










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versión impresa ISSN 1646-706X
Angiol Cir Vasc vol.16 no.1 Lisboa mar. 2020
CASOS CLÍNICOS
The right way to catch a fish comes from the left
O caminho certo para apanhar um peixe vem da esquerda
Luís Loureiro1, Sérgio Teixeira1, Rui de Almeida1
1 Serviço de Angiologia e Cirurgia Vascular, Centro Hospitalar Universitário do Porto Porto, Portugal
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
The right aberrant subclavian artery, also known as arteria lusoria, is an anatomical variation described in the literature with an incidence of < 1%. Compression related symptoms can arise from the retroesophageal space and retrotracheal course of the artery. Only a few cases are reported of ischemic symptoms derived from a stenosed or occluded right aberrant subclavian artery. We present a case of ischemic right upper limb symptoms due to an occluded right aberrant subclavian artery treated with a hybrid procedure. The patient was submitted to a left subclavian artery stenting and left to right axillary bypass without complications.
Keywords: Arteria lusoria; Right aberrant subclavian artery; Hybrid surgery
RESUMO
A artéria subclávia aberrante direita, também conhecida como artéria lusória, é uma variação anatómica descrita na literatura com incidência < 1%. Os sintomas relacionados à compressão podem surgir por causa do trajeto retroesofágico e retrotraqueal da artéria. Apenas alguns casos são relatados de sintomas isquémicos derivados de uma artéria subclávia aberrante direita estenosada ou ocluída. Apresentamos um caso de sintomas isquémicos do membro superior direito devido a uma artéria subclávia aberrante direita ocluída tratada com cirurgia híbrida. O doente foi submetido a stenting da artéria subclávia esquerda e pontagem axilo-axilar esquerda / direita sem complicações.
Palavras-chave: Artéria lusória; Artéira subclávia direita aberrante; Cirurgia hibrida
Introduction
The right aberrant subclavian artery, also known as arteria lusoria, is an anatomical variation described in the literature with an incidence of < 1% (1). It was the first arch anomaly to be described in 1735 by Hunauld (2).
The right subclavian artery, normally, develops from the fusion of the right proximal dorsal aorta with the right seventh intersegmental artery distally. When the right proximal dorsal aorta and the right fourth vascular arch involutes and the seventh intersegmental artery persists originating from the proximal descending thoracic aorta the aberrant course of the subclavian artery is formed (3).
Most of the individuals with a right aberrant subclavian artery are asymptomatic. Compression related symptoms can arise from the retroesophageal space (dysphagia) and retrotracheal (dyspnea) course of the artery. Only a few cases are reported of ischemic symptoms derived from a stenosed or occluded right aberrant subclavian artery. Most patients were treated with right carotid to right subclavian bypass and some with endovascular angioplasty and stenting(4-8).
Case report
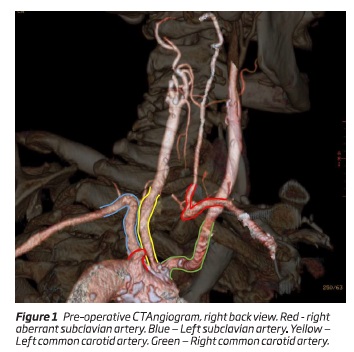
A 71-year old man presented with intermittent claudication of the right hand for 2 years. The symptoms appeared when he was fishing, activity that took most of his spare time and that he especially enjoyed. He had a previous history of peripheral arterial disease with an aorto-bi-femoral bypass 6 years before due to lower limbs rest pain and a stroke with complete recovery 2 months before. He was smoker for 40 years and diabetic for 12 years. An ischemic right coronary disease was present without indication for PCI or CABG. Radial pulses were present. Systolic pressures in the radial arteries measured by Doppler were asymmetric (right: < 35mmHg than left) and the right vertebral artery also had flow inversion in the Doppler ultrasound. CT angiogram showed a right aberrant subclavian artery occluded from the origin up to the retro-oesophagus (Figure 1). The left subclavian artery also had a 30% post-ostial stenosis. No stenosis was identified in the carotid arteries. The patient was on aspirin, ticagrelor, beta-blocker, statin and sitagliptin/metformin.
