










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkTourism & Management Studies
versão impressa ISSN 2182-8458versão On-line ISSN 2182-8466
TMStudies vol.15 no.2 Faro jun. 2019
https://doi.org/10.18089/tms.2019.150204
MANAGEMENT: SCIENTIFIC PAPERS
The feminization of the medical career in Brazil and work-family conflicts
A feminização da carreira médica no Brasil e conflitos trabalho-família
Daniela Cristina Machado Tameirão1, Simone Costa Nunes2
1Pontifícia Universidade Católica de Minas Gerais and Faculdade Atenas Sete Lagoas, Brazil, danielacmtameirao@gmail.com
2Pontifícia Universidade Católica de Minas Gerais, Brazil, sinunes@pucminas.br
ABSTRACT
This article deals, in a comparative manner from a gender perspective, with the occurrence of work-family conflicts and its antecedents, in the medical career of Brazilian professionals. The results indicate that the greater the stressors are presented at work or within the family, the greater the conflict tends to be, and the greater the social support in these two spheres, the lesser the conflict tends to be. Stressors related to work have shown themselves to be more significant than those related to the family, while social support at work is what succeeds in diminishing the effects of stressors in both spheres. Even though women have larger degrees of stress at work on average and less social support, there were no significant differences in terms of conflicts. This study contributes to a reflection on actions related to minimizing conflicts and promoting gender equality as well as the well-being of workers.
Keywords: Medical career, work-family conflicts, family-work conflicts, female medical, role stressors.
RESUMO
Este artigo trata, de maneira comparativa, na perspectiva de gênero, a ocorrência de conflitos trabalho-família e seus antecedentes, na carreira médica de profissionais brasileiros. Os resultados indicam que quanto maiores os estressores são apresentados no trabalho ou na família, maior o conflito tende a ser e quanto maior o suporte social nessas duas esferas, menor o tende a ser. Os estressores relacionados ao trabalho mostraram-se mais significativos do que os relacionados à família, enquanto o apoio social no trabalho é o que consegue diminuir os efeitos dos estressores nas duas esferas. Embora as mulheres tenham maior grau de estresse no trabalho, em média, e menos apoio social, não houve diferenças significativas em termos de conflitos. Este estudo contribui para uma reflexão sobre ações relacionadas à minimização de conflitos e promoção da igualdade de gênero e do bem-estar dos trabalhadores.
Palavras-chave: Carreira médica, conflitos trabalho-família, conflitos trabalho-família, medicina feminina, estressores.
1. Introduction
Dedication to work tends to absorb a large amount of an individual’s time and energy, as well as dedication to one’s family (Evans, 1996). Since the 1970s, various processes have led to significant transformations in work and family configurations, which have had repercussions in terms of the concept of career and family. As a consequence, the interface between professional and personal roles has become more tenuous in contemporary society, which makes for greater conflict between these two realms (Byron, 2005; Santos, 2015a) and has spurred interest in studying the work-family conflict phenomenon.
In the contemporary context, the development of science and technology, changes in society and health systems, and the feminization of the medical workforce are a few of the aspects that have affected medicine and have created an environment that is conducive to Work-Family Conflicts (Kilimnik, Bicalho, Oliveira & Mucci, 2012; Oliveira, Cavazotte, & Paciello, 2013).
From this perspective, it was outlined a study whose objective was to analyze the occurrence of work-family conflicts in Brazilian´s medical careers, in order to identify the antecedents that contribute to these occurrences and moderate them, and, from this study, an analysis was made taking into accounts gender issues. In other words, this article proposes a discussion that considers gender differences in the characterization of work-family conflicts in the medical career.
2. Theoretical approach
2.1 Career and Family
The notion of a career changed after the 1970s, due, among other things, to technological advances which affected the means of production, as well as, more widespread access to education, permitted greater ethnic diversification and feminization of the labor market (Chanlat, 1995). As a consequence, new forms of behavior converged to break with the then-current traditional career model (Andrade, Kilimnik & Pardini, 2011) leading to new challenges based on the desire to reconcile personal and professional lives (Silva, Dias, Silva, Krakauer & Marinho, 2011).
Both career concept and family concept were also be influenced by historical processes. Beginning in the 1960s, new concepts of the family and marriage resulted from a true revolution, brought about by the feminist movement and birth control. Sexuality was separated from reproduction, leading to an increase in the use of contraception, maternity after the age of 30, and a reduction in the number of children. These factors led women to leave the exclusivity of maternity and taking care of the home, to occupying the public sphere (Pereira & Schimanski, 2013).
In relation to families, we can verify an increase in consensual unions and a reduction in legal barriers to divorce, leading to successive marriages and the combination of children from different unions; homosexual unions; and, an increase in extended families, resulting from an increase in the elderly population (Pereira & Schimanski, 2013).
Given this scenario, many people have experienced difficulties in reconciling professional activities and family responsibilities, with each sphere interfering with the other with greater frequency (Santos, 2015b; Santos & Gonçalves, 2014).
