










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.23 no.3 Lisboa jun. 2016
https://doi.org/10.1016/j.jpge.2015.11.004
REVIEW ARTICLE
Anti-TNF Withdrawal in Inflammatory Bowel Disease
Discontinuação dos Anti-TNF na Doença Inflamatória Intestinal
Joana Torresa,b,*, Marília Cravoa, Jean-Frédéric Colombelb
a Surgical Department, Gastroenterology Division, Hospital Beatriz Ângelo, Loures, Portugal
b The Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, USA
* Corresponding author.
Abstract
The introduction of the anti-tumor necrosis factorα agents (anti-TNFα) in clinical practice has greatly advanced the treatment of inflammatory bowel disease. The use of these medications results in durable remission in a subset of patients, preventing surgery and hospitalizations. However, there are some concerns about safety and costs associated with their long-term use. Therefore, anti-TNF withdrawal has emerged as an important consideration in clinical practice. Herein our goal was to discuss the available evidence about anti-TNFα discontinuation in IBD that could inform the clinician on the expected rates of relapse, the potential predictors of relapse, as well the response to re-treatment.
Keywords: Inflammatory Bowel Diseases/drug therapy, Tumor Necrosis Factor-Alpha/antagonists and inhibitors, Tumor Necrosis Factor-Alpha/therapeutic use, Withholding Treatment
Resumo
A introdução dos anti-TNFα na prática clínica produziu um avanço considerável no tratamento da doença inflamatória intestinal. A utilização destes medicamentos resulta numa remissão duradoura num sub-grupo de doentes, evitando cirurgias e hospitalização. No entanto, existem algumas preocupações com a segurança e o custo associados com a sua utilização a longo prazo. Assim, a descontinuação dos anti-TNFα tem emergido como uma questão importante na prática clínica. Pretendemos neste artigo, discutir a evidência disponível sobre interrupção dos anti-TNFα na doença inflamatória intestinal, proporcionando ao clínico informação actualizada sobre as taxas de recidiva após interrupção do fármaco, potenciais factores predictores de recidiva, assim como a resposta ao re-tratamento.
Palavras-chave: Doença Inflamatória Intestinal/tratamento, Inibidores Factor de Necrose Tumoral Alfa/antagonistas & inibidores, Factor de Necrose Tumoral Alfa/uso terapêutico, Suspensão de Tratamento
1. Introduction
The introduction of anti-TNF has changed the course of inflammatory bowel disease (IBD). These drugs have proven efficacious in healing the mucosa, and in reducing surgical and hospitalizations rates. Their introduction in the clinic led to major shifts in the therapeutic paradigm that evolved from mere symptomatic clinical remission toward sustained and deep remission. In parallel with the evolution of these therapeutic goals, we have also seen a shift in treatment strategies in IBD. Central to these strategies are the early introduction of immunosuppression, the rapid escalation to anti-TNF therapies (accelerated step-up strategy) or the early introduction of combination therapy (top-down strategy), allied with a tight and frequent control of inflammatory activity, and adjustment of therapy based on that assessment (treat-to-target strategy).1,2 As a result of these strategies, there has been an exponential increase in the number of patients that are treated with anti-TNF monotherapy, or more frequently as combination therapy. However, despite their proven efficacy, anti-TNF's high cost and safety issues are among the main concerns claimed against their long-term use that may motivate doctors and patients to discontinue the drugs when sustained and deep remission has been reached. Questions on if, when and in whom we should discontinue anti-TNF are actively debated by the scientific community. Many studies have now reported on the relapse rates following drug de-escalation, in the hope of identifying a subset of patients in whom therapy could be reduced to the minimal effective therapy that could maintain remission. However, so far no definitive evidence or strategy has been defined. Herein, our goal was to review and summarize the available evidence about anti-TNF discontinuation in IBD, in a comprehensive way that could provide information and hopefully guidance in clinical practice.
2. Why is anti-TNF withdrawal considered in clinical practice?
It may seem counterintuitive to stop a therapy once its therapeutic goals have been achieved; both clinicians and patients may be reluctant, fearing relapse and/or loss of efficacy in the event of re-treatment. However, therapeutic de-escalation is considered in clinical practice for several reasons, namely: (1) safety concerns or side-effects, (2) cost/national regulations, and (3) special situations such as pregnancy, travel or patient preference.
2.1. Safety
Overall, if used with the due precautions, anti-TNF agents have a good short and medium-term safety profile. However, we must also recognize that the follow-up time for anti-TNF and combination therapy is still very limited. An example of this can be drawn from thiopurine use in IBD. Although these drugs have been used in IBD for more than 30 years,3 only recently has it been definitely confirmed their association with the development of lymphoproliferative disorders4 and skin cancer.5 The increased risk of infections and/or malignancies is the most important concern associated with long-term anti-TNF therapy in IBD,6 especially when used in combination therapy. Anti-TNF therapies may increase the risk of infections,6 especially fungal and bacterial,7 and marginally increase the risk of melanoma.8 Patients on combination therapy may have an increased risk of developing hepatosplenic T-cell lymphoma, non-Hodgkin's lymphoma,9 and infections.6 Certain populations, such as the elderly or male pediatric patients,10–12 may be at higher risk for specific complications. Furthermore, side effects may require drug discontinuation.
