










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.22 no.2 Lisboa abr. 2015
https://doi.org/10.1016/j.jpge.2015.01.004
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Pneumoperitoneum after Percutaneous Endoscopic Gastrostomy
Pneumoperitoneu após Gastrostomia Endoscópica percutânea
Sandra Barbeiro∗, Catarina Martins, Cláudia Gonçalves
Gastroenterology Department, Centro Hospitalar de Leiria, Leiria, Portugal
* Corresponding author.
1. Case report
A 68-year-old male was admitted to the Gastroenterology department for elective percutaneous endoscopic gastrostomy (PEG) tube placement. The patient had neurologic dysphagia secondary to amiotrophic lateral sclerosis, recurrent low respiratory tract infections and was receiving nutricional support from a nasogastric tube since the previous four months.
A 20Fr PEG tube ( Covidien®) was placed by pull-onstringtechnique, with the external bumper on the 3.5 cm mark. There were no complications during the procedure or after a 24-hour surveillance period. Enteral feeding with the PEG tube was successfully started. Oral and written educational support was provided to the caregivers.
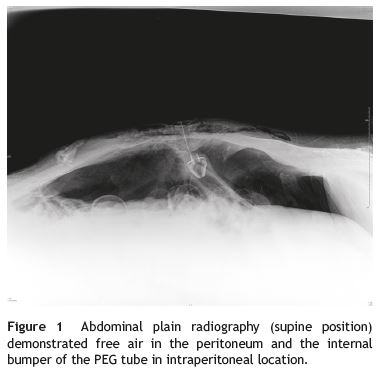
Four days after PEG tube placement, the patient developed abdominal distension and dyspnea. Complications with feeding, hygiene and PEG tube mobilization were denied by the caregivers. Polypnea and subcutaneous emphysema in the upper and lower left quadrants were noticed, as well as abdominal distension and diffuse tenderness with peritoneal signs. Abdominal plain radiography demonstrated pneumoperitoneum and the internal bumper of the PEG tube in intraperitoneal location (Fig. 1). An exploratory laparotomy was undertaken and a perforation site in the gastric greater curvature was identified, although it was covered by epiplon with engaging fibrin. Surgical washing, raphy with epiplonoplasty and an Witzel feeding jejunostomy were done. The patient recovered successfully after surgery.
2. Discussion
PEG tube placement is a safe and effective method allowing the enteric nutritional support when oral ingestion is compromised.1
Pneumoperitoneum complicate s the procedure in 5-16%,3,4 occurring during the tube placement or after early tube mobilization, before fistula path is definitely created (the first 14-20 days).2 The presence of a small amount of air in the peritoneal cavity is a benign finding due to air inflated into the gastric lumen during endoscopy.1 In 85-91% of these cases the course is benign, with spontaneous and quick recovery (mean time to resolution was 2.7 days).1,3 However, pneumoperitoneum can be a sign of a more severe complication, as intestinal perforation. The clinical challenge is the distinction between these two entities.
Thus, the suspicion of pneumoperitoneum requires evaluation and must not always be assumed as benign. The asymptomatic and stable patient should be kept under surveillance and usually no intervention is needed.1,5 However, in the presence of abdominal pain, tenderness, rigidity, progressive distension, fever, hemodynamic instability, leucocytosis or evidence of free fluid in the peritoneal cavity in addition to free air, a surgical attitude must be strongly considered.1,5
In our current case, excessive traction of the tube with release of the internal bumper into the peritoneal cavity and consequent flow of air from the gastric lumen was the probable cause of the pneumoperitoneum. A surgical approach was taken due to the presence peritoneal signs and ventilatory compromise secondary to the severe abdominal distention.
In conclusion, checking for pneumoperitoneum routinely is pointless in the absence of peritoneal signs. Clinical signs of peritonitis are a much more accurate marker of acute complication than the presence of pneumoperitoneum in a postprocedure radiograph.3
References
1. Vijayakrishnan R, Adhikari D, Anand CP. Recurrent tense pneumoperitoneum due to air influx via abdominal wall stoma of a PEG tube. World J Radiol. 2010;2:280-2. [ Links ]
2. Varela SZ, Pareja CF, Docobo DF, García MD, García MJ. Giant pneumoperitoneum secondary to percutaneous endoscopic gastrostomy. Rev Esp Enferm Dig. 2007;99:121-2. [ Links ]
3. Blum CA, Selander C, Ruddy JM, Leon S. The incidence and clinical significance of pneumoperitoneum after percutaneous endoscopic gastrostomy: a review of 722 cases. Am Surg. 2009;75:39-43. [ Links ]
4. Nazarian A, Cross W, Kowdley GC. Pneumoperitoneum after percutaneous endoscopic gastrostomy among adults in the intensive care unit: incidence, predictive factors, and clinical significance. Am Surg. 2012;78:591-4. [ Links ]
5. Milanchi S, Allins A. Early pneumoperitoneum after percutaneous endoscopic gastrostomy in intensive care patients: sign of possible bowel injury. Am J Crit Care. 2007;16:132-6. [ Links ]
* Corresponding author
E-mail address: sandrabarbeiro@gmail.com (S. Barbeiro).
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interest
The authors have no conflicts of interest to declare.
Received 4 November 2014; accepted 12 January 2015

