari S: Ultrasound-guided peripheral venous access: a meta-analysis and systematic review. J Vasc Access 2015;16:321–326. [ Links ]
26 Byon HJ, Lee GW, Lee JH, Park YH, Kim HS, Kim CS, Kim JT: Comparison between ultrasound-guided supraclavicular and infraclavicular approaches for subclavian venous catheterization in children – a randomized trial. Br J Anaesth 2013;111:788–792. [ Links ]
27 Rabindranath KS, Kumar E, Shail R, Vaux E: Use of real-time ultrasound guidance for the placement of hemodialysis catheters: a systematic review and meta-analysis of randomized controlled trials. Am J Kidney Dis 2011;58:964–970. [ Links ]
28 Ramirez-Schrempp D, Dorfman DH, Tien I, Liteplo AS: Bedside ultrasound in pediatric emergency medicine fellowship programs in the United States: little formal training. Pediatr Emerg Care 2008;24:664–667. [ Links ]
29 Macaluso CR, McNamara RM: Evaluation and management of acute abdominal pain in the emergency department. Int J Gen Med 2012;5:789–797. [ Links ]
30 Pidgeon TE, Shariff U, Devine F, Menon V: A report on an acute, in-hours, outpatient review clinic with ultrasonography facilities for the early evaluation of general surgical patients. Ann R Coll Surg Engl 2016;98:468–474. [ Links ]
31 Yim ES, Corrado G: Ultrasound in athletes: emerging techniques in point-of-care practice. Curr Sports Med Rep 2012;11:298–303. [ Links ]
32 Wagner MS, Garcia K, Martin DS: Point-ofcare ultrasound in aerospace medicine: known and potential applications. Aviat Space Environ Med 2014;85:730–739. [ Links ]
33 Mair F, Fraser S, Ferguson J, Webster K: Telemedicine via satellite to support offshore oil platforms. J Telemed Telecare 2008;14:129–131. [ Links ]
34 McBeth PB, Crawford I, Blaivas M, Hamilton T, Musselwhite K, Panebianco N, Melniker L, Ball CG, Gargani L, Gherdovich C, Kirkpatrick AW: Simple, almost anywhere, with almost anyone: remote low-cost telementored resuscitative lung ultrasound. J Trauma 2011;71:1528–1535. [ Links ]
35 Rabindranath KS, Kumar E, Shail R, Vaux EC: Ultrasound use for the placement of haemodialysis catheters. Cochrane Database Syst Rev 2011;CD005279. [ Links ]
36 Kristensen MS, Teoh WH, Graumann O, Laursen CB: Ultrasonography for clinical decision-making and intervention in airway management: from the mouth to the lungs and pleurae. Insights Imaging 2014;5:253–279. [ Links ]
37 Nassour I, Spalding MC, Hynan LS, Gardner AK, Williams BH: The surgeon-performed ultrasound: a curriculum to improve residents basic ultrasound knowledge. J Surg Res 2017;213:51–59. [ Links ]
38 Ultrasound Training Recommendations for Medical and Surgical Specialties, ed 3. The Royal College of Gastroenterologists, 2017. [ Links ]
39 Grubel P: Evaluation of abdominal ultrasound performed by the gastroenterologist in the office. J Clin Gastroenterol 2011;45:405–409. [ Links ]
40 Atkinson NS, Bryant RV, Dong Y, Maaser C, Kucharzik T, Maconi G, Asthana AK, Blaivas M, Goudie A, Gilja OH, Nolsoe C, Nurnberg D, Dietrich CF: WFUMB position paper. Learning gastrointestinal ultrasound: theory and practice. Ultrasound Med Biol 2016;42:2732–2742. [ Links ]
41 Rettenmaier G: Sonography in gastroenterology (in German). ZFA (Stuttgart) 1979;55:695–705. [ Links ]
42 Gandolfi L, Mazziotti A, Caletti GC, Bolondi L, Gozzetti G: The role of gastroenterologists and digestive surgeons in ultrasonography. Ital J Gastroenterol 1992;24:225–229. [ Links ]
43 Nylund K, Maconi G, Hollerweger A, Ripolles T, Pallotta N, Higginson A, Serra C, Dietrich CF, Sporea I, Saftoiu A, Dirks K, Hausken T, Calabrese E, Romanini L, Maaser C, Nuernberg D, Gilja OH: EFSUMB recommendations and guidelines for gastrointestinal ultrasound. Ultraschall Med 2017;38:e1–e15. [ Links ]
