










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.24 no.4 Lisboa ago. 2017
https://doi.org/10.1159/000453271
REVIEW ARTICLE
Endoscopic Treatment for Gastric Antral Vascular Ectasia: Current Options
Ectasia Vascular do Antro Gástrico (GAVE): Opções Atuais
Sergio Zepeda-Gómez
Division of Gastroenterology, University of Alberta, Edmonton, AB, Canada
* Corresponding author.
ABSTRACT
Gastric antral vascular ectasia (GAVE) is a capillary-type vascular malformation located primarily in the gastric antrum. Patients can present with iron-deficiency anemia, overt gastrointestinal bleeding, or both. Diagnosis and characterization is made at endoscopic examination, and the preferred management of patients with GAVE is endoscopic therapy. Herein, we present a review of the evidence about the efficacy, complications, and outcomes of the most frequently used endoscopic therapies for GAVE.
Keywords: Gastric antral vascular ectasia; Endoscopy; Gastrointestinal bleeding; Stomach
RESUMO
A ectasia vascular do antro gástrico (GAVE) é uma malformação vascular do tipo capilar formada no antro e que se organiza sob a forma de estrias ou de forma difusa. A GAVE pode causar uma anemia ferropénica com ou sem hemorragia gastrointestinal evidente. O tratamento da GAVE inclui abordagens cirúrgicas e farmacológicas, contudo, a terapêutica endoscópica provou ser a mais eficaz e segura. Várias terapêuticas endoscópicas foram descritas. A coagulação com árgon plasma (APC) tem sido a terapêutica endoscópica mais descrita e utilizada, no entanto, estudos recentes mostram que a laqueação por banda elástica e a ablação por radiofrequência são terapêuticas promissoras com uma eficácia a curto prazo que pode ser superior à APC. O objectivo deste artigo é rever a evidência sobre a eficácia, complicações e resultados a longo prazo das terapêuticas endoscópicas mais frequentemente utilizadas para o tratamento da GAVE.
Palavras-Chave: Ectasia vascular do antro; Endoscopia; Hemorragia digestiva; Estômago
Introduction
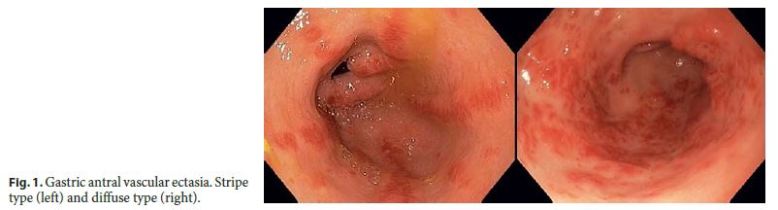
Gastric antral vascular ectasia (GAVE) is a capillary-type vascular malformation characterized endoscopically by red, angiomatous lesions originating in the antrum and organized either in stripes or in a diffuse pattern [1] (Fig. 1). Histologically, GAVE presents as dilated, tortuous mucosal capillaries, which are often occluded by thrombus and associated with dilated, tortuous submucosal veins. In general, it is uncommon to see inflammatory changes [2]. GAVE may cause chronic iron-deficiency anemia with or without the presence of overt gastrointestinal (GI) bleeding, manifested commonly by melena. Many patients may require frequent blood transfusions or iron supplementation to maintain adequate hemoglobin levels. GAVE can be isolated or associated with systemic conditions, especially in patients with liver cirrhosis, scleroderma, chronic renal failure, and after bone marrow transplantation. GAVE may account for about 4% of the causes of non-variceal bleeding [3]. The pathophysiology of GAVE is unknown; however, multiple mechanisms have been proposed as the origin of its development. These have included gastric dysmotility leading to chronic mucosal trauma and subsequent fibromuscular hyperplasia and vascular ectasia or an autoimmune reaction to gastric blood vessels among the main contributing factors [4–6].
