










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.22 no.3 Lisboa jun. 2015
https://doi.org/10.1016/j.jpge.2014.12.002
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Meckels Diverticulum: A Rare Cause of Overt Obscure Gastrointestinal Bleeding in an Adult Male
Divertículo de Meckel: Causa Rara de Hemorragia Digestiva Obscura Manifesta num Homem Adulto
Carlos Fernandes∗, Rolando Pinho, João Carvalho
Gastroenterology Department, Centro Hospitalar Vila Nova de Gaia/Espinho, Vila Nova Gaia, Portugal
* Corresponding author.
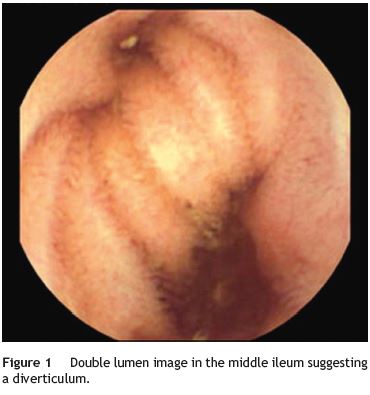
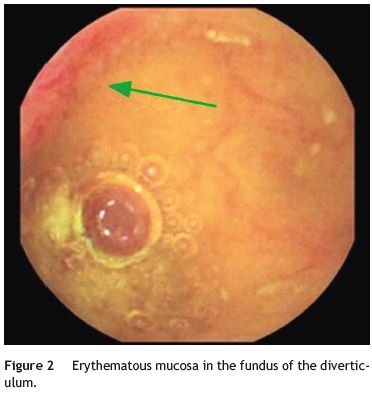
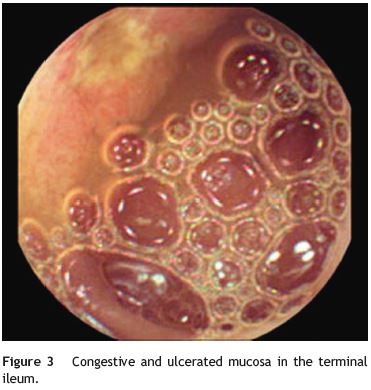
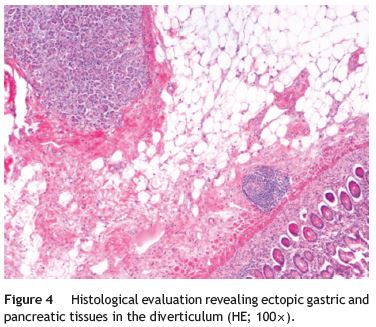
A 64-year-old male, with history of arterial hypertension and colonic polyps, recurred to the emergency department with recurrent hematochezia in the last 6 h. He denied abdominal pain, fever or other symptoms. No anemia or hemodynamic instability was present. Physical examination confirmed fresh blood and clots in the rectal ampulla. An urgent colonoscopy revealed fresh blood and clots in the terminal ileum and through the colon. Subsequently an urgent upper gastrointestinal endoscopy was performed with no relevant findings. Hence, in the same day, an urgent capsule enteroscopy was performed. In the middle ileum, a large diverticulum (Fig. 1) with erythematous mucosa in the fundus (Fig. 2) and a linear ulcer in the neck was found. Congestive mucosa and several deep ulcers with no active bleeding were apparent adjacent and downstream from the diverticulum (Fig. 3). These features highly suggested a Meckels diverticulum with ectopic gastric mucosa. After a multidisciplinary discussion, a laparoscopic diverticulectomy was performed. Histological evaluation confirmed a Meckels diverticulum with gastric and pancreatic tissues (Fig. 4). The patient was discharged 5 days later. No changes in the terminal ileum were apparent in a colonoscopy performed because of a post-polipectomy surveillance 4 months later.
Meckels diverticulum is the most common congenital anomaly in the GI tract. It results from a persistent remnant of the omphalomesenteric duct and it is usually located in the antimesenteric side of the middle/distal ileum. It has an estimated prevalence of 2% in general population and it is twice more prevalent in males.1 Histological evaluation reveals ectopic tissue in 10-20% of the cases, mostly gastric mucosa.2 Nevertheless, the embryological origin of this later phenomenon is not well known. Meckels diverticulum is often asymptomatic and only 2-4% will develop a related complication during the life course. Gastrointestinal bleeding is the most common manifestation in adults.3 Ectopic gastric tissue leads to acid secretion and consequently to mucosal ulceration downstream from the diverticulum. Hence, an obscure or overt GI bleeding may rarely occur. A nuclear medicine study using 99m technetium pertechnetate - Meckels scan - has been used for diagnosis. Nevertheless it is only able to diagnose Meckels diverticulum with ectopic gastric mucosa, which is only present in 20% of the cases. More recently, capsule enteroscopy and device-assisted enteroscopy have also been used for diagnosis.4 A surgical approach is recommended in symptomatic Meckels diverticulum.5 A simple diverticulectomy or segmental bowel resection with a primary anastomosis are possible. The management of incidental and asymptomatic Meckels diverticulum is still controversial.
References
1. Brown CK, Olshaker JS. Meckels diverticulum. Am J Emerg Med. 1988;6:157-64. [ Links ]
2. Menezes M, Tareen F, Saeed A, Khan N, Puri P. Symptomatic Meckels diverticulum in children: a 16-year review. Pediatr Surg Int. 2008;24:575-7. [ Links ]
3. Freeny PC, Walker JH. Inverted diverticula of the gastrointestinal tract. Gastrointest Radiol. 1979;4:57-9. [ Links ]
4. Zheng CF, Huang Y, Tang ZF, Chen L, Leung YK. Double-balloon enteroscopy for the diagnosis of Meckels diverticulum in pediatric patients with obscure GI bleeding. Gastrointest Endosc. 2014;79:354-8. [ Links ]
5. Papparella A, Nino F, Noviello C, Marte A, Parmeggiani P, Martino A, et al. Laparoscopic approach to Meckels diverticulum. World J Gastroenterol. 2014;20:8173-8. [ Links ]
* Corresponding author.
E-mail address: carlosdpfernandes@gmail.com (C. Fernandes).
Ethical responsibilities
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflict of interest
Nothing to declare.
Received 21 November 2014; accepted 9 December 2014

