Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Portuguesa de Medicina Geral e Familiar
Print version ISSN 2182-5173
Rev Port Med Geral Fam vol.36 no.2 Lisboa Apr. 2020
https://doi.org/10.32385/rpmgf.v36i2.12604
REVISÕES
Family determinants as a risk factor for chronic obstructive pulmonary disease: a systematic review
Determinantes familiares como fator de risco para doença pulmonar obstrutiva crónica: uma revisão sistemática
Ana Martins,1
 https://orcid.org/0000-0003-1799-3048
https://orcid.org/0000-0003-1799-3048
Susana Vasques,2
Paulo Santos3-4
1 Faculdade de Medicina, Universidade do Porto.
2 Médica Interna de Medicina Geral e Familiar. USF Ermesinde, ACeS Grande Porto III - Maia/Valongo.
3 Departamento de Medicina da Comunidade, Informação e Decisão em Saúde (MEDCIDS). Faculdade de Medicina, Universidade do Porto.
4 Centro de Investigação em Tecnologias e Serviços de Saúde (CINTESIS). Universidade do Porto.
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Chronic obstructive pulmonary disease (COPD) is a preventable respiratory disease, with repercussions in quality of life. Worldwide COPD is a leading cause of mortality. Cigarette smoking is the most debated risk factor, but it’s important to identify other determinants at stake. Family context and behaviors have an impact on the individual’s health.
Objective: This systematic review aims to characterize family determinants as possible risk factors for the development of COPD.
Methods: A systematic search was conducted in PubMed, followed by a three-step selection process. Data were processed by two independent reviewers and studies were gathered based on pre-defined variables. English written, articles about risk factors for COPD related to the familiar context, meta-analysis, case-control, cohort, and cross-sectional studies were included. The family determinants considered were childhood maltreatment, education level of the patient, socioeconomic status and family history of tobacco.
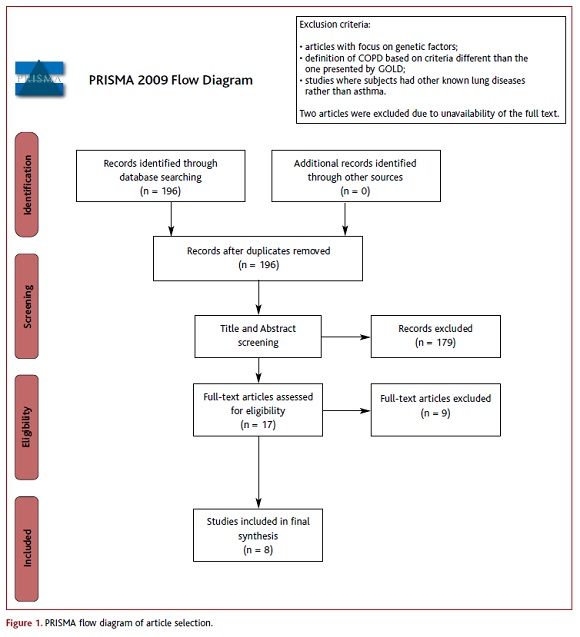
Results: From 196 references retrieved, inclusion and exclusion criteria were applied, and eight studies were included. This review found six articles about education, one about socioeconomic status, one about family history of tobacco and one about childhood maltreatment as possible risk factors. One of the studies was a meta-analysis that did not contain any of the other studies included.
Conclusions: Little evidence is available on the effect of family determinants in the development of COPD. The studies reported an association between COPD and low socioeconomic status and low education and interaction with childhood maltreatment.
Keywords: Chronic obstructive pulmonary disease; Family; Risk factors.
RESUMO
Introdução: A doença pulmonar obstrutiva crónica (DPOC) é uma doença respiratória evitável, com uma repercussão na qualidade de vida. A DOPC é uma das principais causas de morte. O tabaco é o fator de risco mais debatido, mas é importante identificar outros determinantes. O contexto e comportamentos familiares apresentam um impacto na saúde individual.
Objetivo: Esta revisão sistemática pretende caracterizar determinantes familiares como possíveis fatores de risco para o desenvolvimento de DPOC.
Métodos: Uma pesquisa sistemática foi conduzida na PubMed, seguida por um processo de seleção com três fases. A informação foi processada por dois revisores independentes e os estudos foram escolhidos com base em variáveis pré-definidas. Estudos em inglês, artigos sobre fatores de risco para DPOC relacionados com o contexto familiar, estudos de meta-análise, casoscontrolo, coorte e transversais foram incluídos. Os determinantes familiares considerados foram maus tratos na infância, nível socioeconómico, educação e história familiar de tabaco.