The management of GAVE has included surgical, pharmacological, and endoscopic therapy. Surgical therapy (antrectomy) carries high morbidity and mortality, especially in patients with liver cirrhosis, and has therefore been reserved for refractory cases only. The evidence for the effectiveness of medical treatment is very limited, there are no studies with comparators, and only 1 case series with a low number of patients has been published (estrogen and progesterone treatment) [7]. Endoscopic therapy has been the mainstay of treatment for GAVE; multiple modalities have been evaluated. Some of these (cryotherapy, Nd:YAG laser) are of limited use, mainly because they are not widely available or have been associated with a higher rate of complications (20–33%) [8–13].
The purpose of this paper is to review the evidence about the effectiveness, complications, and long-term outcomes of the most frequent endoscopic modalities currently used for the treatment of GAVE.
Endoscopic Treatment Options
There is only 1 case series on monopolar coagulation and 1 on heath probe for the treatment of GAVE. These included 6 and 12 patients, respectively. Both studies showed a complication rate of 33% [14, 15]. These endoscopic techniques are not performed routinely, since argon plasma coagulation (APC) has been the traditional method of choice. APC has been the endoscopic therapy most frequently utilized for GAVE; however, recent data shows that endoscopic band ligation (EBL) and radiofrequency ablation (RFA) are new, promising options for the treatment of this condition.
Argon Plasma Coagulation
APC is a non-contact thermal method that uses argon gas to deliver plasma of evenly distributed thermal energy to a field of tissue adjacent to the probe with a depth of penetration of roughly 2–3 mm. APC electrosurgical settings vary among studies regarding electrical power, gas flow, and type of APC delivery (pulse, forced coagulation, etc.). There is no data to support specific settings for GAVE; however, last-generation electrosurgical units have a pre-established setting for APC delivery in the stomach. APC has been the endoscopic treatment of choice for GAVE since its introduction; however, most of the published data in the literature are from retrospective case series (Table 1). In some of these studies, patients with angiodysplasias in the stomach were also included, the follow-up period was short, and the evaluation of efficacy and/or failure of therapy is not well defined. In general, patients have a good initial response with a low rate of complications. However, the recurrent bleeding rates can be high and in some studies are reported to range from 35 to 78.9% [16–26].
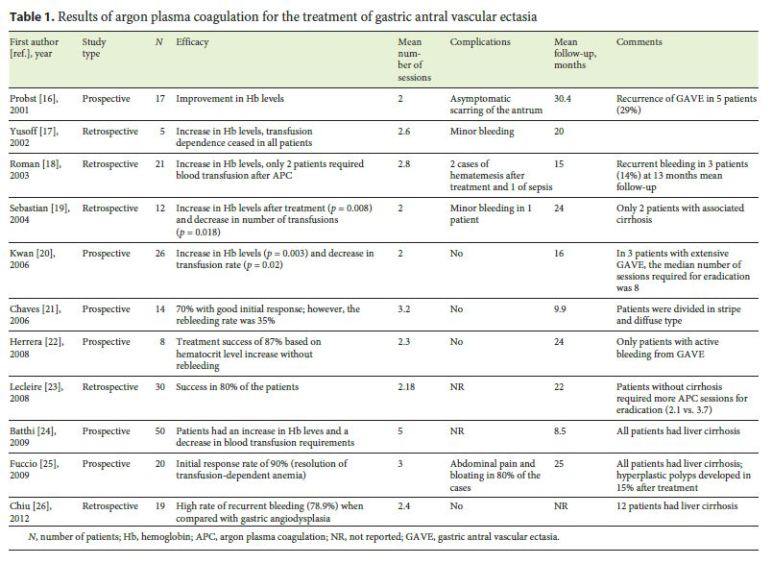
There are 2 studies that have evaluated long-term outcomes after APC treatment for GAVE. Boltin et al. [27] retrospectively identified patients who underwent APC treatment for GAVE with a mean follow-up of 46.9 ± 26.5 months. Treatment success was defined by resolution of the symptoms and stabilization of the hemoglobin level at 30% above baseline. Thirty-one patients were identified; the final analysis showed that treatment success was achieved in only 16 (25.8%) patients [27]. Another retrospective study that included 18 patients showed recurrent bleeding in 7 patients (39%) after a mean follow-up of 42 months [28].