2.2. Cost/national regulations
In parallel with reduced surgery and hospitalization rates in the biological era,13 the recently published COIN study,14 demonstrated that direct healthcare costs in IBD are now led by medications. The goal of this study, performed in the Netherlands, was to provide an updated overview of general costs in IBD the current era of expanding use of biologics. This study showed that anti-TNF use accounted for 64% and 31% of the direct costs in CD and UC respectively.14 Conversely, surgery, hospitalization, and sick leave accounted for only 19%, <1% and 16% of the healthcare costs in CD, and 23%, 1%, and 39% of costs in UC patients respectively.14 Whilst these calculations do not argue against the cost-effectiveness of these therapies (rather it is the other way around), these costs are indeed substantial. In fact, a number of national societies and expert panels have recommended stopping anti-TNF after one or two year(s) of therapy, provided that clinical remission has been achieved.15–17
2.3. Special situations (pregnancy, traveling, patient preference, insurance policies)
An increasing number of female IBD patients conceive whilst under treatment with anti-TNF. Infliximab (IFX) and adalimumab (ADA) cross the placenta and serum drug levels in the baby may exceed those of the mother.18,19 Therefore discontinuation by the end of the second trimester is generally recommended in pregnant patients in remission.20 Other special situation refers to patients traveling for long periods in areas of the world where access to medications or medical facilities is limited, or where serious infections such as tuberculosis are endemic. The decision to continue anti-TNF in such special situations needs to be carefully balanced against the risk of relapse, taking into account patient's expectations.
3. What are the relapse rates after stopping?
Clinicians and patients are often faced with the question on whether it is possible to stop anti-TNF therapy given that disease remission has been conquered. However, despite all the studies that have now addressed this issue in IBD, no conclusive strategy has yet emerged.21 This may be due to large heterogeneity across different studies precluding firm conclusions on the ideal clinical scenario when the drug could be stopped. Furthermore, and most importantly, it is difficult to draw firm conclusions about the effect of anti-TNF withdrawal due to the lack of control data.
3.1. Anti-TNF discontinuation in Crohn's disease
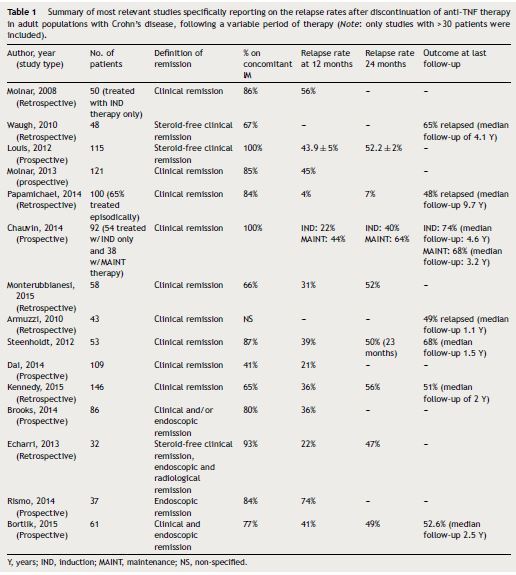
Many studies have now looked into anti-TNF withdrawal in Crohn's disease (see Table 1 for a summary of most relevant studies).22–33 The STORI trial (Infliximab diSconTinuation in Crohn's disease patients in stable Remission on combined therapy with Immunosuppressors) was the pivotal study boosting clinical research in this topic, being thereafter followed by many studies. This was a multicenter study led by the GETAID, and it was the first prospective study specifically designed to assess the risk of relapse, and to identify predictors of relapse following anti-TNF maintenance therapy withdrawal.34 Patients entering the trial had to be in steroid-free remission for a minimum of 6 months, while on at least 1 year of scheduled IFX combined with a stable dose of immunomodulators (azathioprine, 6-mercaptopurine, or MTX). Among the 115 CD patients with luminal disease that were enrolled (perianal CD was excluded), there was a 43.9% (±5.0%) rate of relapse over 1 year and a 52.2% (±5.2%) rate of relapse over 2 years after stopping IFX. Relapse occurred after a median of 16.4 months. Following STORI, many other retrospective and prospective cohorts followed. Importantly, it is worth mentioning, that for most of these studies, patients had the anti-TNF discontinued while they were in clinical remission (with variable definitions of clinical remission and variable duration of remission before drug withdrawal). Interestingly, the relapse rates among those studies are fairly homogenous, ranging from 21 to 56% at 12 months and from 47 to 64% at 24 months