Resultados: Após a aplicação de critérios de inclusão e exclusão foram incluídos oito artigos de 196 encontrados. Esta revisão encontrou seis artigos sobre educação, um sobre o nível socioeconómico, um sobre história familiar de tabaco e um sobre maus tratos na infância como possíveis fatores de risco. Um dos estudos consiste numa meta-análise, a qual não inclui os outros estudos.
Conclusões: Existe pouca evidência disponível sobre o efeito de determinantes familiares no desenvolvimento da DPOC. Os estudos incluídos mostraram uma associação entre DPOC e um baixo nível educacional e baixo nível socioeconómico e uma interação com abusos na infância.
Palavras-chave: Doença pulmonar obstrutiva crónica; Família; Fatores de risco.
Introduction
Chronic obstructive pulmonary disease (COPD) is defined by airflow obstruction that is not fully reversible. It is a preventable and treatable common respiratory disease.1 Spirometry is used as a diagnostic tool and the presence of a post-bronchodilator FEV1/FVC < 0.70 confirms the presence of COPD.1
Worldwide COPD is a leading cause of morbidity and mortality.2-3 In 2010, the number of cases of COPD was estimated to be 384 million, with a global prevalence of 11.70% (CI95%, 8.40-15.00%).4 According to the World Health Organization (WHO), COPD is the fourth cause of death in the world.5 About 3 million people die every year with COPD and it is expected that, by 2030, it will be the third leading cause of death worldwide.6-7
Cigarette smoking is the most debated known risk factor for COPD. However, COPD also develops in non-smokers.8 Besides, the burden of COPD is still increasing even though the smoking rate has recently decreased.9
Besides the genetic factors, there are many environmental factors associated with the incidence of COPD. Factors that influence disease development include age and sex, exposure to particles, infections, lung growth and development. The role of childhood maltreatment, education, socioeconomic status and family history of tobacco is still open to debate.1
Social determinants of health represent conditions in which individuals are born and live that play an active role in their health. These include situations like early childhood experiences and development, social support and educational opportunities. Therefore, family context and behaviors have an impact in the individual’s health.10
Primary care plays a crucial role in the continuity of care, since the early onset of risk factors to the development and progression of COPD, putting it in the best position to act preventively, especially in high-risk individuals and their respective families. Tobacco smoking and environmental exposure to pollutants are quite known factors. It is important to identify other determinants at stake. The aim of this review is to characterize family determinants as possible risk factors for the development of COPD in order to early detect high-risk individuals.
Methods
A systematic search was conducted in PubMed between November 10 and January 22, 2019, using as a query a combination of ‘family’, ‘risk factors’ and ‘Pulmonary Disease, Chronic Obstructive’. English written articles and articles performed in humans were included. No time limits were applied. Subsequently, a selection process was carried out in three stages. The data was processed by two independent reviewers and the information was collected based on pre-defined variables. In the first step, titles and abstracts were selected, and articles proceeded to the second stage after the inclusion by at least one reviewer. Within the second stage, full-text was evaluated and the disagreements were discussed and solved by consensus.
Inclusion criteria were: articles about risk factors for COPD related to the familiar context, casecontrol studies, cohort studies, meta-analysis, and cross-sectional studies. Exclusion criteria were: articles with a focus on genetic factors; those in whom COPD defined by spirometry was explicitly based on spirometric criteria different than the one presented by GOLD; studies where subjects had other known lung diseases except asthma.