Endoscopic Band Ligation
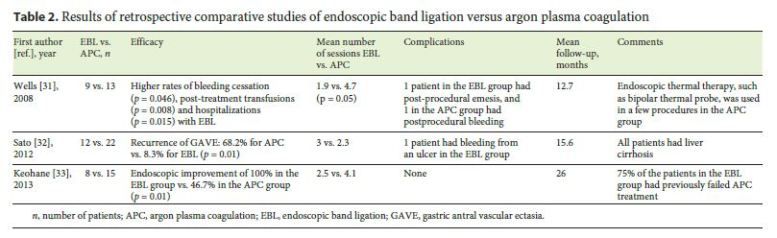
EBL was first reported for the treatment of GAVE in 2006. In 1 case, EBL was utilized as a salvage therapy in a patient who presented with recurrent melena and required blood transfusions. This was refractory after several sessions of APC therapy. After 2 sessions of EBL (the mean number of bands applied was 5.5) with an interval of 2 weeks, the hemoglobin levels increased and were stable without the need of further blood transfusions [29]. In a second report, EBL was performed as there was no availability of APC at the authors institution. The patient presented with signs of upper GI bleeding and anemia. Two sessions of EBL were performed with an interval of 6 weeks and application of 6 bands in each session. The hemoglobin levels stabilized, and the serum ferritin normalized [30]. Subsequently, 3 comparative studies of EBL versus APC were published; 1 study also included endoscopic thermal therapy along with APC [31–33]. The overall results of these studies showed better outcomes for the groups treated with EBL, including less transfusion requirements and stabilization of hemoglobin levels. However, these studies included a low number of patients and are all retrospective (Table 2).
The first prospective study about the efficacy of EBL in GAVE was published in 2015 [34]. This study included 21 consecutive patients. The clinical response to therapy was defined by eradication or near-eradication of GAVE along with stabilization of hemoglobin levels and/or a decrease in blood transfusion requirements. Patients received endoscopic treatment every 2 months and were under treatment with proton pump inhibitors during the study period. Clinical response was achieved in 91% of the patients after a mean of 2.2 sessions of endoscopic therapy (Fig. 2). Nine patients (43%) had previously failed endoscopic treatment with APC. The 2 patients who did not achieve complete clinical response had chronic renal failure as well as diffuse-type GAVE. Regarding complications, 2 patients experienced mild-to-moderate abdominal pain that disappeared 24 h later. Finally, a randomized controlled trial of EBL versus APC for GAVE has recently been published [35]. Eighty-eight patients (all cirrhotic) were included and randomized to receive endoscopic treatment every 2 weeks. The results showed a significantly lower number of endoscopic sessions required for eradication (2.98 vs. 3.48, p = <0.05) and a significant decrease in blood transfusion requirements (p = <0.05) in the EBL group. Both groups had a significant increase in hemoglobin levels, but without differences between them. In the EBL group, 13.6 % of the patients had adverse events, including fever, mild bleeding from a post-banding ulcer, and epigastric pain in 3 cases. In the APC group, 20.5% of the patients experienced adverse events: fever occurred in 2, abdominal distention in 4, and epigastric pain in 2 patients. There was no statistically significant difference between the groups.