2.2 The Medical Career and Feminization
The medical profession has reconfigured itself within this context of greater female participation, and it is also characterized by an intense rhythm, long working hours, various forms of hiring, and the need for continuous studying, which lead to a lack of time for family and friends (Kilimnik et al., 2012). These elements “are having a greater and greater effect on the choices and activities of physicians.” (Scheffer, Biancarelli & Cassenote, 2015, p.13).
A study by Scheffer, Cassenote, Guilloux, Biancarelli, Miotto & Mainard (2018) indicated the male dominance that existed in the Brazilian medical profession (more than 80%) up until the 1970s. In 1993, women represented 36% of Brazilian medicals; in 2000 this number had reached 40.8%; and, in 2014, women became the majority (54.8%). This trend has also occurred in Japan (Nomura & Gohchi, 2012), the United States, Canada and the other member nations of the OECD (The Organization for Economic Cooperation and Development) (Gjerberg, 2003; Wang & Sweetman, 2013).
Despite the number of women in the medical profession, inequalities in terms of gender have been revealed. In Brazil, women receive lower remuneration in comparison to their colleagues of the opposite sex, even when this involves similar conditions in terms of the number of labor ties, the complexity of the work and the hourly workload (Bruschini, 2007; Scheffer et al., 2015). In addition, they represent the minority in 36 of 54 medicals specialities (Scheffer et al., 2018). These inequalities reflect the influence of cultural traits and suggest that some medicals specialities are more appropriate for women given their gender characteristics (Gjerberg, 2003; Riska, 2011; Scheffer et al., 2018; Treister-Goltzman & Peleg, 2016). Just as in the corporate world (Carvalho Neto Tanure & Andrade, 2010; Tanure, Carvalho Neto & Andrade, 2006), the medical world is still characterized by a small number of women in leadership positions (Gjerberg, 2003; Nomura & Gohchi, 2012).
The progress of women in medical career has attracted interest on the part of many researchers, especially outside Brazil, with 40% of the articles about this subject being published in or after 2005. Some are conservative, others feminist, and some justify these inequalities based on the structural aspect of this career (concrete barriers or support that women or men receive in their career choices), while others point out that these differences result from the choices that these women have made in trying to reconcile their personal and professional lives (using the basic argument that women and men make career choices which confirm their respective normative gender roles in society) (Heiligers & Hingstman, 2000; Nomura & Gohchi, 2012; Treister-Goltzman & Peleg, 2016).
There are studies that suggest that the feminization of the medical career has advantages such as: female physicians are better at primary care since they generally have a more preventive orientation; they have a greater propensity to be empathetic with their patients, making their relationships more harmonious and collaborative; they tend to involve the patient more in decision making because they discuss treatments more; and they are less of a burden to the system because they are less inclined to use unnecessary technology (Riska, 2011; Scheffer et al., 2015; Tsugawa, Jena, Figueroa, Orav, Blumenthal & Jha, 2016). In negative terms, there are studies that reveal that female physicians tend to work fewer hours, are less available to work in medical shifts, are less likely to relocate, and are less represented in various medical specialties such as surgery and urology (Riska, 2011; Scheffer et al., 2018; Wang & Sweetman, 2013).
From the point of view of traditional heterosexual gender norms, one could suppose that differences exist between men and women in terms of the conflicts they experience in these two realms (work-family conflict - family-work conflict). From a different point of view, one could suppose that both experience similar conflicts since they share responsibilities in these two spheres, which is more and more common today. However, the results of various studies have not formed a consensus, because although they recognize that there are differences between the genders, they don’t reach any concrete conclusions (Van Daalen, Willemsen & Sanders, 2006).
Fadigas, Souza & Blerrenbach (1996) state that the effective participation of women in the labor market has also brought about structural changes for men, in both the work and the family spheres. Howell, Beckett, Nettiksimmons & Villablanca (2012, p.726) also argue that increasing work-family conflict - family-work conflict among men in dual career couples can be a symptom of these modifications, which they call the “new male mystique” or “the new dad.” This argument points to the possibility that men experience as many conflicts due to sociocultural changes as women do.
2.3 Work-Family Conflict
The definition of the work-family conflict phenomenon (Greenhaus & Beutell, 1985) is based on the Role Theory created by Kahn, Wolfe, Quinn, Snoek & Rosenthal (1964), which postulates the existence of a limited amount of time and energy, which makes the family and work realms incompatible, in some aspects, due to the different norms and requirements competing for the same resources (Michel, Mitchelson, Pichler, & Cullen, 2010). In other words, the individual perceives difficulties in meeting all of these concomitant pressures and experiences a conflict.
When professional duties interfere with the performance of family responsibilities, it is called work-family conflict (WFC) and when family responsibilities interfere with work it is termed a family-work conflict (FWC) (Greenhaus & Beutell, 1985). The literature displays a tendency to consider this construct as being bidirectional (Michel et al., 2010; Van Daalen et al., 2006), even though some studies consider work-family conflict and family-work conflict to have different antecedents and consequences (Oliveira et al., 2013).
The factors that contribute to the occurrence of WFC/FWC are mainly called Role Stressors, no matter they origin either from the spheres of work or private life (Greenhaus & Beutell, 1985; Michel et al., 2010).