44 Odegaard S, Nesje LB, Hausken T, Gilja OH: Ultrasonography in gastroenterology. Scand J Gastroenterol 2015;50:698–707. [ Links ]
45 Bota S, Piscaglia F, Marinelli S, Pecorelli A, Terzi E, Bolondi L: Comparison of international guidelines for noninvasive diagnosis of hepatocellular carcinoma. Liver Cancer 2012;1:190–200. [ Links ]
46 Boal Carvalho P, Pereira E: Imagiological diagnosis of gastrointestinal diseases – diagnostic criteria of hepatocellular carcinoma. GE Port J Gastroenterol 2015;22:153–160. [ Links ]
47 European Association for the Study of the Liver; European Organisation for Research and Treatment of Cancer: EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. Eur J Cancer 2012;48:599–641. [ Links ]
48 Heimbach JK, Kulik LM, Finn R, Sirlin CB, Abecassis M, Roberts LR, Zhu A, Murad MH, Marrero J: AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018;67:358–380. [ Links ]
49 Sconfienza LM, Cavallaro F, Colombi V, Pastorelli L, Tontini G, Pescatori L, Esseridou A, Savarino E, Messina C, Casale R, Di Leo G, Sardanelli F, Vecchi M: In-vivo axial-strain sonoelastography helps distinguish acutely-inflamed from fibrotic terminal ileum strictures in patients with Crohns disease: preliminary results. Ultrasound Med Biol 2016;42:855–863. [ Links ]
50 Migaleddu V, Scanu AM, Quaia E, Rocca PC, Dore MP, Scanu D, Azzali L, Virgilio G: Contrast-enhanced ultrasonographic evaluation of inflammatory activity in Crohns disease. Gastroenterology 2009;137:43–52. [ Links ]
51 Gaitini D, Kreitenberg AJ, Fischer D, Maza I, Chowers Y: Color-coded duplex sonography compared to multidetector computed tomography for the diagnosis of Crohn disease relapse and complications. J Ultrasound Med 2011;30:1691–1699. [ Links ]
52 Coelho R, Ribeiro H, Maconi G: Bowel thickening in Crohns disease: fibrosis or inflammation? Diagnostic ultrasound imaging tools. Inflamm Bowel Dis 2017;23:23–34. [ Links ]
53 Calabrese E, Maaser C, Zorzi F, Kannengiesser K, Hanauer SB, Bruining DH, Iacucci M, Maconi G, Novak KL, Panaccione R, Strobel D, Wilson SR, Watanabe M, Pallone F, Ghosh S: Bowel ultrasonography in the management of Crohns disease. A review with recommendations of an international panel of experts. Inflamm Bowel Dis 2016;22:1168–1183. [ Links ]
54 Panes J, Bouhnik Y, Reinisch W, Stoker J, Taylor SA, Baumgart DC, Danese S, Halligan S, Marincek B, Matos C, Peyrin-Biroulet L, Rimola J, Rogler G, van Assche G, Ardizzone S, BaSsalamah A, Bali MA, Bellini D, Biancone L, Castiglione F, Ehehalt R, Grassi R, Kucharzik T, Maccioni F, Maconi G, Magro F, Martin-Comin J, Morana G, Pendse D, Sebastian S, Signore A, Tolan D, Tielbeek JA, Weishaupt D, Wiarda B, Laghi A: Imaging techniques for assessment of inflammatory bowel disease: joint ECCO and ESGAR evidence-based consensus guidelines. J Crohns Colitis 2013;7:556–585. [ Links ]
55 Gomollon F, Dignass A, Annese V, Tilg H, Van Assche G, Lindsay JO, Peyrin-Biroulet L, Cullen GJ, Daperno M, Kucharzik T, Rieder F, Almer S, Armuzzi A, Harbord M, Langhorst J, Sans M, Chowers Y, Fiorino G, Juillerat P, Mantzaris GJ, Rizzello F, Vavricka S, Gionchetti P; ECCO: 3rd European evidencebased consensus on the diagnosis and management of Crohns Disease 2016: part 1: diagnosis and medical management. J Crohns Colitis 2017;11:3–25. [ Links ]
56 Sidhu PS, Brabrand K, Cantisani V, Correas JM, Cui XW, DOnofrio M, Essig M, Freeman S, Gilja OH, Gritzmann N, Havre RF, Ignee A, Jenssen C, Kabaalioglu A, Lorentzen T, Mohaupt M, Nicolau C, Nolsoe CP, Nurnberg D, Radzina M, Saftoiu A, Serra C, Sparchez Z, Sporea I, Dietrich CF: EFSUMB guidelines on interventional ultrasound (INVUS), part II. Diagnostic ultrasound-guided interventional procedures (long version). Ultraschall Med 2015;36:E15–E35. [ Links ]