Radiofrequency Ablation
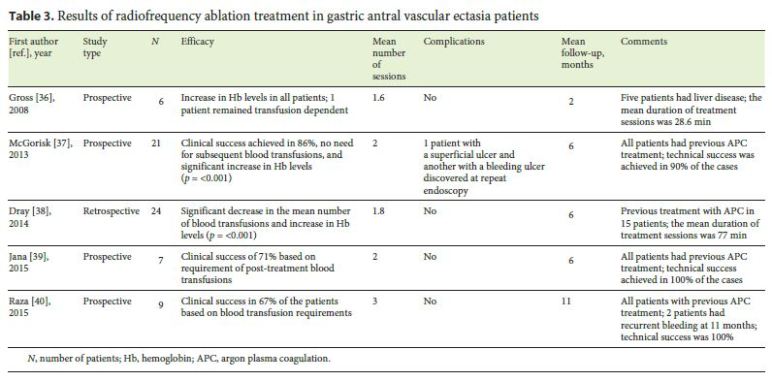
RFA is a technique that delivers rapid pulses of radiofrequency energy at a constant power of 40 W with variable energy densities, depending on the pathology being treated. This results in a uniform ablation depth of 0.5–1 mm, which involves only the superficial layer of the mucosa. RFA has been used for the ablation of dysplastic mucosa in Barretts esophagus and recently for the treatment of GAVE. RFA is a method that requires further training to familiarize with the technique. A pilot trial of RFA for the treatment of GAVE with the HALO90 ablation catheter that included 6 patients was published in 2008. This showed improvement of the hemoglobin levels after 1–3 treatment sessions, and 5 patients did not require subsequent blood transfusions [36]. Since then, 4 additional studies on the usefulness of RFA treatment in GAVE have been published. Table 3 shows a summary of the results of these trials [36–40]. The patients included in these trials had previous endoscopic treatment for GAVE, mainly APC. The overall clinical success rate ranged from 67 to 86%. Complications were mild; however, there is a recent report of a patient that experienced bacteremia and sepsis after RFA treatment for GAVE [41].
Discussion
Multiple types of endoscopic treatment have been used for GAVE. A recent systematic review regarding therapies for angiodysplasia and GAVE has shown a lack of good-quality studies (prospective and randomized trials) about endoscopic therapy for this condition [42]. Traditionally, APC has been the most frequently used modality; however, a considerable number of patients will not have a good initial response or will experience recurrence of anemia or bleeding at follow-up. This is also true for other GI angiodysplastic lesions, as shown in a recent systematic review that excluded patients with GAVE. The authors found that the pooled recurrence rate of bleeding was 36% [43]. Endoscopic therapy with EBL and RFA has recently shown promising results regarding efficacy and safety, but the long-term outcome of these modalities is still unknown. EBL may have the advantage over RFA that it is more widely available and is an easier technique to perform.
One of the drawbacks when analyzing the information from the current literature regarding endoscopic therapy for GAVE is that the definition of treatment success or clinical response varies widely among studies. Clinical response to endoscopic therapy should be defined by the increase or stabilization of hemoglobin and iron levels, along with a decrease or elimination of blood transfusions when patients are transfusion dependent. Complete or near-eradication of GAVE at the endoscopic examination should also be part of the definition. However, it is important to understand that near-eradication of GAVE does not mean failure to endoscopic therapy if the other endpoints are achieved. There is also a need for further information about the long-term response to therapy. Patients with GAVE will need regular determinations of hemoglobin and iron levels after endoscopic therapy to confirm response to treatment and to identify cases of recurrent bleeding and/or anemia from refractory GAVE. Patients with recurrence of symptoms may need to undergo further endoscopic examination and therapy. The clinical response to this approach needs to be established with a prospective, long-term follow-up study.
There is also not sufficient information about subgroups of patients with GAVE regarding differences in clinical response. For example, patients with comorbidities such as chronic renal failure or liver cirrhosis and patients under treatment with anticoagulation or antiplatelets may, in theory, have a poor clinical response when compared to patients without these conditions. In summary, GAVE can be a challenging condition when patients do not respond well to traditional endoscopic therapy. New endoscopic modalities for GAVE are available and promising. Nonetheless, there is need for high-quality, randomized prospective studies to confirm their efficacy and safety in the short and long term.