The factors that contribute to attenuate WFC/FWC in each sphere form the concept of Social Support which deals with significant help from other people in the individual’s performance of her or his functions (Greenhaus & Beutell, 1985). These factors are termed moderators.
2.3.1 Role Stressors
Role Stressors can be related to the time invested in each of these spheres (time stressors), the tension caused by the role exercised (strain stressors) or the conflict/ambiguity in exercising these respective roles (behavior-based stressors) (Michel et al., 2010).
A time stressor occurs when the time spent doing the duties of one realm leaves less time to be involved in another realm. The extensive work schedule of a doctor leads to a lack of time and energy that can be dedicated to one’s personal life, and this is why it contributes to WFC/FWC (Tayfur & Arslan, 2013). Other examples of time stressors are: an inflexible or unpredictable schedule; working at night and during weekends; the number of hours spent in family activities such as taking care of children and other dependents; cleaning tasks; and the acquisition and preparation of food (Byron, 2005; Michel et al., 2010).
Strain stressors occur when the demands of one realm cause reactions such as irritability, anxiety, fatigue or apathy, affecting the performance of the other role. Examples include: overload in terms of roles; stressful work; characteristics of the organization where one works and work relationships; and conjugal and or parental conflicts (Byron, 2005; Michel et al., 2010).
Behavior-based stressors occur when the expectations of the conduct associated with a role are incompatible with the behavior expected in the other (Greenhaus & Beutell, 1985). Intimacy, typical of a family environment, is the opposite of the objectivity and impersonal behavior expected in the work environment. That being so, the individual needs to adjust her or his attitudes to the preconceived standards of each environment, and this ambiguity can generate apprehension. Some examples of these stressors are: the loss of information about the obligations and responsibilities required for a specific work role; multiple jobs; a misalignment between performance and personal expectations or the expectations of others (within the family or at work); facing difficulties in relationships with patients and their relatives; and ambiguity in family roles (Michel et al., 2010; Tayfur & Arslan, 2013).
From the perspective of gender and referring to disparities in medicine, Nomura and Gohchi (2012) state that female physicians often choose for part-time work schedules seeking to balance the demands of their personal and professional lives, but end up perceiving that they are treated with prejudice when they face greater obstacles in the development of their careers. These career obstacles can be noted by the offer of positions with less remuneration, difficulties in obtaining leadership positions, fewer opportunities to enter training courses made available by organizations and the veiled perception that they are less than welcome members of the medical team (Cabrera, 2007; Nomura & Gohchi, 2012). In this case, career choices, as objectives to reduce the impact of time stressors, end up leading to strain stressors when individuals are faced with the adverse psychological effects of these obstacles and the associated perceived prejudice, which are reflected in career standards, contributing to WFC/FWC (Nomura & Gohchi, 2012; Treister-Goltzman & Peleg, 2016).
Possibly, these prejudices and career obstacles perceived by the female physicians may also accentuate the behavior-based stressors, because these prejudices are derived from the expectation of a masculine standard of uninterrupted work and a full time commitment (Gjerberg, 2003; Cabrera, 2007). Wang and Sweetman (2013) reveal that data shows that gaps in a medical career arise due to the presence of children especially under the age of five, which leads to a redistribution of the hours that couples dedicate to their tasks at work and at home. The literature related to WFC/FWC indicates that the most prevalent stressors in the family sphere are related to the presence of children, and in the work sphere, the number of hours worked (Santos & Gonçalves, 2014).
2.3.2 Moderators: Social Support
Social Support can be divided into four types: emotional support (empathy, care, love and confidence); instrumental support (help in real-time, in terms of money, and energy); appraisal support (relevant information for self-assessment); informational support (advice information and suggestions) (Michel et al., 2010; Samsinar, Sambasivan, & Ismail, 2010).
The participation of third parties in the work sphere (the organization, supervisors, and colleagues) or the family sphere (spouse, relatives, friends, and domestic staff) constitutes a source of Social Support. Social Support can reduce WFC/FWC in two ways: reducing certain role pressures or acting as a moderator in the relationship between WFC/FWF and psychological well-being (Greenhaus & Beutell, 1985).
Social Support in the work sphere can occur through organizational policies and practices oriented toward benefitting family members or spontaneously based on the attitudes of peers (Gjerberg, 2003; Samsinar et al., 2010). Social Support on the part of the supervisor (Tayfur & Arslan, 2013) can include functional aspects (the providing of resources or space to solve work-related problems) and emotional aspects (demonstrating a preoccupation with problems that are related to work and not related to work). This Social Support is indispensable not only because it solves problems related to the performance of a function, but also because it reduces the perception of stressful factors, including those related to issues involving doctor-patient relationships and also increases the resources available to help workers overcome adversity.
Social Support in the family sphere is characterized by significant help from domestic staff or people with emotional ties, through attitudes such as sharing domestic tasks, collaborating in solving problems, supporting career decisions, exchanging information that makes it possible to reevaluate situations, and giving advice and supplying the psychic or physical support necessary to reduce the effects of stress that are being experienced (Samsinar et al., 2010).
The results are inconclusive in terms of how strong or what type of impact it has in minimizing WFC/FWC or the differences between men and women (Michael et al., 2010).