57 Lorentzen T, Nolsoe CP, Ewertsen C, Nielsen MB, Leen E, Havre RF, Gritzmann N, Brkljacic B, Nurnberg D, Kabaalioglu A, Strobel D, Jenssen C, Piscaglia F, Gilja OH, Sidhu PS, Dietrich CF; EFSUMB: EFSUMB guidelines on interventional ultrasound (INVUS), part I. General aspects (long version). Ultraschall Med 2015;36:E1–E14. [ Links ]
58 Dietrich CF, Lorentzen T, Appelbaum L, Buscarini E, Cantisani V, Correas JM, Cui XW, DOnofrio M, Gilja OH, Hocke M, Ignee A, Jenssen C, Kabaalioglu A, Leen E, Nicolau C, Nolsoe CP, Radzina M, Serra C, Sidhu PS, Sparchez Z, Piscaglia F: EFSUMB guidelines on interventional ultrasound (INVUS), part III – abdominal treatment procedures (long version). Ultraschall Med 2016;37:E1–E32. [ Links ]
59 European Federation of Societies for Ultrasound in Medicine (EFSUMB): Minimum training recommendations for the practice of medical ultrasound. Ultraschall Med 2006;27:79–105. [ Links ]
60 Atkinson NSS, Bryant RV, Dong Y, Maaser C, Kucharzik T, Maconi G, Asthana AK, Blaivas M, Goudie A, Gilja OH, Nuernberg D, Schreiber-Dietrich D, Dietrich CF: How to perform gastrointestinal ultrasound: anatomy and normal findings. World J Gastroenterol 2017;23:6931–6941. [ Links ]
61 Claudon M, Dietrich CF, Choi BI, Cosgrove DO, Kudo M, Nolsoe CP, Piscaglia F, Wilson SR, Barr RG, Chammas MC, Chaubal NG, Chen MH, Clevert DA, Correas JM, Ding H, Forsberg F, Fowlkes JB, Gibson RN, Goldberg BB, Lassau N, Leen EL, Mattrey RF, Moriyasu F, Solbiati L, Weskott HP, Xu HX: Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver – update 2012: a WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med 2013;34:11–29. [ Links ]
62 Nolsoe CP, Lorentzen T: International guidelines for contrast-enhanced ultrasonography: ultrasound imaging in the new millennium. Ultrasonography 2016;35:89–103. [ Links ]
63 Piscaglia F, Nolsoe C, Dietrich CF, Cosgrove DO, Gilja OH, Bachmann Nielsen M, Albrecht T, Barozzi L, Bertolotto M, Catalano O, Claudon M, Clevert DA, Correas JM, DOnofrio M, Drudi FM, Eyding J, Giovannini M, Hocke M, Ignee A, Jung EM, Klauser AS, Lassau N, Leen E, Mathis G, Saftoiu A, Seidel G, Sidhu PS, ter Haar G, Timmerman D, Weskott HP: The EFSUMB guidelines and recommendations on the clinical practice of contrast enhanced ultrasound (CEUS): update 2011 on non-hepatic applications. Ultraschall Med 2012;33:33–59. [ Links ]
64 Fraquelli M, Sarno A, Girelli C, Laudi C, Buscarini E, Villa C, Robotti D, Porta P, Cammarota T, Ercole E, Rigazio C, Senore C, Pera A, Malacrida V, Gallo C, Maconi G: Reproducibility of bowel ultrasonography in the evaluation of Crohns disease. Dig Liver Dis 2008;40:860–866. [ Links ]
65 Castiglione F, de Sio I, Cozzolino A, Rispo A, Manguso F, Del Vecchio Blanco G, Di Girolamo E, Castellano L, Ciacci C, Mazzacca G: Bowel wall thickness at abdominal ultrasound and the one-year-risk of surgery in patients with Crohns disease. Am J Gastroenterol 2004;99:1977–1983. [ Links ]
66 Shiina T, Nightingale KR, Palmeri ML, Hall TJ, Bamber JC, Barr RG, Castera L, Choi BI, Chou YH, Cosgrove D, Dietrich CF, Ding H, Amy D, Farrokh A, Ferraioli G, Filice C, Friedrich-Rust M, Nakashima K, Schafer F, Sporea I, Suzuki S, Wilson S, Kudo M: WFUMB guidelines and recommendations for clinical use of ultrasound elastography: part 1: basic principles and terminology. Ultrasound Med Biol 2015;41:1126–1147. [ Links ]
67 Cosgrove D, Piscaglia F, Bamber J, Bojunga J, Correas JM, Gilja OH, Klauser AS, Sporea I, Calliada F, Cantisani V, DOnofrio M, Drakonaki EE, Fink M, Friedrich-Rust M, Fromageau J, Havre RF, Jenssen C, Ohlinger R, Saftoiu A, Schaefer F, Dietrich CF; EFSUMB: EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: clinical applications. Ultraschall Med 2013;34:238–253. [ Links ]