References
1 Ito M, Uchida Y, Kamano S, Kawabata H, Nishioka M: Clinical comparisons between two subsets of gastric antral vascular ectasia. Gastrointest Endosc 2001;53:764–770. [ Links ]
2 Jabbari M, Cherry R, Lough JO, Daly DS, Kinnear DG, Goresky CA: Gastric antral vascular ectasia: the watermelon stomach. Gastroenterol 1984;87:1165–1170. [ Links ]
3 Fuccio L, Mussetto A, Laterza L, Eusebi LH, Bazzoli F: Diagnosis and management of gastric antral vascular ectasia. World J Gastrointest Endosc 2013;5:6–13. [ Links ]
4 Charneau J, Petit R, Cales P, Dauver A, Boyer J. Antral motility in patients with cirrhosis with or without gastric antral vascular ectasia. Gut 1995;37:488–492. [ Links ]
5 Spahr L, Villeneuve JP, Dufresne MP, Tassé D, Bui B, Willems B, et al. Gastric antral vascular ectasia in cirrhotic patients: absence of relation with portal hypertension. Gut 1999;44:739–742. [ Links ]
6 Hung EW, Mayes MD, Sharif R, Assassi S, Machicao VI, Hosing C, et al: Gastric antral vascular ectasia and its clinical correlates in patients with early diffuse systemic sclerosis in the SCOT trial. J Rheumatol 2013;40:455–460. [ Links ]
7 Tran A, Villeneuve JP, Bilodeau M, Willems B, Marleau D, Fenyves D, et al: Treatment of chronic bleeding from gastric antral vascular ectasia (GAVE) with estrogen-progesterone in cirrhotic patients: an open pilot study. Am J Gastroenterol 1999;94:2909–2911. [ Links ]
8 Calamia KT, Scolapio JS, Viggiano TR. Endoscopic YAG laser treatment of watermelon stomach (gastric antral vascular ectasia) in patients with systemic sclerosis. Clin Exp Rheumatol 2000;18:605–608. [ Links ]
9 Geller A, Gostout CJ, Balm RK: Development of hyperplastic polyps following laser therapy for watermelon stomach. Gastrointest Endosc 1996;43:54–56. [ Links ]
10 Liberski SM, McGarrity TJ, Hartle RJ, Varano V, Reynolds D: The watermelon stomach: long-term outcome in patients treated with Nd:YAG laser therapy. Gastrointest Endosc 1994;40:584–587. [ Links ]
11 Potamiano S, Carter CR, Anderson JR: Endoscopic laser treatment of diffuse gastric antral vascular ectasia. Gut 1994;35:461–463. [ Links ]
12 Kantsevoy SV, Cruz-Correa MR, Vaughn CA, Jagannath SB, Pasricha PJ, Kalloo AN: Endoscopic cryotherapy for the treatment of bleeding mucosal vascular lesions of the GI tract: a pilot study. Gastrointest Endosc 2003;57:403–406. [ Links ]
13 Cho S, Zanati S, Yong E, Cirocco M, Kandel G, Kortan P, et al: Endoscopic cryotherapy for the management of gastric antral vascular ectasia. Gastrointest Endosc 2008;68:895–902. [ Links ]
14 Yamada M, Ichikawa M, Takahara O, Tsuchida T, Ishihara A, Yamada M, et al: Gastroduodenal vascular ectasia in patients with liver cirrhosis. Dig Endosc 1999;11:241–245. [ Links ]
15 Petrini JL, Johnston JH: Heath probe treatment for antral vascular ectasia. Gastrointest Endosc 1989;35:324–328. [ Links ]
16 Probst A, Scheubel R, Wienbeck M: Treatment of watermelon stomach (GAVE syndrome) by means of endoscopic argon plasma coagulation (APC): long term outcome. Z Gastroenterol 2001;39:447–452. [ Links ]
17 Yusoff I, Brennan F, Ormonde D, Laurence B: Argon plasma coagulation for the treatment of watermelon stomach. Endoscopy 2002; 34:407–410. [ Links ]
