










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.23 no.5 Lisboa out. 2016
https://doi.org/10.1016/j.jpge.2015.12.002
ENDOSCOPIC SNAPSHOT
Skin Metastases: The Visible Face of a Disastrous Unusual Finding
Metástases Cutâneas: A Face Visível de um Nefasto Achado Incomum
Sílvia Giestasa, * , Adriano Casela a, Cláudia Agostinho a, Paulo Souto a, Ernestina Camacho a, M. Julião b, Maria Augusta Cipriano b, Carlos Sofia a
a Gastroenterology Department, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
b Pathology Department, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
* Corresponding author.
Keywords: Carcinoma, Acinar Cell. Pancreatic Neoplasms. Skin Neoplasms/secondary.
Palavras-chave: Carcinoma de Células Acinares. Neoplasias Pancreáticas. Neoplasias da Pele/secundária.
1. Introduction
Acinar cell carcinoma (ACC) of the pancreas is a rare pancreatic malignancy, constituting only 1–2% of all exocrine pancreatic tumors.1–3 There is a slight male preponderance and it mostly presents in 5–7th decades of life. ACC arise more commonly from the head of the pancreas. Clinical symptoms are usually non-specific. In contrast to ductal adenocarcinoma, ACC rarely obstructs the common bile duct because it generally compresses and does not infiltrate into adjacent structures, so jaundice is infrequent (12%). It has a unique ability to produce pancreatic enzymes. Paraneoplastic syndrome may be the only presenting symptom in 15% of patients. Lipase hypersecretion syndrome characterized by subcutaneous fat necrosis, polyarthralgia and peripheral eosinophilia is a type of paraneoplastic syndrome associated with it. Skin nodules in this syndrome are commonly seen on the lower extremities and often mistaken for metastatic disease.1–3 Surgical resection is the best treatment for localized ACC but this is a highly aggressive tumor. Approximately 50% of the cases presented with metastasis at diagnosis. More than 70% the patients who undergo surgical resection are eventually confirmed to show recurrent disease.2,3 Chemotherapy and radiotherapy are therapeutic options when ACC is unresectable or recurs after resection, but no effective treatment strategies have been established. Although recent studies have clarified the characteristics of ACC it still has not been fully understood.4,5
We report a rare case of ACC with widespread metastases in a 35-year-old woman who presented with subcutaneous nodules as the initial symptom without evidence of subcutaneous fat necrosis. To our knowledge, this is the second report of ACC with skin metastases.3
2. Clinical case
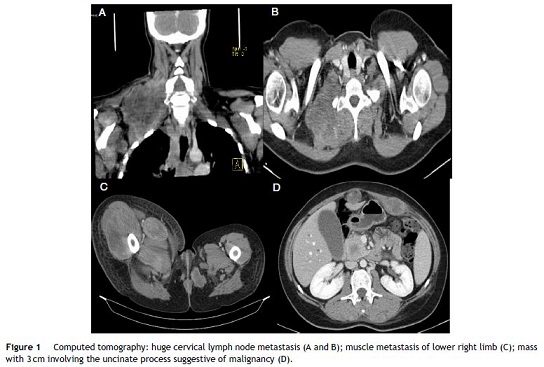
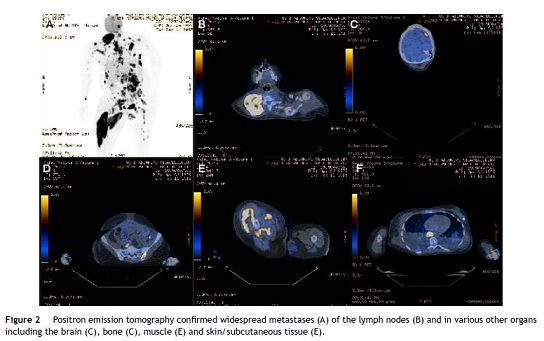
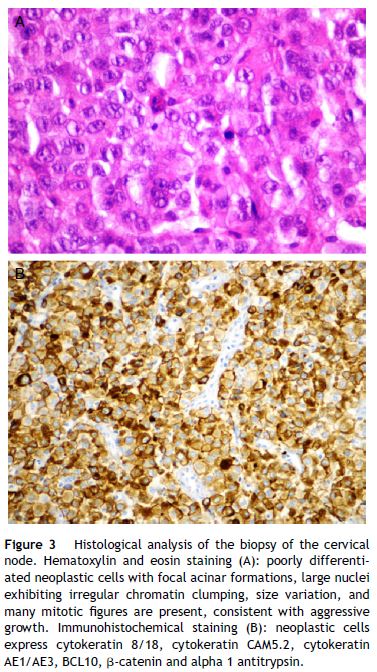
A 35-year-old woman presents with a one week history of jaundice, abdominal discomfort and intensive asthenia associated with abrupt growth of painful nodules in the neck, abdominal wall and lower right limb. No history of trauma and fever. Without significant previous medical history. She had a delivery eight months ago without complications. Laboratory tests showed cholestasis (gamma glutamyl transpeptidase 346 U/L (<55); alkaline phosphatase 230 U/L (40–150); total bilirubin 4.4 mg/dL (0.3–1.2); direct bilirubin 2.8 mg/dL (0.1–0.5)) without other alterations. Ultrasonography showed moderate dilatation of the main bile duct and could not define the cause of obstruction. Computed tomography revealed multiple metastases in the lymph nodes (the largest with 10 cm, Fig. 1A and B), in the skin/subcutaneous tissue, muscular (Fig. 1C) and also showed a 3 cm mass involving the uncinate process suggestive of neoplastic nature (Fig. 1D). Positron emission tomography confirmed a hypermetabolic mass in the topography of the pancreas (probable primary lesion) and extensive metastasis of the lymph nodes and also in the muscle, lung, bone, cutaneous/subcutaneous tissue and brain (Fig. 2). A biopsy of the cervical node was performed and histological analysis revealed an undifferentiated carcinoma but with immunohistochemistry findings suggestive of ACC of the pancreas (Fig. 3). Under palliative care, patient died tree months after the diagnosis.
Our patient was an uncommon presentation of a rare tumor with widespread metastases to various organs including the skin. This case emphasizes that ACC diagnosis although rare and usually associated with advanced ages cannot be ruled out in young patients.
References
1. Klimsatra D, Heffess C, Oertel J, Rosai J. Acinar cell carcinoma of the pancreas. A clinicopathologic study of 28 cases. Am J Surg Pathol. 1992;16:815-37. [ Links ]
2. Toll A, Hruban R, Ali S. Acinar cell carcinoma of the pancreas: clinical and cytomorphologic characteristics. Korean J Pathol. 2013;47:93-9. [ Links ]
3. Ikezoe M, Nishihara T, Yanagawa K, Kohro T, Yamai T, Ikezoe S, et al. A case of pancreatic acinar cell carcinoma metastatic to skin. Rare Tumors. 2010;2:176-8. [ Links ]
4. Lowery M, Klimstra D, Shia J, Yu K, Allen P, Brennan M, et al. Acinar cell carcinoma of the pancreas: new genetic and treatment insights into a rare malignancy. Oncologist. 2011;16:1714-20. [ Links ]
5. La Rosa S, Sessa F, Capella C. Acinar cell carcinoma of the pancreas: overview of clinicopathologic features and insights into the molecular pathology. Front Med. 2015;2:1-13. [ Links ]
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflicts of interest
The authors have no conflicts of interest to declare.
* Corresponding author.
E-mail address: silviagiestas@gmail.com (S. Giestas).
Received 9 November, 2015; accepted 2 December 2015