respectively24,29,31,34–41 (see Table 1). An exception is the study by Papamichael et al42 that reported lower relapse rates after drug discontinuation; the cumulative probability of maintaining sustained clinical remission after the first, second, third, fourth, and fifth year was 96%, 93%, 88%, 79.9%, and 72.8%, respectively. However, by the end of follow-up (median 10 years), 52% of patients had relapsed. Studies with long follow-up periods have reported high relapse rates ranging from 27%42 to 65%36 at 5 years, and 88% at 10 years.37 The long-term (median 6.9 years) follow-up of the STORI trial, recently presented, showed that 25% of patients who discontinued anti-TNF in the original trial eventually developed bowel damage (need for surgical resection, new perianal fistula).43
The results from the STORI trial suggested that patients with deep remission (clinical and endoscopic) had a very low chance for relapse.34 These results were felt to be encouraging, as they suggested that a subset of patients who had reached deep remission could be good candidates for stopping therapy. Therefore, it was anticipated that stopping anti-TNF in patients presenting full endoscopic and biologic remission, could lead to even higher remission rates. However, recent studies that recruited patients in deep remission (clinical and endoscopic remission) have shown somehow similar relapse rates between 22–74% at 12 months,44,45 47–49% at 24 months,44,46 and 50% at 36 months,27 very similar to those when anti-TNF was discontinued while in clinical remission. For example, in a recently published cohort, patients who discontinued the anti-TNF after endoscopic remission (absence of ulcerations) was attained, were prospectively followed.46 The cumulative probability of relapse at 2 years was 49%.46 The authors compared the relapse rates between the subset of patients that besides endoscopic remission also presented biological remission (FC < 150 mg/kg and CRP levels ≤5 mg/L) to those who only presented clinical and endoscopic remission only. The relapse rates at 2 years were 60% and 52% respectively (non-significant). Although these data require further confirmation, in appropriately powered cohorts, they are somehow disappointing, raising the possibility that even after deep remission has been achieved, the disease will eventually resume its trajectory and the inflammatory cascade will relapse, after the drug has been discontinued.
3.2. Anti-TNF discontinuation in ulcerative colitis
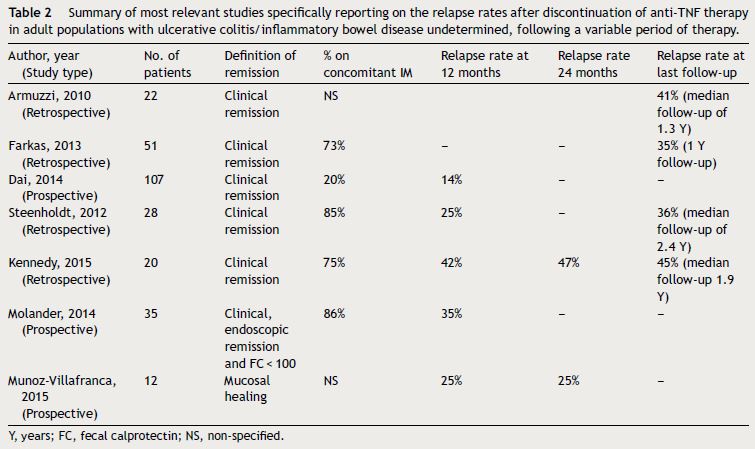
Like in CD, most of the studies that have been made studying anti-TNF discontinuation in UC are very heterogeneous (see Table 2). Nevertheless, the reported relapse rates are somehow similar, perhaps slightly lower than CD. Studies in adult populations have reported relapse rates that range between 14–42% at 12 months, and 25–47% at 24 months24,37,38,41,47–50 (see Table 2). Studies where anti-TNF was discontinued after mucosal healing had been attained, report similar relapse rates at 12 and 24 months of 17–25% and 25–35% respectively47,50. The study with longest follow-up by Steenholdt et al37 reported relapse rates of 60% at 4.5 years.37
4. Can we predict relapse after anti-TNF discontinuation?
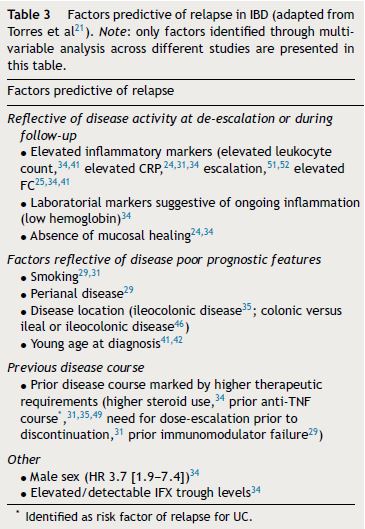
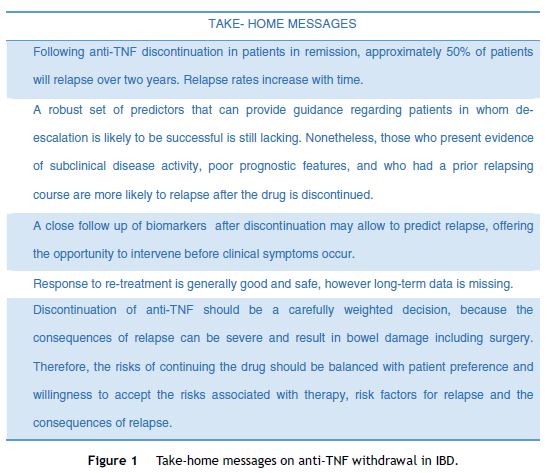
Since anti-TNF discontinuation is associated with high relapse rates, it is crucial to be able to identify risk factors for recurrence (Table 3) that could inform on the risk/benefit of withdrawing. However, it is important to recognize that most studies on anti-TNF discontinuation were not adequately powered for determining risk factors for recurrence, and therefore clinicians should be cautious on relying exclusively in these factors for making their decision. Stopping anti-TNF (or any other therapy) should instead be a personalized and individualized decision, that should take into account the presence of risk factors for relapse, patient phenotype, patient preference, patient specific risk factors for side-effects, weighing them against the consequences of relapse in the individual patient21 (Fig. 1).
