










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.3 Lisboa jun. 2018
https://doi.org/10.1159/000478943
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Early Presentation of Buried Bumper Syndrome
Síndrome da Campânula Interna: Apresentação Precoce
Richard Azevedo, Ana Caldeira, António Banhudo
Department of Gastroenterology, Amato Lusitano Hospital, Castelo Branco, Portugal
* Corresponding author.
Keywords: Buried bumper syndrome, Percutaneous endoscopic gastrostomy, Early presentation, Complication
Palavras-Chave: Síndrome campânula interna, Gastrostomia endoscópica percutânea, Apresentação precoce,·Complicação
Case Report
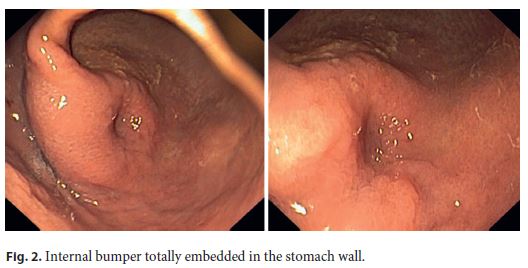
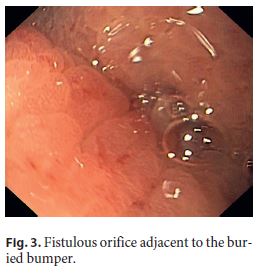
A 71-year-old female with Alzheimer disease, submitted to a percutaneous endoscopic gastrostomy (PEG) 3 days before, without immediate complications, presented to the emergency department with acute abdominal pain, exacerbated by attempts to infuse feeding solution through the tube. Stoma showed no signs of infection or peristomal leakage (Fig. 1). The external bumper was juxtaposed to the skin surface and it was not possible to mobilize the tube. Flushing the tube with water was difficult and exacerbated the patient complaints. On gastroscopy, the internal bumper was not visible, and the anterior face of the stomach showed an elevated round area with normal mucosa and a central depression, compatible with the internal bumper totally embedded in the stomach wall (Fig. 2). After water instillation, a fistulous orifice adjacent to the bulging area was identified (Fig. 3). As the internal bumper was collapsible, it was removed by simple external traction under endoscopic control, without resistance and with no signs of complications on the stomach wall. Introduction of a Foley catheter through the PEG orifice under endoscopic visualization was attempted without success, probably due to the creation of an alternative tract on the gastric wall.

The patient referred significant pain relief after the procedure and was admitted to the gastroenterology department for surveillance and antibiotic prophylaxis with ciprofloxacin for 5 days.
As the patient still maintained some oral intake, it was decided to perform fractional diet with oral nutritional supplements and intravenous fluids.
Follow-up abdominal ultrasound performed 24 h after gastrostomy tube removal and immediately before discharge showed the previous tube and bumper tract, with no signs of complications (Fig. 4).

According to the will of the patient and her family, a new PEG was not performed. The patient was discharged 5 days after admission, with a follow-up consultation in order to schedule a new procedure.
Discussion
PEG is a relatively safe and effective method of nutrition delivery for patients who require long-term enteral nutrition [1]. Major complications related to the procedure are rare. Buried bumper syndrome represents a severe complication, occurring in 0.3–2.4% of the patients [1], as a consequence of excessive compression of the tissue between the external and internal fixation bumpers [2] in which the internal bumper migrates and becomes lodged anywhere between the gastric wall and the skin along the PEG tract [3]. Although it usually corresponds to a late complication [2], months to years after placement, it can also occur in an acute (<30 days after placement) [1] setting. This is the earliest case reported in theliterature [1, 4]. Early diagnosis and prompt management are required to avoid further complications [2].
The removal method will depend on the type of the PEG set and the depth of disc migration. In this particular case, as the PEG system was equipped with a soft internal retention device, it was safely amenable to simple pulling extraction without resistance, with no potential complications apart from slight bleeding.
References
1 Cyrany J, Rejchrt S, Kopacova M, Bures J: Buried bumper syndrome: A complication of percutaneous endoscopic gastrostomy. World J Gastroenterol 2016;22:618–627. [ Links ]
2 Lucendo AJ, Friginal-Ruiz AB: Percutaneous endoscopic gastrostomy: an update on its indications, management, complications, and care. Rev Esp Enferm Dig 2014;106:529–539. [ Links ]
3 Schrag SP, et al: Complications related to percutaneous endoscopic gastrostomy (PEG) tubes. A comprehensive clinical review. J Gastrointestin Liver Dis 2007;16:407–418. [ Links ]
4 Afifi I, Zarour A, Al-Hassani A, Peralta R, El- Menyar A, Al-Thani H: The challenging buried bumper syndrome after percutaneous endoscopic gastrostomy. Case Rep Gastroenterol 2016;10:224–232. [ Links ]
Statement of Ethics
This study did not require informed consent or review/approval by the appropriate ethics committee.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. Richard Azevedo
Department of Gastroenterology, Amato Lusitano Hospital
Avenida Pedro Álvares Cabral
PT–6000-085 Castelo Branco (Portugal)
E-Mail richardazevedo13@gmail.com
Received: March 31, 2017; Accepted after revision: June 5, 2017