18 Roman S, Saurin JC, Dumortier J, Perreira A, Bernard G, Ponchon T: Tolerance and efficacy of argon plasma coagulation for controlling bleeding in patients with typical and atypical manifestations of watermelon stomach. Endoscopy 2003;35:1024–1028. [ Links ]
19 Sebastian S, McLoughlin R, Qasim A, OMorain CA, Buckley MJ: Endoscopic argon plasma coagulation for the treatment of gastric antral vascular ectasia (watermelon stomach): long-term results. Dig Liver Dis 2004;36:212–217. [ Links ]
20 Kwan V, Bourke MJ, Williams SJ, Gillespie PE, Murray MA, Kaffes AJ, et al: Argon plasma coagulation in the management of symptomatic gastrointestinal vascular lesions: experience in 100 consecutive patients with long-term follow-up. Am J Gastroenterol 2006;101:58–63. [ Links ]
21 Chaves D, Sakai P, Oliveira CV, Cheng S, Ishioka S: Watermelon stomach: clinical aspects and treatment with argon plasma coagulation. Arq Gastroenterol 2006;43:191–195. [ Links ]
22 Herrera S, Bordas JM, Llach J, Ginès A, Pellisé M, Fernández-Esparrach G, et al: The beneficial effects of argon plasma coagulation in the management of different types of gastric vascular ectasia lesions in patients admitted for GI hemorrhage. Gastrointest Endosc 2008;68:440–446. [ Links ]
23 Lecleire S, Ben-Soussan E, Antonietti M, Goria O, Riachi G, Lerebours E, et al: Bleeding gastric vascular ectasia treated by argon plasma coagulation: a comparison between patients with and without cirrhosis. Gastrointest Endosc 2008;67:219–225. [ Links ]
24 Batthi MA, Khan AA, Alam AK, Butt AK, Shafqat F, Malik K, et al: Efficacy of argon plasma coagulation in gastric vascular ectasia in patients with liver cirrhosis. J Coll Physicians Surg Pak 2009;19:219–222. [ Links ]
25 Fuccio L, Zagari RM, Serrani M, Eusebi LH, Grilli D, Cennamo V, et al: Endoscopic argon plasma coagulation for the treatment of gastric antral vascular ectasia-related bleeding in patients with liver cirrhosis. Digestion 2009;79:143–150. [ Links ]
26 Chiu YC, Lu LS, Wu KL, Tam W, Hu ML, Tai WC, et al: Comparison of argon plasma coagulation in management of upper gastrointestinal angiodysplasia and gastric antral vascularectasia hemorrhage. BMC Gastroenterol 2012;9:12: 67. [ Links ]
27 Boltin D, Gingold-Belfer R, Lichtenstein L, Levi Z, Niv Y: Long-term treatment outcome of patients with gastric antral vascular ectasia treated with argon plasma coagulation. Eur J Gastroenterol Hepatol 2014;26:588–593. [ Links ]
28 Baudet JS, Diaz-Bethencourt D, Soler M, Vela M, Morales S, Avilés J: Long-term follow-up of patients with gastric antral vascular ectasia treated with argon plasma coagulation. Med Clin (Barc) 2009;11:217–220. [ Links ]
29 Kumar R, Mohindra S, Pruthi HS: Endoscopic band ligation: a novel therapy for bleeding gastric antral vascular ectasia. Endoscopy 2007;39:E56–E57. [ Links ]
30 Sinha SK, Udawat HP, Varma S, Lal A, Rana SS, Bhasin DK: Watermelon stomach treated with endoscopic band ligation. Gastrointest Endosc 2006; 64: 1028–1031. [ Links ]
31 Wells CD, Harrison ME, Gurudu SR, Crowell MD, Byrne TJ, Depetris G, et al: Treatment of gastric antral vascular ectasia (watermelon stomach) with endoscopic band ligation. Gastrointest Endosc 2008;68:231–236. [ Links ]