Most studies reporting on predictive factors for relapse were made on Crohn's disease, and less evidence is available in UC. Generally speaking, risk factors for disease recurrence can be grouped into four categories: (1) factors indicating (sub-clinical) active disease, (2) prognostic factors for poor disease course, (3) prior disease course, and (4) other mixed factors (Table 3).21 Since many studies have included patients that were discontinued while on clinical remission, it comes as no surprise that evidence of active but sub-clinical disease (reflected as elevated inflammatory markers [elevated C-reactive protein – CRP, elevated fecal calprotectin – FC, high leukocyte count, etc.], presence of ulcers on endoscopy or bowel wall thickening on MRI), is consistently identified across studies as predictive for relapse.25,34,41,51,52 Therefore, it is legitimate to state that clinical remission per se is not enough of an argument to stop a drug in IBD. Physicians that are considering on discontinuing anti-TNF should always make a full work-up on their patients, including an endoscopic and/or radiological examination before making that decision. Those patients presenting risk factors that have been associated with a poor disease course, such as young age at diagnosis, complicated phenotype, and disease located in the terminal ileum, more extensive disease, smoking, etc, will be more likely to relapse when the drug is discontinued.29,31,35,42,46 Likewise, prior disease course may be informative on relapse. Patients that had in the past a disease that was more difficult to control, or that had higher therapeutic requirements, need for dose-escalation to achieve and/or maintain remission, etc. may reflect a group with more severe disease, and therefore may be at higher risk for relapsing.31,35,49 The type and duration of therapy and of disease may impact recurrence rates, as shorter anti-TNF duration and longer disease duration before anti-TNF have been identified as predictors for relapse in some studies, whereas a shorter interval between disease diagnosis and starting anti-TNF, and maintaining the treatment with an immunomodulator were associated with remission.42,53Other factors have also been identified. A very interesting finding, that has now been replicated in some studies is that those patients who have lower or undetectable trough levels before drug discontinuation have a lower chance of relapse.34,42,54 In a retrospective cohort, patients with IBD who discontinued anti-TNF while in remission (endoscopic or radiological remission documented in 95% of patients) had their trough levels measured before discontinuation. The odds for clinical relapse by 12 months of follow-up was 30 times higher (95% CI: 5.8–153) for those who presented detectable trough levels as compared to those who did not.54 This finding had also been observed in the STORI trial, where presenting infliximab trough level >2 mg/L (HR 2.5 [1.1–5.4)] was predictive for relapse.34 This may seem counterintuitive, as absence or low trough levels have been associated with worse outcomes,55 boosting the use of therapeutic drug monitoring in the clinic for therapy optimization. However, for the subset of patients in long-lasting remission, low/absent trough levels may indicate that remission is no longer driven by the anti-TNF, and therefore that these patients no longer need the drug to maintain the remission state. On the same topic, it is very interesting to note that for patients stopping the immunomodulator and maintaining the anti-TNF, the presence of good anti-TNF trough levels is protective from relapse.56 Therefore, therapeutic drug monitoring may in the future be a powerful tool to select patients for anti-TNF withdrawal.
One very important message that arose from a sub-study of the STORI trial and was later confirmed in another cohort is that clinical relapse is preceded by elevation of inflammatory markers.51,52 In STORI's51 prospective follow-up, 113 patients had bimonthly measurements of CRP and FC; those who later relapsed, presented a marked rise in these inflammatory markers occurring 4 months before relapse. The median value for FC and CRP before relapse was 534 μg/g and 8 mg/L for relapsers and 66.9 μg/g and 3.7 mg/L for non-relapsers, respectively.51 These findings have been confirmed in another cohort52, and indicate that in patients stopping anti-TNF, a close follow-up with regular laboratorial assessment, may allow to diagnose relapse even before symptoms occur, offering the possibility for early intervention.
5. Can we re-treat after we stop?
A reassuring message arising from some studies is that if relapse occurs, re-treatment may be successfully and safely re-instituted. A significant proportion of the patients that relapsed across studies were re-treated. Most studies only provided the rates of clinical remission/response after re-treatment with no further details.30,31,36,41,44,57,58 Also, most studies have only reported short-term results, frequently for the induction therapy phase. Apart from some exceptions,31,36 the short-term remission/response rates to re-treatment (often using the same biologic agent) were generally very good, ranging from 78% to 100% in CD and 54–100% in UC.38,41,47,49 Studies reporting longer follow-up of at least one year reported clinical remission rates between 80 and 92% at one year35,50,53 for CD.