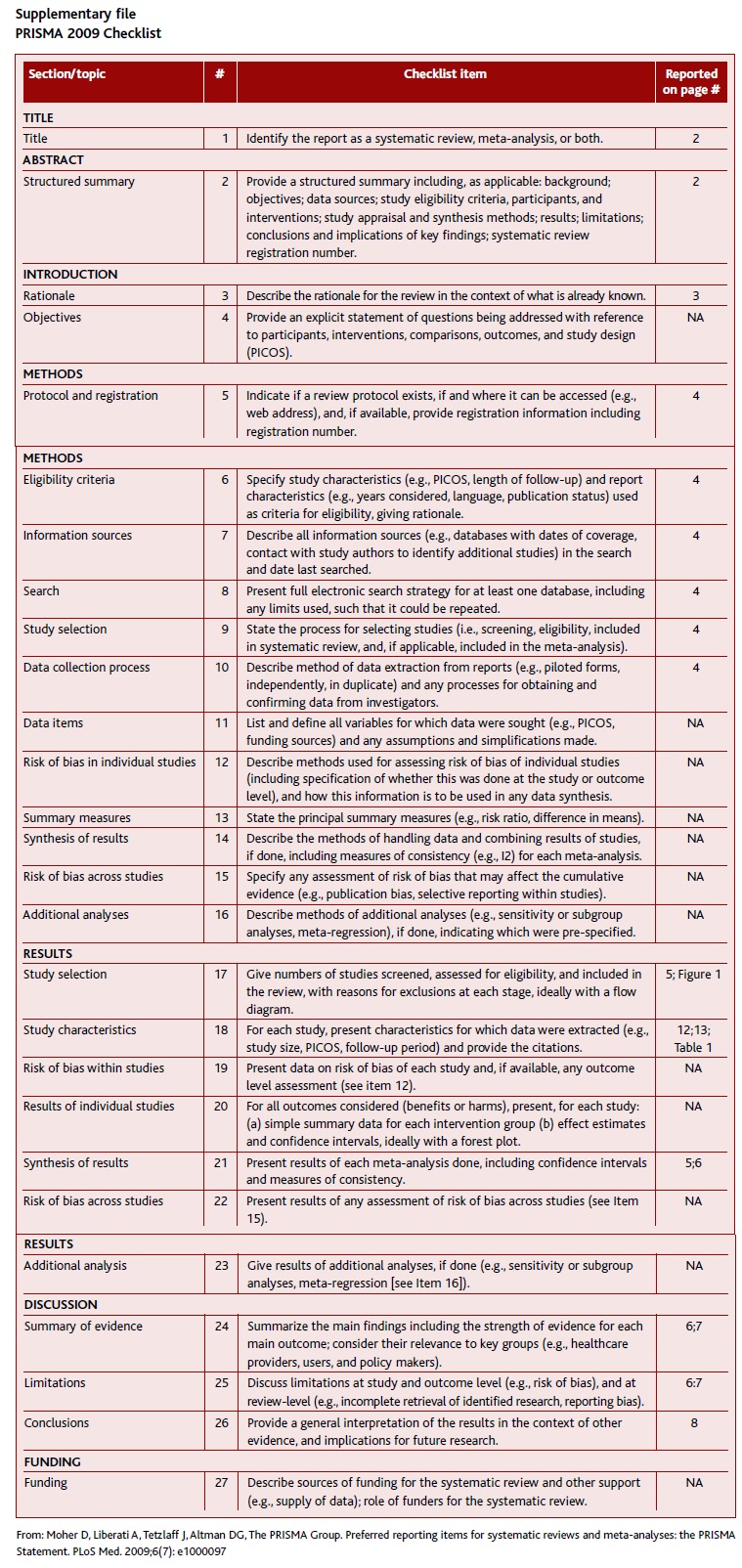
Data on the significance of each study were pooled, with a statistically significant value defined as p<0.05. This review was performed based on Items Preferred Reports for Systematic Reviews and Guidance Indicators for Meta-Analyzes (PRISMA).11 PRISMA checklist is available on supplementary file.