68 Bamber J, Cosgrove D, Dietrich CF, Fromageau J, Bojunga J, Calliada F, Cantisani V, Correas JM, DOnofrio M, Drakonaki EE, Fink M, Friedrich-Rust M, Gilja OH, Havre RF, Jenssen C, Klauser AS, Ohlinger R, Saftoiu A, Schaefer F, Sporea I, Piscaglia F: EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 1: basic principles and technology. Ultraschall Med 2013;34:169–184. [ Links ]
69 Ferraioli G, Filice C, Castera L, Choi BI, Sporea I, Wilson SR, Cosgrove D, Dietrich CF, Amy D, Bamber JC, Barr R, Chou YH, Ding H, Farrokh A, Friedrich-Rust M, Hall TJ, Nakashima K, Nightingale KR, Palmeri ML, Schafer F, Shiina T, Suzuki S, Kudo M: WFUMB guidelines and recommendations for clinical use of ultrasound elastography: part 3: liver. Ultrasound Med Biol 2015;41:1161–1179. [ Links ]
70 Dietrich CF, Barr RG, Farrokh A, Dighe M, Hocke M, Jenssen C, Dong Y, Saftoiu A, Havre RF: Strain elastography – how to do it? Ultrasound Int Open 2017;3:E137–E149. [ Links ]
71 Dietrich CF, Bamber J, Berzigotti A, Bota S, Cantisani V, Castera L, Cosgrove D, Ferraioli G, Friedrich-Rust M, Gilja OH, Goertz RS, Karlas T, de Knegt R, de Ledinghen V, Piscaglia F, Procopet B, Saftoiu A, Sidhu PS, Sporea I, Thiele M: EFSUMB guidelines and recommendations on the clinical use of liver ultrasound elastography, update 2017 (long version). Ultraschall Med 2017;38:e16–e47. [ Links ]
72 Baumgart DC, Muller HP, Grittner U, Metzke D, Fischer A, Guckelberger O, Pascher A, Sack I, Vieth M, Rudolph B: US-based realtime elastography for the detection of fibrotic gut tissue in patients with stricturing Crohn disease. Radiology 2015;275:889–899. [ Links ]
73 Fufezan O, Asavoaie C, Tamas A, Farcau D, Serban D: Bowel elastography – a pilot study for developing an elastographic scoring system to evaluate disease activity in pediatric Crohns disease. Med Ultrason 2015;17:422–430. [ Links ]
74 Fraquelli M, Branchi F, Cribiu FM, Orlando S, Casazza G, Magarotto A, Massironi S, Botti F, Contessini-Avesani E, Conte D, Basilisco G, Caprioli F: The role of ultrasound elasticity imaging in predicting ileal fibrosis in Crohns disease patients. Inflamm Bowel Dis 2015;21:2605–2612. [ Links ]
75 The ESBGH Training Programme – The Blue Book: Speciality Training Programme and Curriculum for Gastroenterology and Hepatology. The European Section and Board of Gastroenterology and Hepatology, 2017. http://www.eubogh.org/blue-book. [ Links ]
76 Bisschops R, Areia M, Coron E, Dobru D, Kaskas B, Kuvaev R, Pech O, Ragunath K, Weusten B, Familiari P, Domagk D, Valori R, Kaminski MF, Spada C, Bretthauer M, Bennett C, Senore C, Dinis-Ribeiro M, Rutter MD: Performance measures for upper gastrointestinal endoscopy: a European Society of Gastrointestinal Endoscopy (ESGE) quality improvement initiative. Endoscopy 2016;48:843–864. [ Links ]
77 Kaminski MF, Thomas-Gibson S, Bugajski M, Bretthauer M, Rees CJ, Dekker E, Hoff G, Jover R, Suchanek S, Ferlitsch M, Anderson J, Roesch T, Hultcranz R, Racz I, Kuipers EJ, Garborg K, East JE, Rupinski M, Seip B, Bennett C, Senore C, Minozzi S, Bisschops R, Domagk D, Valori R, Spada C, Hassan C, Dinis-Ribeiro M, Rutter MD: Performance measures for lower gastrointestinal endoscopy: a European Society of Gastrointestinal Endoscopy (ESGE) quality improvement initiative. Endoscopy 2017;49:378–397. [ Links ]
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. João Sebastião Lopes Dias Pinto
Gastroenterology Department, Amato Lusitano Hospital
Avenida Pedro Álvares Cabral
PT–6000-085 Castelo Branco (Portugal)
E-Mail jsdiaspinto@gmail.com
Received: December 22, 2017; Accepted after revision: January 24, 2018