6. Unanswered questions and perspectives
There are many unanswered questions that are worth mentioning. The first and most important is that so far there is no controlled study that can really answer the question on whether maintaining the anti-TNF is superior to maintain remission as opposed to discontinuing the drug. In second place, there is a lack of studies appropriately powered, looking into the possibility of reducing the dose of the anti-TNF once remission has been attained, although this could be an interesting approach for reducing costs and perhaps adverse effects.59 In rheumatoid arthritis for example, a meta-analysis on de-escalation of anti-TNF in randomized and controlled clinical trials in patients with rheumatoid arthritis (RA), showed that while reducing the drug dose (etarnecept data only) was not associated with worse outcomes, stopping the drug (etarnecept or adalimumab data) led to higher rates of clinical activity and worse radiological and functional outcomes.60 In IBD, three small studies have explored this possibility with apparently good results.22,25,61 Third, stopping the anti-TNF when the drug has been used as monotherapy has also not been adequately studied in IBD, which reflects the clinical practice where these agents are often used in combination with an immunomodulator agent. Fourth, it is also very interesting to acknowledge that are no studies specifically studying anti-TNF discontinuation in early disease. Evidence from rheumatology suggests that studies focusing on drug withdrawal after early drug treatment with anti-TNF may be more fruitful.62 Finally, the topic of personalizing discontinuation, taking into account the specific patient risk for complications development needs to be further explored.10
Clearly, the topic of drug de-escalation is a very important one in IBD and warrants further research. A large European Union funded trial (Biocycle project) will soon start and likely solve many of the answered questions.63 This large multicenter project will for the first time study different discontinuation strategies in a controlled fashion. Patients with CD in sustained steroid-free remission on combination therapy will be randomized to continuing therapy, discontinuing the anti-TNF or the immunomodulator. The results of this trial will be then used to inform the concept of treatment cycles in IBD, characterized by periods where both anti-TNF and immunomodulators are administered alternating with periods where either of the drug is withdrawn after remission has been reached. Hopefully this large trial will inform us on how to make the best use of the current therapeutic strategies we currently have, shedding some light into this important question in clinical practice.
References
1. Ordas I, Feagan BG, Sandborn WJ. Early use of immunosuppressives or TNF antagonists for the treatment of Crohn's disease: time for a change. Gut. 2011;60:1754-63. [ Links ]
2. Sandborn WJ, Hanauer S, Van Assche G, Panes J, Wilson S, Petersson J, et al. Treating beyond symptoms with a view to improving patient outcomes in inflammatory bowel diseases. J Crohns Colitis. 2014;8:927-35. [ Links ]
3. Present DH, Korelitz BI, Wisch N, Glass JL, Sachar DB, Pasternack BS. Treatment of Crohn's disease with 6-mercaptopurine. A long-term, randomized, double-blind study. N Engl J Med. 1980;302:981-7. [ Links ]
4. Beaugerie L, Brousse N, Bouvier AM, Colombel JF, Lemann M, Cosnes J, et al. Lymphoproliferative disorders in patients receiving thiopurines for inflammatory bowel disease: a prospective observational cohort study. Lancet. 2009;374:1617-25. [ Links ]
5. Peyrin-Biroulet L, Khosrotehrani K, Carrat F, Bouvier AM, Chevaux JB, Simon T, et al. Increased risk for nonmelanoma skin cancers in patients who receive thiopurines for inflammatory bowel disease. Gastroenterology. 2011;141:1621-8. [ Links ]
6. Lichtenstein GR, Feagan BG, Cohen RD, Salzberg BA, Diamond RH, Price S, et al. Serious infection and mortality in patients with Crohn's disease: more than 5 years of follow-up in the TREAT registry. Am J Gastroenterol. 2012;107:1409-22. [ Links ]
7. Colombel JF, Loftus EV, Tremaine WJ, Egan LJ, Harmsen WS, Schleck CD, et al. The safety profile of infliximab in patients with Crohn's disease: the Mayo clinic experience in 500 patients. Gastroenterology. 2004;126:19-31. [ Links ]
8. Long MD, Martin CF, Pipkin CA, Herfarth HH, Sandler RS, Kappelman MD. Risk of melanoma and nonmelanoma skin cancer among patients with inflammatory bowel disease. Gastroenterology. 2012;143:390-9. [ Links ]
9. Siegel CA, Marden SM, Persing SM, Larson RJ, Sands BE. Risk of lymphoma associated with combination anti-tumor necrosis factor and immunomodulator therapy for the treatment of Crohn's disease: a meta-analysis. Clin Gastroenterol Hepatol. 2009;7:874-81. [ Links ]
10. Kirchgesner J, Carrat F, Cosnes J, Schwarzinger M, Beaugerie L. Sa1118 withdrawing or continuing maintenance treatment with thiopurines in patients with Crohn's disease in sustained clinical remission: a lifetime risk-benefit analysis. Gastroenterology. 2015;148:S231. [ Links ]
11. Cottone M, Kohn A, Daperno M, Armuzzi A, Guidi L, D’Inca R, et al. Advanced age is an independent risk factor for severe infections and mortality in patients given anti-tumor necrosis factor therapy for inflammatory bowel disease. Clin Gastroenterol Hepatol. 2011;9:30-5.