Results
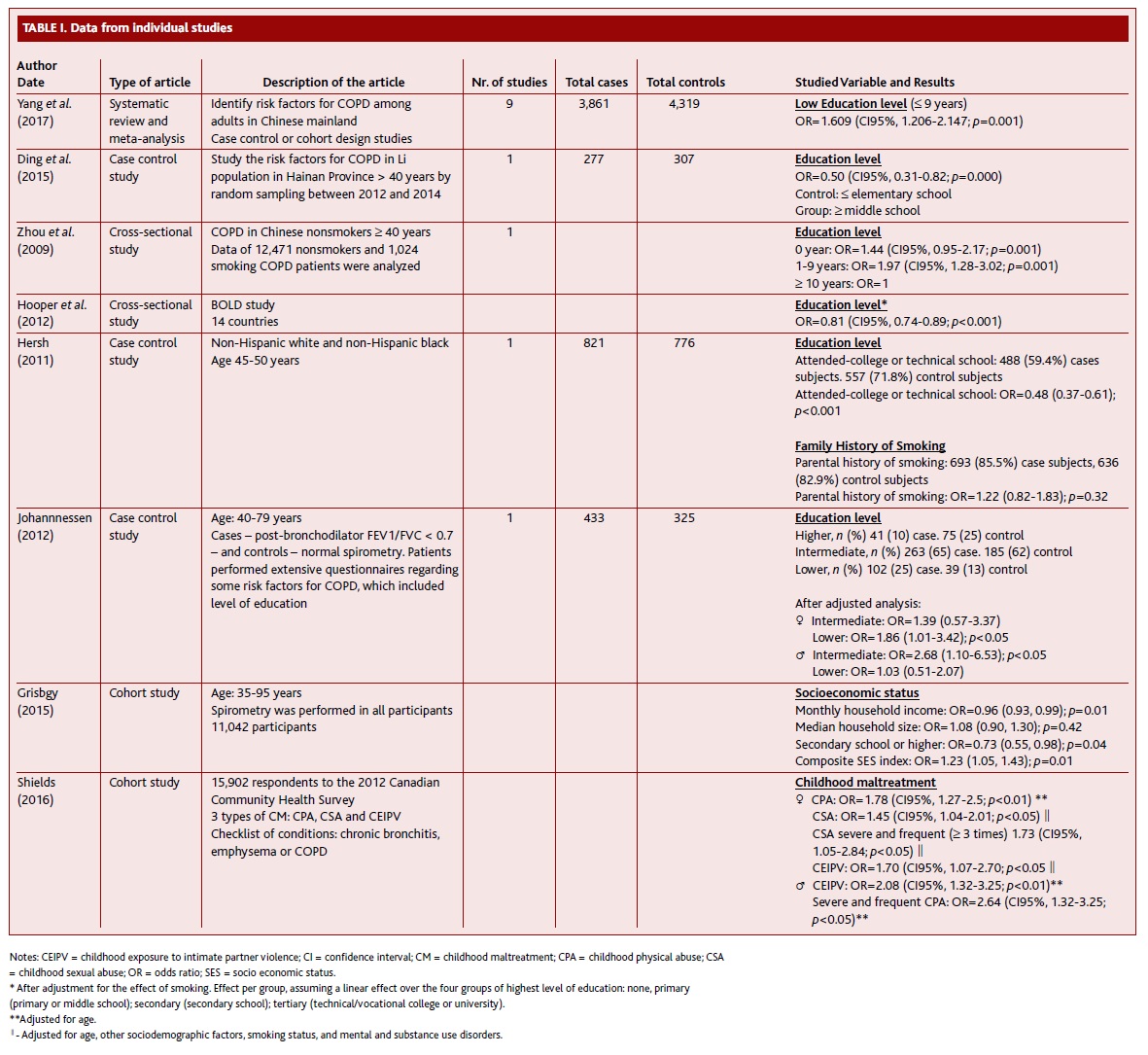
From 196 references retrieved, inclusion and exclusion criteria were applied, and eight studies were included in the final revision. The flow diagram summarizing the study identification and selection is shown in Figure 1. This review found six articles about education, one about socioeconomic status, one about family history of tobacco and one about childhood maltreatment as possible risk factors for COPD (Table I). One of the studies was a meta-analysis that did not contain any of the other studies included. In seven studies, COPD was defined by post-bronchodilator spirometry criteria (FEV1/FVC < 0.7). In another study, the presence of COPD was only based on questionnaire answers.
(clique para ampliar ! click to enlarge)
Education level
All six studies showed an association between low educational level and COPD.
One of the studies showed that lower educational achievement was associated with COPD in women (OR=1.86; CI95%, 1.01-3.42; p<0.05). In men, the level of education was also a risk factor for COPD (OR=2.68; CI95%, 1.10-6.53; p<0.05).12 However, the categorization of education level is not explicit enough.
