










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
Print version ISSN 2341-4545
GE Port J Gastroenterol vol.22 no.2 Lisboa Apr. 2015
https://doi.org/10.1016/j.jpge.2014.10.004
ENDOSCOPIC SNAPSHOT
A New Method for Distal Repositioning of a Misplaced Esophageal Stent
Rui Silva
Gastroenterology Department, Instituto Português de Oncologia do Porto Francisco Gentil, Porto, Portugal
* Corresponding author.
Several techniques for managing migrated and misplaced self-expanding esophageal metal stents have been described.1-5 However, most of these techniques apply only when there is distal stent dislodgment. When there is proximal stent migration or misplacement, and unless there is a lasso at the distal flange, trying to reposition the stent distally through the stenotic tumor can be challenging. Although it may be tried by grasping distal tines with forceps or inflating a dilating balloon within the stent and applying gentle pressure, it seldom results. We herein report an endoscopic approach for an easy and safe reposition of proximal dislodged esophageal metal stents that, as far as we are aware, was never described before.
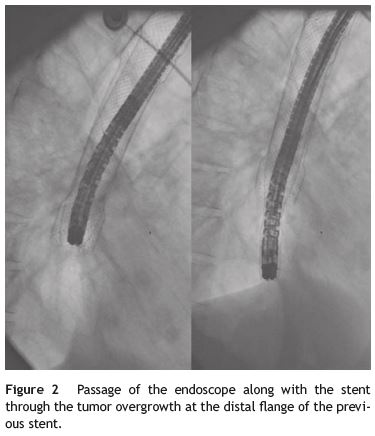
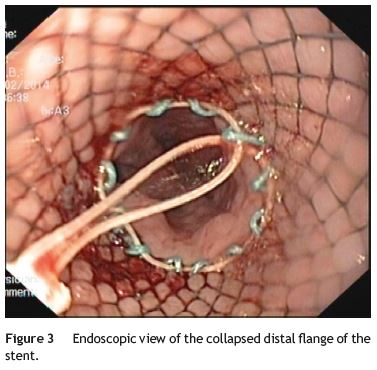
The stent is removed by grasping the lasso on the proximal end of the stent with an alligator jaw grasping forceps. Outside the patient, the lasso is released and the stent s turned upside down. The endoscope is then introduced through the distal end of the stent until the proximal end, where the lasso is re-grasped by the forceps and pulled back, allowing the upper flange of the stent to collapse over the tip of the endoscope (Fig. 1). The body of the stent is generously lubricated with aqueous jelly and stretched along the endoscope. The patient is reintubated with gently passage of the endoscope and the stent through the pharynx and cricopharyngeus into the upper esophagus. Under fluoroscopic guidance and direct visualization, the endoscope is than advanced through the tumor (Figs. 2 and 3). If significant narrowing prevents the safe passage of the endoscope along with the stent, gentle esophageal dilation to 11-13mm is performed. The lasso is then released and the stent deployed according with the marks previously placed.

We have performed this technique in 3 patients during the last four years, with successful stent repositioning and no complications.
References
1. Seitz U, Thonke F, Bohnacker S, Brand B, Jaeckle S, Soehendra N. Endoscopic extraction of a covered esophageal Z-stent with the aid of Endoloops. Endoscopy. 1998;30:S91-2. [ Links ]
2. Raijman I, Marcon NE, Kandel G, Haber GB, Kortan P. Repositioning of an esophageal stent after migration using a snare. Gastrointest Endosc. 1994;40:652. [ Links ]
3. Farkas PS, Farkas JD, Koenigs KP. An easier method to remove migrated esophageal Z-stents. Gastrointest Endosc. 1999;50:277-9. [ Links ]
4. May A, Gossner L, Feess G, Bauer R, Ell C. Extraction of migrated self-expanding esophageal metal stents. Gastrointest Endosc. 1999;49:524-6. [ Links ]
5. Martins B, Sorbello MP, Retes F, Kawaguti FS, Lima MS, Hondo FY, et al. Endoscopic removal of migrated esophageal stent - the grasper and pusher method. Endoscopy. 2012;44 Suppl. 2. UCTN:E10. [ Links ]
* Corresponding author
E-mail address: rsgastro@sapo.pt
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflicts of interest
Consultant for Cook Medical and Boston Scientific Corporation.
Received 24 September 2014; accepted 20 October 2014