12. Beaugerie L. Lymphoma: the bete noire of the long-term use of thiopurines in adult and elderly patients with inflammatory bowel disease. Gastroenterology. 2013;145:927-30. [ Links ]
13. Costa J, Magro F, Caldeira D, Alarcao J, Sousa R, Vaz-Carneiro A. Infliximab reduces hospitalizations and surgery interventions in patients with inflammatory bowel disease: a systematic review and meta-analysis. Inflamm Bowel Dis. 2013;19:2098-110. [ Links ]
14. van der Valk ME, Mangen MJ, Leenders M, Dijkstra G, van Bodegraven AA, Fidder HH, et al. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFalpha therapy: results from the COIN study. Gut. 2014;63:72-9. [ Links ]
15. Mowat C, Cole A, Windsor A, Ahmad T, Arnott I, Driscoll R, et al. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2011;60:571-607. [ Links ]
16. Pittet V, Froehlich F, Maillard MH, Mottet C, Gonvers JJ, Felley C, et al. When do we dare to stop biological or immunomodulatory therapy for Crohn's disease? Results of a multidisciplinary European expert panel. J Crohns Colitis. 2013;7:820-6. [ Links ]
17. D’Haens GR, Panaccione R, Higgins PD, Vermeire S, Gassull M, Chowers Y, et al. The London Position Statement of the World Congress of Gastroenterology on Biological Therapy for IBD with the European Crohn's and Colitis Organization: when to start, when to stop, which drug to choose, and how to predict response?. Am J Gastroenterol. 2011;106:199-212.
18. Zelinkova Z, de Haar C, de Ridder L, Pierik MJ, Kuipers EJ, Peppelenbosch MP, et al. High intra-uterine exposure to infliximab following maternal anti-TNF treatment during pregnancy. Aliment Pharmacol Ther. 2011;33:1053-8. [ Links ]
19. Zelinkova Z, van der Ent C, Bruin KF, van Baalen O, Vermeulen HG, Smalbraak HJT, et al. Effects of discontinuing anti-tumor necrosis factor therapy during pregnancy on the course of inflammatory bowel disease and neonatal exposure. Clin Gastroenterol Hepatol. 2013;11:318-21. [ Links ]
20. van der Woude CJ, Ardizzone S, Bengtson MB, Fiorino G, Fraser G, Katsanos K, et al. The second European evidenced-based consensus on reproduction and pregnancy in inflammatory bowel disease. J Crohns Colitis. 2015;9:107-24. [ Links ]
21. Torres J, Boyapati RK, Kennedy N, Louis E, Colombel JF, Satsangi J. Systematic review of effects of withdrawal of immunomodulators or biologic agents from patients with inflammatory bowel disease. Gastroenterology. 2015;149:1716-30. [ Links ]
22. Sorrentino D, Paviotti A, Terrosu G, Avellini C, Geraci M, Zarifi D. Low-dose maintenance therapy with infliximab prevents postsurgical recurrence of Crohn's disease. Clin Gastroenterol Hepatol. 2010;8:591-9. [ Links ]
23. Ciria V, Silva P, Leo E, Trigo C, De La Cruz MD, Herrera JM, et al. Factors influencing recurrence following suspension of biological treatment. Importance of mucosal healing. J Crohns Colitis. 2014;8:S270. [ Links ]
24. Armuzzi A, Marzo M, Felice C, De Vincentis F, Andrisani G, Mocci G, et al. Long-term scheduled therapy with infliximab in inflammatory bowel disease: a single-centre observational study. Gastroenterology. 2010;1:S691-S2. [ Links ]
25. Mantzaris GJ, Karatzas P, Kyriakos N, Archavlis EJ, Papamichael K, Tzannetakou X, et al. Can we increase the dose interval of infliximab to 10 weeks without risking loss of response in patients with crohn's disease? Prospective, single-center pilot study based on successive measurements of fecal calprotectin. Gastroenterology. 2014;1:S-248. [ Links ]
26. Lane C, Ramakrishnan S, Dougherty J. Outcomes of the use of infliximab and adalimumab in patients with Crohn's disease at a district general hospital. Gut. 2014;63:A70. [ Links ]
27. Iimuro M, Nakamura S, Sato T, Ogawa T, Kawai M, Nogami K, et al. Long term outcome of top-down therapy in Crohn's disease: a single-center experience. Inflamm Bowel Dis. 2011;17:S49-50. [ Links ]
28. Domenech E, Hinojosa J, Nos P, Garcia-Planella E, Cabre E, Bernal I, et al. Clinical evolution of luminal and perianal Crohn's disease after inducing remission with infliximab: how long should patients be treated?. Aliment Pharmacol Ther. 2005;22:1107-13. [ Links ]
29. Chauvin A, Le Thuaut A, Belhassan M, Le Baleur Y, Mesli F, Bastuji-Garin S, et al. Infliximab as a bridge to remission maintained by antimetabolite therapy in Crohn's disease: a retrospective study. Dig Liver Dis. 2014;46:695-700. [ Links ]