Education level equal or inferior to ninth grade was a risk factor for COPD.13
Low educational level was associated with stages I-IV COPD in non-smokers. Stage 0 was not found to be associated with education to the same degree as stages II or higher and stage I. Lower educational level was a risk factor for non-smoking COPD patients (0 years: OR=1.44; CI95%, 0.95-2.17, and 1-9 years: OR=1.97; CI95%, 1.28-3.02).14 It should be noted that stage 0 (chronic obstruction with preserved lung function) is no longer part of the GOLD criteria for COPD. A higher level of education was strongly and significantly associated with less disease (OR=0.81; CI95%, 0.74-0.89; p<0.001).15
In other study, high educational level (defined as middle school or higher) seemed to be protective for COPD (OR=0.50; CI95%, 0.31-0.82; p<0.001), but it didn’t confirm after the adjustment in a multivariate model including exposure to pollutants.16
Socioeconomic status
One study evaluated the relation between socioeconomic status and COPD. Lower composite socioeconomic status index was associated with higher odds of having COPD (OR=1.23; CI95%, 1.05-1.43; p=0.01), and higher household income showed to be protective (OR=0.96; CI95%, 0.93-0.99; p=0.01). However, the authors were not able to adjust for occupation, which could influence the association between socioeconomic status and COPD.17
Family history of smoking
The relationship between parental history of smoking and childhood environmental tobacco smoke exposure was studied. Although the history of smoking in the relatives is very common (more than 80%), it didn’t seem to be a significant predictor of COPD (OR=1.22; CI95%, 0.82-1.83; p=0.32).18
Childhood maltreatment
COPD was related to childhood maltreatment in children according to sex. Among women, the binary childhood physical abuse was significantly associated with COPD after controlling for age (OR=1.78; CI95%, 1.27-2.5; p<0.01). A dose-response relationship was found between childhood physical abuse and COPD when severity and frequency were considered (OR=3.51; CI95%, 1.82-6.77, for severe and frequent childhood physical abuse and OR=2.44; CI95%, 1.50-3.98, for severe childhood physical abuse, ≤ 10 times). After fully adjustment controlling for smoking status and other covariates, the association persisted both with childhood sexual abuse (OR=1.45; CI95%, 1.04-2.84; p<0.05) and childhood exposure to intimate partner violence (OR=1.70; CI95%, 1.07-2.7; p<0.05), but not with childhood physical abuse. The authors also noticed that, among females that never smoked, childhood physical abuse and childhood exposure to intimate partner violence were associated with COPD, but not childhood sexual abuse (childhood physical abuse, OR=2.29; CI95%, 1.17-4.47; p<0.05; childhood exposure to intimate partner violence, OR=3.15; CI95%, 1.26-7.91; p<0.05).
Among males, COPD was associated with childhood exposure to intimate partner violence (OR=2.08; CI95%, 1.32-3.25; p<0.01) and severe and frequent childhood physical abuse (OR=2.64; CI95%, 1.32-3.25; p<0.05) but this association did not persist after the fully adjusted model. The authors found that smoking and mental and substance use disorders were important mediators in associations between childhood maltreatment and COPD. The associations that persisted after the full adjustment suggest that other pathways may be involved in the associations between childhood maltreatment and COPD.19
This systematic review assessed family determinants as a risk factor for the development of COPD. We considered family determinants such as childhood maltreatment, education level, socioeconomic status and family history of tobacco. According to the data available, low socioeconomic status is associated with the development of COPD.20-21
All six articles about education level showed an association between a lower level of education and the development of COPD. One showed no significant correlation with education, suggesting it isn’t a high-risk factor for COPD.16 The association between family history of smoking and COPD was not significant.18 One article found that smoking and mental and substance use disorders were important mediators in the associations between childhood maltreatment and COPD.19
Therefore, education level and socioeconomic status are important family determinants that play a role in the development of COPD.
Nevertheless, only eight articles were included in the final synthesis and some limitations can be pointed out. The definition of the level of education was not equal between the studies analyzed and in one of the studies, it was not defined. Education is also closely related to socioeconomic status. In one of the studies, socioeconomic status was defined by educational achievement, but it can also be measured by other individual factors. The article about childhood maltreatment refers not only to violence in the family but also in school and neighborhood, so we cannot attribute the entire effects to the role of the family. Also, it is prone to recall bias, which could have interfered with the associations between childhood maltreatment, smoking, and COPD.
This systematic review has a few limitations. Due to the heterogeneity of the data collected, we could not perform a quantitative meta-analysis. Also, neither a publication bias nor quality assessments were performed. Nevertheless, our conclusions are an appropriate summary of the current evidence available on this topic.
Conclusion
Little evidence is available on the effect of family behaviors or environment conditionings in the development of Chronic Obstructive Pulmonary Disease, a preventable cause of chronic morbidity and mortality.1 The studies gathered reported an association between COPD and low socioeconomic status and with low education and interaction with childhood maltreatment. Although tobacco and environment exposure to pollutants are the main factors to pay attention in the risk estimation for COPD, it is important to identify other potential conditioners, especially in primary prevention, selecting those patients to stress the tobacco eviction and cessation and to protect from hostile environments, such as low socioeconomic status and low education.