3. Methodology
This study uses the survey method with its collection instrument being a structured electronic questionnaire of 78 questions about the study object, as well as variables used to characterize this sample. The variables were extracted from the literature regarding this subject, mainly based on the metaanalyses of Byron (2005), Michel et al. (2010) and Van Daalen et al. (2006). Ten items were used to characterize WFC/FWC, using the scale of Netemeyer, Boles and McMurrian (1996). This scale was adapted to the Portuguese and Brazilian context by Aguiar and Bastos (2013). The questionnaire first went through a pre-test with 40 physicians.
This study was approved by the Institutional Research Ethics Board and the consent of the respondents was obtained.
The number of active physicians registered with the Federal Board of Medicine (CFM) totaled 390,737 (Conselho Federal de Medicina, 2016), and this was the population from which the sample was drawn. Being a resident physician was a criterion for exclusion, given that these individuals do not have autonomy over their work schedule and the workday is one of the points that most interferes in the occurrence of WFC/FWC. The composition of the sample was determined by the researchers’ contact networks and the expansion of this network based on contacts indicated by these participants. The sample members work in various medical specialities and regions of Brazil. In this manner, it can be characterized as a non-random snowball sample. The final sample consists of 336 respondents.
Factor Analysis was the technique selected to make it possible to consider all of the variables simultaneously to search for predominant patterns, and also because the phenomenon studied involves multidimensional and complex relationships (Hair, Black, Babin, Anderson & Tatham, 2009).
Initially, we adjusted the database and adjusted the sample by using the KMO (Kaiser-Meyer-Olkin) indicator. Then we used factor analysis to extract the items that were not contributing to the formation of the construct, using a varimax orthogonal rotation method. Each statistic variable was analyzed based on three parameters: factor load, communality and weight.
Structural Equation Modeling validated the Exploratory Factor Analysis and was performed using the PLS (Partial Least Square) approach. Structural Equation Modeling is divided into two stages: Measurement Model (Outer Model) and Structural Model (Inner Model).
The Outer Model verified its reliability (through Cronbach’s Alpha and its Composite Reliability), convergent and discriminant validity (using the Average Variance ExtractedAVE) and its dimensionality (according to the Parallel Analysis criterion). It was necessary to employ the Bootstrap method to calculate the confidence intervals and the weights for the Two-Step approach, given that the measurement structure presented some constructs which were not formed directly by the items (questions), but rather through latent variables (indicators).
The theoretical framework selected as the basis for this study’s criteria and arguments was extracted from the literature and has already been validated. That being so, the Inner Model analysis step was useful to evaluate to what extent the findings of this study correspond to the selected theoretical model. The quality of the fit was verified by R² and GoF. The β coefficient was also used to quantify the force and direction of the relationships between the constructs, as well as the β Standard Error and p-value. The construct indicators were created the items’ weighted averages and were standardized on a scale ranging from 0 to 100 (Hair et al., 2009).
4. Results
4.1 Characterization of the Sample and Gender Issues
The analysis revealed a sample of ages between 22 and 81, with the majority being of the female sex (68%), especially in the younger age groups, which is in keeping with studies which indicate a feminization of the medical career (Nomura & Gohchi, 2012; Scheffer et al., 2015, 2018; Wang & Sweetman, 2013).
In terms of marital status, 86% live/or have lived with their partner, with a larger proportion of men living with spouses (84%) than women (67%). Among those who reside with their partners, 73% of the women are part of a couple in which both have full-time careers, while only 45% of the men are in this situation. The basic argument that women and men make career choices that confirm that respective normative gender roles in society could be one of the explanations for this difference, as suggested by Cabrera (2007), Heiligers and Hingstman (2000), Nomura and Gohchi (2012) and TreisterGoltzman and Peleg (2016).
Among the respondents, 64% have biological or adopted children. Just 21% of the men in this sample do not have biological or adopted children, while 43% of the women do not, and this fact could reflect the overlapping of a woman’s most fertile years with the most critical years of a professional career (Carvalho Neto et al., 2010; Mache, Bernburg, Vitzthum, Groneberg, Klapp & Danzer, 2015; Montagner & Montagner, 2010; Tanure et al., 2006).
The majority of the respondents (72%) are located in the Southeastern region of Brazil, which is in keeping with the data from the Scheffer et al. (2015, 2018) studies. Only three states (federative unit) were not represented by the respondents (Piauí, Roraima and Tocantins). Another highlight of this sample is that 52% of the individuals work most of the time in the country towns of these states, but the geographic distribution did not indicate relevant differences between men and women, in terms of the regions of the country or the capital cities vs. country towns.
In terms of handling ambulatory cases, 87% of the respondents indicated that they do, but 53% do not attend on public institutions and the majority (53%) of those who do have passed a qualifying exam (form of hiring), with there being no relevant statistical difference between the results of the men and women. Of the 54% who have their own office, 87% handle patients who have supplementary health plans, as well as selfpaying patients. It may be noted that more men have their own offices (67%) than women (48%), and more men attend selfpaying patients in their offices (21%) than women (8%). In other words, they perform the same function, but it is more common for women to have lower remuneration, which is in accordance with Scheffer et al. (2015).