32 Sato T, Yamazaki K, Akaike J: Endoscopic band ligation versus argon plasma coagulation for gastric antral vascular ectasia associated with liver diseases. Dig Endosc 2012;24:237–242. [ Links ]
33 Keohane J, Berro W, Harewood GC, Murray FE, Patchett SE: Band ligation of gastric antral vascular ectasia is a safe and effective endoscopic treatment. Dig Endosc 2013;25:392–396. [ Links ]
34 Zepeda-Gomez S, Sultanian R, Teshima CW, Sandha G, Van Zanten S, Montano-Loza AJ: Gastric antral vascular ectasia: a prospective study of treatment with endoscopic band ligation. Endoscopy 2015;47:538–540. [ Links ]
35 Elhendawy M, Mosaad S, Alkhalawany W, Abo-Ali L, Enaba M, Elsaka A, et al: Randomized controlled study of endoscopic band ligation and argon plasma coagulation in the treatment of gastric antral and fundal vascular ectasia. United European Gastroenterol J 2016;4:423–428. [ Links ]
36 Gross SA, Al-Haddad M, Gill KR, Schore AN, Wallace MB: Endoscopic mucosal ablation for the treatment of gastric antral vascular ectasia with the HALO90 system: a pilot study. Gastrointest Endosc 2008;67:324–327. [ Links ]
37 McGorisk T, Krishnan K, Keefer L, Komanduri S: Radiofrequency ablation for refractory gastric antral vascular ectasia (with video). Gastrointest Endosc 2013;78:584–588. [ Links ]
38 Dray X, Repici A, Gonzalez P, Fristrup C, Lecleire S, Kantsevoy S, et al: Radiofrequency ablation for the treatment of gastric antral vascular ectasia. Endoscopy 2014;46:963–969. [ Links ]
39 Jana T, Thosani N, Fallon M, Dupont AW, Ertan A: Radiofrequency ablation for treatment of refractory gastric antral vascular ectasia (with video). Endosc Int Open 2015;3:E125–E127. [ Links ]
40 Raza N, Diehl DL: Radiofrequency ablation of treatment-refractory gastric antral vascular ectasia (GAVE). Surg Laparosc Endosc Percutan Tech 2015;25:79–82. [ Links ]
41 Gaslightwala I, Diehl DL: Bacteremia and sepsis after radiofrequency ablation of gastric antral vascular ectasia. Gastrointest Endosc 2014;79:873–874. [ Links ]
42 Swanson E, Mahgoub A, MacDonald R, Shaukat A: Medical and Endoscopic therapies for angiodysplasia and gastric antral vascular ectasia: a systematic review. Clin Gastroenterol Hepatol 2014;12:571–582. [ Links ]
43 Jackson CS, Gerson LB: Management of gastrointestinal angiodysplastic lesions (GIADs): a systematic review and meta-analysis. Am J Gastroenterol 2014;109:474–483. [ Links ]
Statement of Ethics
The author declares that no experiments on humans or animals were performed for this study. Furthermore, he declares that they have followed the protocols of their work center on the publication of patient data and that no patient data appear in this article.
Disclosure Statement
The author has no conflicts of interest to declare.
* Corresponding author.
Dr. Sergio Zepeda-Gómez
Division of Gastroenterology, University of Alberta
1–20A Zeidler Ledcor Centre, 130 University Campus
Edmonton, AB T6G 2X8 (Canada)
E-Mail zepedago@ualberta.ca, zepedagomez@hotmail.com
Received: September 26, 2016; Accepted after revision: November 4, 2016