REFERENCES
1. Singh D, Agusti A, Anzueto A, Barnes PJ, Bourbeau J, Celli BR, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: the GOLD Science Committee Report 2019. Eur Respir J. 2019;53(5):1900164. [ Links ]
2. Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095-128. [ Links ]
3. Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163-96. [ Links ]
4. Adeloye D, Chua S, Lee C, Basquill C, Papana A, Theodoratou E, et al. Global and regional estimates of COPD prevalence: systematic review and meta-analysis. J Glob Health. 2015;5(2):020415. [ Links ]
5. World Health Organization. World health statistics 2008. Geneva: WHO; 2008. [ Links ] ISBN 9789240682740
6. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117-71. [ Links ]
7. World Health Organization. Burden of COPD 2011 [homepage]. Geneva: WHO; [s.d.]. Available from: https://www.who.int/respiratory/copd/burden/en/ [ Links ]
8. Andreeva E, Pokhaznikova M, Lebedev A, Moiseeva I, Kozlov A, Kuznetsova O, et al. The RESPECT study: RESearch on the PrEvalence and the diagnosis of COPD and its Tobacco-related etiology: a study protocol. BMC Public Health. 2015;15:831. [ Links ]
9. Lee SJ, Kim SW, Kong KA, Ryu YJ, Lee JH, Chang JH. Risk factors for chronic obstructive pulmonary disease among never-smokers in Korea. Int J Chron Obstruct Pulmon Dis. 2015;10:497-506. [ Links ]
10. Andermann A. Taking action on the social determinants of health in clinical practice: a framework for health professionals. CMAJ. 2016;188(17-18):E474-83. [ Links ]
11. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151(4):W65-94. [ Links ]
12. Johannessen A, Bakke PS, Hardie JA, Eagan TM. Association of exposure to environmental tobacco smoke in childhood with chronic obstructive pulmonary disease and respiratory symptoms in adults. Respirology. 2012;17(3):499-505. [ Links ]
13. Yang Y, Mao J, Ye Z, Li J, Zhao H, Liu Y. Risk factors of chronic obstructive pulmonary disease among adults in Chinese mainland: a systematic review and meta-analysis. Respir Med. 2017;131:158-65. [ Links ]
14. Zhou Y, Wang C, Yao W, Chen P, Kang J, Huang S, et al. COPD in Chinese nonsmokers. Eur Respir J. 2009;33(3):509-18. [ Links ]
15. Hooper R, Burney P, Vollmer WM, McBurnie MA, Gislason T, Tan WC, et al. Risk factors for COPD spirometrically defined from the lower limit of normal in the BOLD project. Eur Respir J. 2012;39(6):1343-53. [ Links ]
16. Ding Y, Xu J, Yao J, Chen Y, He P, Ouyang Y, et al. The analyses of risk factors for COPD in the Li ethnic group in Hainan, People’s Republic of China. Int J Chron Obstruct Pulmon Dis. 2015;10:2593-600. [ Links ]
17. Grigsby M, Siddharthan T, Chowdhury MA, Siddiquee A, Rubinstein A, Sobrino E, et al. Socioeconomic status and COPD among lowand middle-income countries. Int J Chron Obstruct Pulmon Dis. 2016;11:2497-507. [ Links ]
18. Hersh CP, Hokanson JE, Lynch DA, Washko GR, Make BJ, Crapo JD, et al. Family history is a risk factor for COPD. Chest. 2011;140(2):343-50. [ Links ]
19. Shields ME, Hovdestad WE, Gilbert CP, Tonmyr LE. Childhood maltreatment as a risk factor for COPD: findings from a population-based survey of Canadian adults. Int J Chron Obstruct Pulmon Dis. 2016;11:2641-50. [ Links ]
20. Beran D, Zar HJ, Perrin C, Menezes AM, Burney P. Burden of asthma and chronic obstructive pulmonary disease and access to essential medicines in low-income and middle-income countries. Lancet Respir Med. 2015;3(2):159-70. [ Links ]
21. Gershon AS, Warner L, Cascagnette P, Victor JC, To T. Lifetime risk of developing chronic obstructive pulmonary disease: a longitudinal population study. Lancet. 2011;378(9795):991-6. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Ana Martins
E-mail: anainesvm@gmail.com
Conflict of interests
The authors declare they do not have any conflict of interests.
Recebido em 25-04-2019
Aceite para publicação em 19-06-2019
Supplementary file PRISMA 2009 Checklist