In terms of their professional practice in hospitals (hospital care), 76% of the respondents perform their services in hospitals (45% of them are performed as medical shifts). There was no statistically relevant difference between men and women men and women working in medical shifts, but more women (30%) do not attend patients in hospitals compared to men (11%), which is a finding also mentioned in the studies of Riska (2011), Scheffer et al. (2018), and Wang and Sweetman (2013).
Other modalities in terms of the exercise of the medical profession include performing paid functions on the administrative/association level or as professors/teacherresearchers, with the percentages in this sample being 13% and 27% respectively. In teaching, there are more men (30%) in coordinating positions than women (5%), confirming the pattern in medicine and in the corporate world of few women in leadership positions, as mentioned by Carvalho Neto et al. (2010), Gjerberg (2003), Nomura e Gohchi (2012) and Tanure et al. (2006).
4.2 Relationships Between the Constructs
Figure 1 presents the representative indicators of the constructs. The presence of rates for each direction, namely work interfering with the family and family interfering with work, makes it possible to identify the occurrences of WFC/FWC in the study sample. In addition, it is also possible to identify that the Role Stressors at work are significantly greater than the Role Stressors in the family, and Social Support in the family sphere was significantly greater than Social Support at work. That being so, the pressures generated by work in the medical profession are notorious in their impact on the private lives of these professionals.
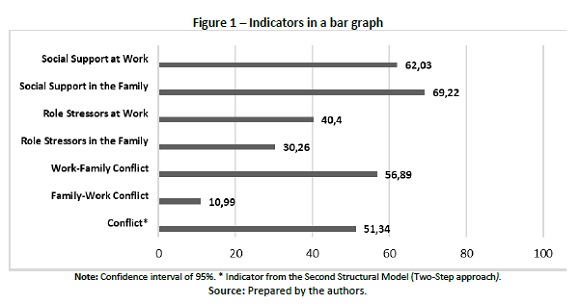
Figure 2 illustrates the structural model that results from the statistical interpretation of the collected data, utilizing the TwoStep approach, which validated the relationship between the constructs and their influence on the general results, based on the theoretical framework that this study is based on. We can affirm from this sample that the greater the Stressors at Work (β= 0.240) and or within the Family (β= 0.215), the greater the WFC/FWC tends to be (having a positive and significant influence with a p-value = 0.000). Stressors at Work had a greater impact than those within the Family. Together, the Role Stressors succeed in explaining 15.0% (R²) of the Conflict.
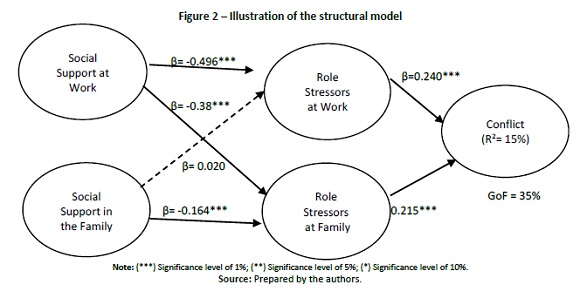
Another influential factor according to the data is Social Support at Work, which showed itself to be inversely correlated with the Role Stressors at Work (β= -0.496) and the Role Stressors in the Family (β= -0.538). Social Support in the Family also strongly influenced (p-value= 0.000) inversely (β= -0.164) the Role Stressors in the Family, however, it did not significantly influence (p-value= 0.680) the Role Stressors at Work. In other words, Social Support, whether it is at Work or in the Family realm, had a greater attenuating impact on stressors in the family sphere than in the work sphere, given that together they succeed in explaining 34.5% (R²) of the variability of the Role Stressors in the Family and 24.3% (R²) of the variability of the Role Stressors at Work. This finding corroborates the idea that Social Support can reduce WFC/FWC diminishing certain role pressures (Greenhaus & Beutell, 1985), or increasing the resources available to face adversity (Tayfur & Arslan, 2013).
Given these results, the lower the Social Support at work, the greater the impact of Role Stressors at Work and in the Family, and the lower the Social Support in the family, the greater the Role Stressors in the Family.
The indices encountered point to a moderate fit (GoF of 35.0%) between this study and the theoretical model that it is based on, which considers Social Support to be an antecedent to Role Stressors in the prediction of WFC/ FWC. From this perspective, individuals with a strong support system perceive these stressors less and, as a result, experience less conflict.
The Explanatory Factor Analysis made it possible to identify which variables contribute and to what extent to the occurrence or moderation of WFC/FWC, and thus identify the most influential antecedents in this sample. According to the results, it should be emphasized that the most significant stressors in the family realm are: the misalignment between the professionals’ planning of their careers and lives, as well as difficulty in dealing with personal expectations (behavior-based stressor), given that they cause some trouble for more than 60% of the respondents; the time invested in caring for family members who are not children/stepchildren (time stressor); and an environment characterized by conflict with children (strain stressor).