30. Wynands J, Belbouab R, Candon S, Talbotec C, Mougenot JF, Chatenoud L, et al. 12-Month follow-up after successful infliximab therapy in pediatric crohn disease. J Pediatr Gastroenterol Nutr. 2008;46:293-8. [ Links ]
31. Molnar T, Lakatos PL, Farkas K, Nagy F, Szepes Z, Miheller P, et al. Predictors of relapse in patients with Crohn's disease in remission after 1 year of biological therapy. Aliment Pharmacol Ther. 2013;37:225-33. [ Links ]
32. Crombe V, Salleron J, Savoye G, Dupas JL, Vernier-Massouille G, Lerebours E, et al. Long-term outcome of treatment with infliximab in pediatric-onset Crohn's disease: a population-based study. Inflamm Bowel Dis. 2011;17:2144-52. [ Links ]
33. Nuti F, Conte F, Cavallari N, Civitelli F, Aloi M, Alessandri C, et al. Long term efficacy of infliximab in inflammatory bowel disease at a single tertiary center. Dig Liver Dis. 2010;42:S326-7. [ Links ]
34. Louis E, Mary JY, Verniermassouille G, Grimaud JC, Bouhnik Y, Laharie D, et al. Maintenance of remission among patients with Crohn's disease on antimetabolite therapy after infliximab therapy is stopped. Gastroenterology. 2012;142:63-70. [ Links ]
35. Brooks AJ, Sebastian S, Cross SS, Robinson K, Warren L, Wright A, et al. Outcome of elective withdrawal of anti-tumour necrosis factor-alpha therapy in patients with Crohn's disease in established remission. J Crohns Colitis. 2015, http://dx.doi.org/10.1016/j.crohns.2014.09.007 (in press). [ Links ]
36. Monterubbianesi R, Papi C, Kohn A. P529. Maintenance of clinical remission in Crohn's disease patients after discontinuation of antiTNF agents: results from a single centre cohort. J Crohns Colitis. 2015;9:S345. [ Links ]
37. Steenholdt C, Molazahi A, Ainsworth MA, Brynskov J, Thomsen OO, Seidelin JB. Outcome after discontinuation of infliximab in patients with inflammatory bowel disease in clinical remission: an observational Danish single center study. Scand J Gastroenterol. 2012;47:518-27. [ Links ]
38. Dai C, Liu WX, Jiang M, Sun MJ. Mucosal healing did not predict sustained clinical remission in patients with IBD after discontinuation of one-year infliximab therapy. PLOS ONE. 2014;9. [ Links ]
39. Waugh AW, Wong K, Fedorak RN. Maintenance of clinical benefit in Crohn's disease patients after discontinuation of infliximab: long term follow-up of a single center cohort. Gastroenterology. 2010;1:S685. [ Links ]
40. Molnar T, Farkas K, Miheller P, Nyari T, Szepes Z, Herszenyi L, et al. Is the efficacy of successful infliximab induction therapy maintained for one year lasting without retreatment in different behavior types of Crohn's disease?. J Crohns Colitis. 2008;2:322-6. [ Links ]
41. Kennedy A, Warner B, Johnston E, Flanders L, Hendy P, Ding N, et al. DOP035. Anti-TNF withdrawal in IBD: relapse and recapture rates and predictive factors from 160 patients in a pan-UK study. J Crohns Colitis. 2015;9:S41-2. [ Links ]
42. Papamichael K, Vande N, Gils A, Tops S, Hauenstein S, Singh S, et al. Long-term outcome of patients with Crohn's disease who discontinued infliximab therapy upon clinical remission. Clin Gastroenterol Hepatol. 2015;13:1103-10. [ Links ]
43. Reenaers C, Nachury M, Bouhnik Y, Laharie D, Allez M, Dupas JL, et al. Long-term outcome after infliximab withdrawal for sustained remission in Crohn's disease. United Eur Gastroenterol J. 2015;3:A31. [ Links ]
44. Echarri A, Ollero V, Rodriguez JA, Gallego JC, Castro J. Predictors of relapse after discontinuing anti-TNF therapy in Crohn's disease patients on deep remission. J Crohns Colitis. 2013;7:S171. [ Links ]
45. Rismo R, Olsen T, Cui G, Paulssen EJ, Christiansen I, Johnsen K, et al. Normalization of mucosal cytokine gene expression levels predicts long-term remission after discontinuation of anti-TNF therapy in Crohn's disease. Scand J Gastroenterol. 2013;48:311-9. [ Links ]
46. Bortlik M, Duricova D, Machkova N, Hruba V, Lukas M, Mitrova K, et al. Discontinuation of anti-tumor necrosis factor therapy in inflammatory bowel disease patients: a prospective observation. Scand J Gastroenterol. 2015;1-7. [ Links ]
47. Munoz C, Bravo MT, Ortiz J, Arreba P, Garcia I, Heras J, et al. Mucosal healing in patients with ulcerative colitis treated with infliximab. What happens after treatment is discontinued?. J Crohns Colitis. 2014;8:S234-5. [ Links ]
48. Anderson GJ, Cipolla CM, Kennedy RT. Western blotting using capillary electrophoresis. Anal Chem. 2011;83:1350-5. [ Links ]
