










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.24 no.4 Lisboa ago. 2017
https://doi.org/10.1159/000453070
ENDOSCOPIC SNAPSHOT
Jejunal Stent-in-Stent for Recurrent Malignant Occlusion Using Single-Balloon Enteroscopy
Prótese-sobre-prótese jejunal para recorrência de oclusão maligna usando enteroscopia de monobalão
Ana Pontea, Rolando Pinhoa, Adélia Rodriguesa, Luísa Proençaa, Alexandre Costab, João Carvalhoa
Departments of aGastroenterology and bGeneral Surgery, Centro Hospitalar Vila Nova de Gaia, Vila Nova Gaia, Portugal
* Corresponding author.
Keywords: Deep enteroscopy; Stents; Malignant occlusion
Palavras-Chave: Enteroscopia profunda; Próteses; Oclusão maligna
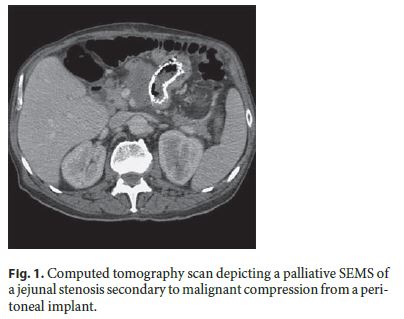
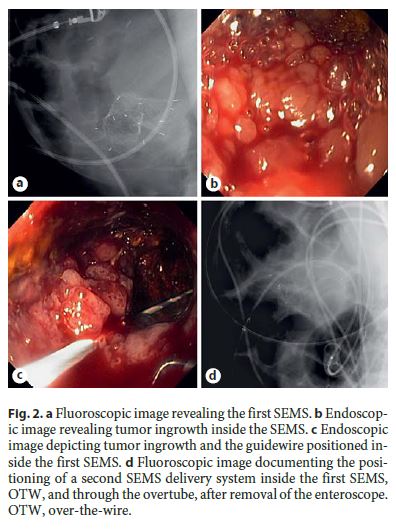
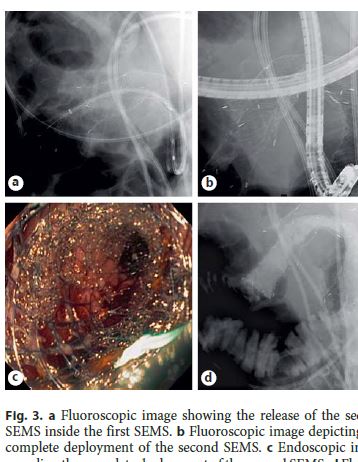
We describe the case of a 75-year-old man previously submitted to palliative stenting of an occlusive jejunal stenosis secondary to malignant compression from a peritoneal implant of a metastatic cholangiocarcinoma (Fig. 1) [1]. After remaining asymptomatic for 5 months after stenting, the patient was admitted with a 4-day history of persistent vomiting and abdominal pain. Single-balloon enteroscopy (SIF-Q180; Olympus, Tokyo, Japan) was performed for diagnostic evaluation and further therapeutic management, revealing gastric and duodenal stasis. The enteroscope was advanced to the proximal jejunum where the previously placed noncovered self-expandable metallic stent (SEMS) was identified. Despite remaining properly positioned inside the stenosis (Fig. 2a), the lumen of the proximal part of the SEMS was partially occluded by tumor ingrowth (Fig. 2b). The enteroscope was advanced into the SEMS through the stenosis, and a 0.035-inch guidewire was then advanced into the first SEMS (Fig. 2c). The overtube (ST-SB1; Olympus) was positioned at the proximal end of the first SEMS. After withdrawing the enteroscope leaving the guidewire in place, a second noncovered SEMS (Hanarostent, DNZL-20-140-230; M.I. Tech Co., Seoul, Republic of Korea) was easily advanced over-the-wire (OTW) through the overtube (Fig. 2d) and subsequently deployed inside the first SEMS under fluoroscopic guidance (Fig. 3a–d), while the overtube was slightly pulled back (the same technique used in the deployment of the first SEMS). The palliative stent-in-stent resulted in immediate resolution of the occlusive symptoms and resumption of oral diet with tolerance.
Placement of SEMS using deep enteroscopy is technically challenging because enteral stents have a delivery system which is larger and shorter than the working channel of the enteroscope, thus preventing the use of the through-the-scope technique, which is the preferred approach in strictures located distant from the insertion route [2–5]. To overcome these limitations, the adaptation of an overtube to the OTW technique may prevent kinking of the delivery system, as the overtube will have a similar role to a working channel [2]. This modified OTW technique allows the placement of SEMS in the small bowel using deep enteroscopy [1].
References
1 Ponte A, Pinho R, Proença L, Bernardes C, Costa A, Francisco E, et al: Palliative stenting of a jejunal stricture secondary to malignant compression using single-balloon enteroscopy. Gastroenterol Hepatol 2016, Epub ahead of print. [ Links ]
2 Pinho R, Proença L, Ponte A, Fernandes C, Ribeiro I, Silva J, et al: Balloon overtube-assisted stenting in difficult upper and lower gastrointestinal locations using a modified over-the-wire technique. Endoscopy 2015;47:266–271. [ Links ]
3 Park JJ, Cheon JH: Malignant small bowel obstruction: the last frontier for gastrointestinal stenting. J Gastroenterol Hepatol 2012;27:1136–1137. [ Links ]
4 Kida A, Matsuda K, Noda Y: Endoscopic metallic stenting by double-balloon enteroscopy and its overtube for malignant gastrointestinal obstruction as palliative treatment. Dig Endosc 2013;25:552–553. [ Links ]
5 Pinho R, Proença L, Alberto L, Carvalho J, Pinto-Pais T, Fernandes C, et al: Biliary self-expandable metallic stent using single balloon enteroscopy assisted ERCP-overcoming limitations of current accessories. Rev Esp Enferm Dig 2013;105:561–564. [ Links ]
Statement of Ethics
Protection of human and animal subjects: the authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data: the authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent: the authors declare that no patient data appear in this article.
Disclosure Statement
The authors have nothing to disclose.
* Corresponding author.
Dr. Ana Ponte
Department of Gastroenterology, Centro Hospitalar Vila Nova de Gaia
Rua Conceição Fernandes
PT–4434-502 Vila Nova Gaia (Portugal)
E-Mail ana.ilponte@gmail.com
Received: September 26, 2016; Accepted after revision: November 4, 2016