In terms of stressors in the work realm, the most prominent were long working hours (time stressor), relationship difficulties within a multidisciplinary team and with employees or patients, including the questioning of conduct (behaviorbased stressors). In terms of strain stressors, they are better determined through variables related to work relationships (difficulties with employer/instability in work relationships) and the conditions and type of work (workplace conditions, resources and stressful tasks).
In terms of Social Support in the work realm, the most prominent form was emotional support, coming from the organization as well as from peers (informal practices), acting as an important moderator of WFC/FWC. Among organizational policies and practices in terms of Social Support, there is instrumental support (flexibility of schedules, remuneration proportionate to tasks), informational support (opportunity for study and training which is necessary for technical improvement and support for following protocols) and appraisal support (feedback and the perception of credibility and good performance). In the family sphere, the attitudes of the spouse, of relatives, friends and employees in demonstrating solidarity, empathy and interest in career challenges represent emotional, informational and appraisal support, which are capable of moderating WFC/ FWC, even though they have a smaller impact compared to Social Support at work.
4.3 Indicators versus the Sex of the Respondents
Table 1 presents the comparative data for the Role Stressors at Work and in the Family, Social Support in these two spheres, and the sex of the respondents, using multiple comparison tests.
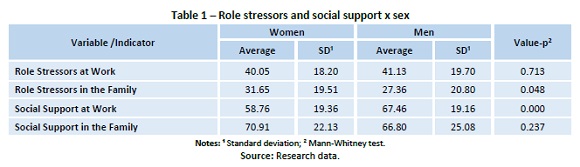
According to Table 1, the averages of Role Stressors in these two spheres differ for men and women, however it is only for Role Stressors in the Family that this difference is statistically significant, being greater for women than for men. This finding reflects the persistence of the heterosexual gender norms in terms of gender roles as has already been suggested by Bruschini (2007), Montagner and Montagner (2010) and Treister-Goltzman and Peleg (2016).
It was also verified that only Social Support at Work displayed a statistically significant difference between men and women. That being so, Social Support at Work is greater for men than for women, but for Social Support in the Family, the difference is not relevant in the examined sample. Thus, in this manner, we can observe that women receive less Social Support at Work, which is precisely the antecedent which has the greatest impact on WFC/FWC effects. These gender inequalities within the medical profession have also been pointed out by Nomura and Gohchi (2012), Riska (2011) and Treister-Goltzman and Peleg (2016). For both men and women, the Social Support at work presents a positive and significant correlation with the age of the individual, that is, the older the individual, the greater the reported support in the sphere of work. On the other hand, the Social Support indicators in the Family, the Role Stressors at Work, the Role Stressors in the Family and the Conflict have the negative and significant correlations, that is to say, the greater the age of the individuals the smaller the indicator’s average value.
Table 2 presents the results of the comparative analysis between WFC, FWC and Conflicts (as a bidirectional indicator) and the sex of the respondents.
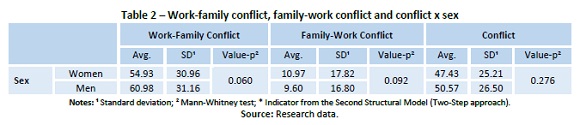
It can be verified that the averages for Work-Family Conflict (WFC), Family-Work Conflict (FWC) and Conflict (WFC/FWC) differ between men and women, however the differences do not have statistical significance (p-value > 0.05). That being so, in the studied sample as well as the study conducted by Van Daalen et al. (2006), differences between the genders in terms of WFC/FWC antecedents were verified, but the results did not present statistically significant differences in the perception of WFC/FWC. Fadigas et al. (1996) state that the effective participation of women in the labor market has also led to structural modifications for men in both the work and family spheres. In accordance with this, Van Daalen et al. (2006) and Howell et al. (2012) argue that perhaps men and women experience similar conflicts given that it is increasingly common for them to share responsibilities in both of these spheres due to socio-cultural changes.
5. Conclusions
This study’s findings reveal that Role Stressors at work are significantly greater than those that come from the family and have a greater impact on WFC/FWC. In addition, even though individuals tend to receive more Social Support from their family than at work, it is precisely this Social Support at work which manages to diminish the stressors in both of these spheres (work/home).
The results make it clear that in terms of the antecedents in the work sphere, both pressures (stressors) and Social Support (moderators) affect WFC/FWC of those in the medical profession. That being so, this reinforces the importance of personal relationships and work relationships, as well as management practices and work conditions in the occurrence of WFC/FWC in the medical careers of Brazilian professionals. Thus, decentralizing the responsibility of physicians to balance the various demands that they are subject to, becomes a topic of great relevance.
In terms of the differences between the sexes in relation to the indicators, in the sample that we have studied Social Support at Work is less for women than for men, and Role Stressors in the Family are greater for women than for men. Despite these differences in terms of the antecedents, WFC/FWC does not differ statistically between men and women.
It is possible to imagine that the differences between the stressor and moderator antecedents result from cultural differences in traditional heterosexual gender norms at work and in the family. They may also reflect career obstacles and choices related to gender, as suggested by the literature.