49. Farkas K, Lakatos PL, Nagy F, Szepes Z, Miheller P, Papp M, et al. Predictors of relapse in patients with ulcerative colitis in remission after one-year of infliximab therapy. Scand J Gastroenterol. 2013;48:1394-8. [ Links ]
50. Molander P, Farkkila M, Salminen K, Kemppainen H, Blomster T, Koskela R, et al. Outcome after discontinuation of TNFalpha-blocking therapy in patients with inflammatory bowel disease in deep remission. Inflamm Bowel Dis. 2014;20:1021-8. [ Links ]
51. De Suray N, Salleron J, Vernier-Massouille G, Grimaud JC, Bouhnik Y, Laharie D, et al. Close monitoring of CRP and fecal calprotectin is able to predict clinical relapse in patients with crohn's disease in remission after infliximab withdrawal. A sub-analysis of the stori study. Gastroenterology. 2012;1:S149. [ Links ]
52. Molander P, Farkkila M, Ristimaki A, Salminen K, Kemppainen H, Blomster T, et al. Does fecal calprotectin predict short-term relapse after stopping TNFalpha-blocking agents in inflammatory bowel disease patients in deep remission?. J Crohns Colitis. 2015;9:33-40. [ Links ]
53. Casanova MJ, Chaparro M, Garcia-Sanchez V, Nantes O, Jáuregui-Amezaga A, Rojas-Feria M, et al. P500. Evolution after anti-TNF drug discontinuation in patients with inflammatory bowel disease (IBD): a multicenter long-term follow-up study. J Crohns Colitis. 2015;9:S329. [ Links ]
54. Ben-Horin S, Chowers Y, Ungar B, Kopylov U, Loebstein R, Weiss B, et al. Undetectable anti-TNF drug levels in patients with long-term remission predict successful drug withdrawal. Aliment Pharmacol Ther. 2015;42:356-64. [ Links ]
55. Ben-Horin S, Chowers Y. Tailoring anti-TNF therapy in IBD: drug levels and disease activity. Nat Rev Gastroenterol Hepatol. 2014;11:243-55. [ Links ]
56. Drobne D, Bossuyt P, Breynaert C, Cattaert T, Vande N, Compernolle G, et al. Withdrawal of immunomodulators after co-treatment does not reduce trough level of infliximab in patients with Crohn's disease. Clin Gastroenterol Hepatol. 2015;13:514-21. [ Links ]
57. Luppino I, Spagnuolo R, Marasco R, Cosco C, Ruggiero G, Cosco V, et al. Withdrawal of infliximab (IFX) after achieving remission: outcome in a cohort of inflammatory bowel disease (IBD) patients. Dig Liver Dis. 2013;45:S100-1. [ Links ]
58. Zucchi E, Fabbro M, Pinese E, Marino M, Panos J, Bulajic M, et al. Outcome of infliximab discontinuation in IBD patients and therapy rechallenging in relapsers: single centre preliminary data. Dig Liver Dis. 2014;46:S31. [ Links ]
59. Westhovens R, Yocum D, Han J, Berman A, Strusberg I, Geusens P, et al. The safety of infliximab, combined with background treatments, among patients with rheumatoid arthritis and various comorbidities: a large, randomized, placebo-controlled trial. Arthritis Rheum. 2006;54:1075-86. [ Links ]
60. van Herwaarden N, den Broeder AA, Jacobs W, van der Maas A, Bijlsma JW, van Vollenhoven RF, et al. Down-titration and discontinuation strategies of tumor necrosis factor-blocking agents for rheumatoid arthritis in patients with low disease activity. Cochrane Database Syst Rev. 2014;9:CD010455. [ Links ]
61. Roblin X, Paul S. Letter: stool adalimumab detection in ulcerative colitis and Crohn's disease. Aliment Pharmacol Ther. 2015;42:240. [ Links ]
62. Smolen JS, Emery P, Fleischmann R, van Vollenhoven RF, Pavelka K, Durez P, et al. Adjustment of therapy in rheumatoid arthritis on the basis of achievement of stable low disease activity with adalimumab plus methotrexate or methotrexate alone: the randomised controlled OPTIMA trial. Lancet. 2014;383:321-32. [ Links ]
63. Biocycle. Biological therapy cycles (accessed October 2015). Available at: http://biocycle-project.eu/. [ Links ]
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data.The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflict of interest
The authors have no conflicts of interest to declare.
Author's contribution
JT has made substantial contributions to conception and design, acquisition and analysis and interpretation of data and has drafted the article. MC and JFC have revised the manuscript critically for important intellectual content. All authors have provided final approval of the version to be published.
* Corresponding author.
E-mail address: joana.torres@hbeatrizangelo.pt, joana.torres@mssm.edu (J. Torres).
Received 4 November 2015; accepted 30 November 2015


{kind=link}
{kind=link}
{kind=link}
{kind=link}