However, since the gender gaps in both spheres do not reflect greater or less conflict, it is thus evident that there are other aspects that have not been contemplated in this study. We may speculate that a limitation of this study may be that it does not consider other intervening factors such as the centrality of the individual in some of these spheres and individual personal resources and coping mechanisms. In addition, another limitation could be the factor that this is a cross-sectional study, which does not identify causal relationships. However, these limitations can provide inspiration for future studies.
The social transformation process which has resulted from the increasing feminization of the labor market has brought many demands to the female universe, both from an economic point of view as well as in terms of personal fulfillment. Even though equal rights are guaranteed by the Constitution, the differences between the sexes have not been reconciled, possibly because there are cultural and traditional processes that guide this behavior. In any event, according to the results of this and other studies, even women who experience a large number of dilemmas and contradictions, have managed to balance this situation, perhaps because there are more and more nonstereotyped solutions available which are also the result of social transformations. It remains to investigate the solutions that they have found to overcome gender inequalities with deeds and not just words.
Given this situation, greater reflection is needed in terms of gender inequalities in careers in general, involving the evaluation of structural aspects of careers (obstacles and choices) and the impact of social and normative aspects of society in the search for finding a balance between one’s personal and professional lives. The ideal scenario would be to add data regarding psychic aspects (the centrality of the individual and coping mechanisms) which contribute to this balance and to find a better explanation of the socio-cultural changes from the feminization of careers that have affected male behavior in both the realms of work and the family.
As an empirical contribution to the field, this study demonstrates the pertinence of studying the medical career, and learning the characteristics, expectations and difficulties which affect its professionals as well as its trends. The information provided here in respect to this profession’s profile can contribute in the form of an empirical platform which can inform debate and guide the development of policies and organizational, personal and collective actions related to conflicts which are designed to make personal and professional lives more compatible. In addition, this study stimulates the discussion of the participation of women in this career and thus promotes gender equality in both the work and domestic spheres.
In terms of its theoretical contribution, one aspect that gives this study relevance is the fact that the subject of work-family conflicts has not been widely explored by researchers in Brazil, especially in terms of a quantitative approach, according to Oliveira et al. (2013), and as Mache et al. (2015) note, it is even rarer to find a study about this subject that examines the medical profession.
REFERENCES
Aguiar, C.V.N., & Bastos, A.V.B. (2013). Tradução, adaptação e evidências de validade para a medida de conflito trabalho-família. Avaliação Psicológica, 12(2), 203-212. [ Links ]
Andrade, G.A., Kilimnik, Z.M., & Pardini, D.J. (2011). Carreira tradicional versus carreira autodirigida ou proteana: um estudo comparativo sobre a satisfação com a carreira, a profissão e o trabalho. Revista de Ciências da Administração, 13(31), 58-80. [ Links ]
Bruschini, M.C.A. (2007). Trabalho e gênero no Brasil nos últimos dez anos. Cadernos de Pesquisa, 37(132), 537-572 [ Links ]
Byron, K. (2005). A meta-analytic review of work-family conflict and its antecedents. Journal of Vocational Behavior, 67, 169-198. [ Links ]
Cabrera, E.F. (2007). Opting out and opting in: understanding the complexities of women's career transitions. Career Development International, 12(3), 218 - 237. [ Links ]
Carvalho Neto, A., Tanure, B., & Andrade, J. (2010). Executivas: carreira, maternidade, amores e preconceitos. RAE-eletrônica, 9(1), 1-23. [ Links ]
Conselho Federal de Medicina (Brasil). (2016). Estatística. Brasília: CFM. Retrieved 25.08.2018 from http://portal.cfm.org.br/?option=com_estatistica. [ Links ]
Chanlat, J.F. (1995). Quais carreiras e para qual sociedade? Revista de administração de Empresas, 35(6), 67-75. [ Links ]
Evans, P. (1996). Carreira, sucesso e qualidade de vida. Revista de administração e Empresas, 36(3), 14-22. [ Links ]
Fadigas, A.M.; Souza, E.A.F., & Blerrenbach M.I.R.S. (1996). Toda nudez será castigada. RAELigtht, 3(2), 12-14. [ Links ]
Gjerberg, E. (2003). Women doctors in Norway: the challenging balance between career and family life. Social Science & Medicine, 57, 13271341. [ Links ]
Greenhaus, J.H., & Beutell, N.J. (1985). Sources of conflict between work and family roles. Academy of Management Review, 10(1), 76-88. [ Links ]
Hair Jr., J.F., Black, W.C., Babin, B.J., Anderson, R.E., & Tatham, R. L. (2009). Análise multivariada de dados. Porto Alegre: Bookman. [ Links ]
Heiligers, P.J.M., & Hingstman, L. (2000). Career preferences and the work-family balance in medicine: gender differences among medical specialists. Social Science & Medicine, 50, 12351246. [ Links ]
Howell, L.P., Beckett, L.A., Nettiksimmons, J., & Villablanca A.C. (2012). Generational and gender perspectives on career flexibility: ensuring the faculty workforce of the future. The American Journal of Medicine, 125, 719-728. [ Links ]
Kilimnik, Z.M., Bicalho, R.F.S., Oliveira, L.C.V., & Mucci, C.B.M.R. (2012). Análise do estresse, fatores de pressão do trabalho e comprometimento com a carreira: um estudo com médicos de uma unidade de pronto-atendimento de Belo Horizonte, Minas Gerais. Gestão & Planejamento, 12(3), 668-693. [ Links ]
Mache, S., Bernburg, M., Vitzthum, K., Groneberg, D.A., Klapp, B.F., & Danzer,G. (2015). Managing work-family conflict in the medical profession: working conditions and individual resources as related factors. BMJ Open, 5, 1-9. [ Links ]
Michel, J.S., Mitchelson, J.K., Pichler, S., & Cullen, K.L. (2010). Clarifying relationships among work and family social support, stressors, and work-family conflict. Journal of Vocational Behavior, 76, 91-104. [ Links ]
Montagner, M.I., & Montagner, M.A. (2010). Mulheres e trajetórias na Faculdade de Ciências Médicas da Unicamp: vozes singulares e imagens coletivas. História, Ciências, Saúde, 17(2), 379-397. [ Links ]
Nomura, K., & Gohchi, K. (2012). Impact of genderbased career obstacles on the working status of women medicals in Japan. Social Science & Medicine, 75, 1612-1616. [ Links ]
Oliveira, L.B., Cavazotte, F.S.C.N., & Paciello, R.R. (2013). Antecedentes e consequências dos conflitos entre trabalho e família. Revista de Administração Contemporânea, 17(4), 418-437. [ Links ]
Pereira, C.M., S. & Schimansk, E. (2013). Família, gênero e novas configurações familiares: um olhar sobre a mulher e a condição de pobreza. Revista Magistro, 8(2), 163-179. [ Links ]
Riska, E. (2011). Gender and medical careers. Maturitas, 68, 264267. [ Links ]
Samsinar, M.S., Sambasivan, M., & Ismail,I. (2010). Relationship between work-family conflict and quality of life: an investigation into the role of social support. Journal of Managerial Psychology, 25(1), 5881. [ Links ]
Santos, H. B. (2015a). The dual career process in Brazilian perspective: unraveling typologies. Revista de Administração, 50 (4), 507-522.
Santos, H. B. (2015b). Casamento, casa e carreira: agora quem fala são as organizações. Anais do Encontro Nacional da Associação Nacional de Pós-Graduação e Pesquisa em Administração, Belo Horizonte, MG, Brasil, 39.
Santos, J.V., & Gonçalves, G. (2014) Contribuição para a adaptação portuguesa das escalas de conflito trabalho-família e conflito famíliatrabalho. Revista Eletrônica de Psicologia, Educação e Saúde, 2, 14-30. [ Links ]
Scheffer, M., Biancarelli, A., & Cassenote, A. (2015). Demografia médica no Brasil 2015. São Paulo: Departamento de Medicina Preventiva, Faculdade de Medicina da USP. Conselho Regional de Medicina do Estado de São Paulo. Brasília: Conselho Federal de Medicina. [ Links ]
Scheffer, M., Cassenote, A., Guilloux, A.G.A., Biancarelli, A., Miotto, B.A., & Mainard, G.M. (2018). Demografia médica no Brasil 2018. São Paulo: Departamento de Medicina Preventiva, Faculdade de Medicina da USP. Conselho Regional de Medicina do Estado de São Paulo. Brasília: Conselho Federal de Medicina. [ Links ]
Silva, R.C., Dias, C.A.F., Silva, M. T. G., Krakauer, P. V.C., & Marinho, B.L. (2011). Carreiras: novas ou tradicionais? Um estudo com profissionais brasileiros. Anais do Encontro Nacional da Associação Nacional de PósGraduação e Pesquisa em Administração, Rio de Janeiro, RJ, Brasil, 35.
Tanure, B., Carvalho Neto, A., & Andrade, J. O. (2006). A super executiva às voltas com carreira, relógio biológico, maternidade, amores e preconceitos. Anais do Encontro Nacional da Associação Nacional de Pós-Graduação e Pesquisa em Administração, Salvador, BA, Brasil, 30.
Tayfur, O., & Arslan, M. (2013). The role of lack of reciprocity, supervisory support, workload, and work-family conflict on exhaustion: evidence from medicals. Psychology, Health & Medicine, 5, 564575. [ Links ]
Treister-Goltzman, Y., & Peleg, R. (2016). Female medicals and the Work-Family Conflict. Israel Medical Association Journal, 18(5), 261266. [ Links ]
Tsugawa, Y., Jena, A.B., Figueroa, J.F., Orav, E.J., Blumenthal, D. M., & Jha, A.K. (2016). Comparison of hospital mortality and readmission rates for medicare patients treated by male vs female medicals. JAMA Internal Medicine. Retrieved from http://jamanetwork.com/. [ Links ]
Van Daalen, G., Willemsen, T. M., & Sanders, K. (2006). Reducing workfamily conflict through different sources of social support. Journal of Vocational Behavior, 69, 462-476. [ Links ]
Wang, C., & Sweetman, A. (2013). Gender, family status and the medical labour supply. Social Science & Medicine, 94, 17-25. [ Links ]
Received: 25.09.2018
Revisions required: 20.12.2018
Accepted: 14.03.2019