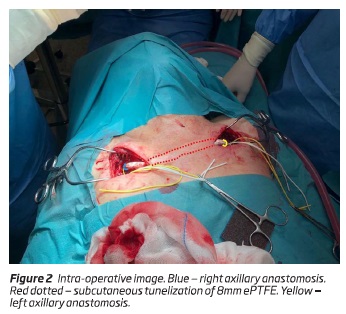
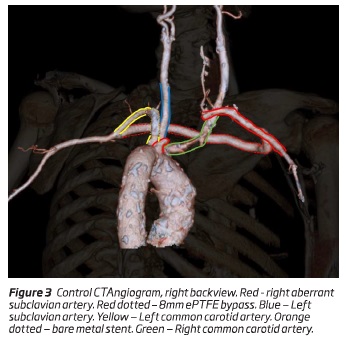
Open treatment was proposed, due to the risk of subclavian-esophageal fistula if stenting was performed. The patient declined the carotid transposition of the right subclavian due to the stroke risk from the carotid cross-clamping. Therefore a hybrid procedure was idealized. First an 8mm ePTFE bypass from the left to right axillary arteries was completed; in the same operative time a retrograde approach of the left subclavian stenosis through the ePTFE graft was performed (Figure 2) and a balloon mounted 7x29mm stent was implanted in the left subclavian artery resolving the stenosis. The procedure was uneventful, and the patient discharged in the third post-operative day. Two weeks after discharge he was fishing without any limitation. Four months later the control CTAngiogram presented patent left subclavian artery stent and axillo-axillary ePTFE bypass (Figure 3).
Discussion
Several groups have described symptomatic right aberrant subclavian artery revascularization by thoracotomy, median sternotomy and cervical approaches, using prosthetic bypass, interposition graft or transposition, with inflow from the common carotid or ascending aorta(6-11). While the open surgical treatments are more durable, they impose a higher surgical aggression on the patients. As our patient, due to the right coronary artery disease, some of them may not withstand a thoracotomy or median sternotomy.
Some other groups treated the ischemic symptoms with endovascular stenting of the stenosis or occlusion(4,5). These treatments may induce an arterial-esophagic fistula with catastrophic consequences.
Our patient recent history of stroke induced him a resistance to accept the unmeasurable stroke risk due to carotid cross-clamping. For this reason we were obliged to perform a hybrid surgery to treat his condition. For our knowledge this was the first left to right axillary bypass performed for the treatment of ischemic symptoms due to right aberrant subclavian artery occlusion.
REFERENCES
1. Recto, C., Boddi, M., Branca, J. J. V., Morucci, G., Pacini, A., Gulisano, M., Paternostro, F. Aortic arch branching pattern variation: its incidence on a 20030 cases review. IJAE, 124(1), 5-15 (2019). [ Links ]
2. Hunauld PM. Examen de quelques parties d’un singe. Hist Acad Roy Sci;2:516-23 (1735).
3. Popieluszko, P., Henry, B. M., Sanna, B., Hsieh, W. C., Saganiak, K., Pekala, P. A., Tomaszewski, K. A. A systematic review and meta-analysis of variations in branching patterns of the adult aortic arch. Journal of vascular surgery, 68(1), 298-306(2018). [ Links ]
4. Basile, A., Lomoschitz, F., Lammer, J. Transbrachial stenting of a critical ostial arteria lusoria stenosis. Journal of Endovascular Therapy, 10(4), 829-832(2003). [ Links ]
5. Machado, L., Rocha, A., Mansilha, A., Teixeira, J. Estenose sintomática da artéria subclávia direita aberrante. Angiologia e Cirurgia Vascular, 12(4), 275-278 (2016). [ Links ]
6. Rowe, D. M., Becker, G. J., Scott, J. A., Conces, D. J. Right subclavian steal associated with aberrant right subclavian artery. American journal of neuroradiology, 9(3), 604-606 (1988). [ Links ]
7. Roland, C. F., Cherry, K. J. Symptomatic atherosclerotic stenotic disease of an aberrant right subclavian artery. Annals of vascular surgery, 5(2), 196-198 (1991). [ Links ]
8. Kieffer, E., Bahnini, A., Koskas, F. Aberrant subclavian artery: surgical treatment in thirty-three adult patients. Journal of vascular surgery, 19(1), 100-111 (1994). [ Links ]
9. Stone, W. M., Ricotta II, J. J., Fowl, R. J., Garg, N., Bower, T. C., Money, S. R. Contemporary management of aberrant right subclavian arteries. Annals of vascular surgery, 25(4), 508-514 (2011). [ Links ]
10. Pifarre, R., Dieter, J. R., Niedballa, R. G. Definitive surgical treatment of the aberrant retroesophageal right subclavian artery in the adult. The Journal of thoracic and cardiovascular surgery, 61(1), 154-159 (1971). [ Links ]
11. Stone, W. M., Brewster, D. C., Moncure, A. C., Franklin, D. P., Cambria, R. P., Abbott, W. M. Aberrant right subclavian artery: varied presentations and management options. Journal of vascular surgery, 11(6), 812-817 (1990). [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Correio eletrónico: lploureiro@gmail.com (L. Loureiro).
Funding
No funding was received for this article.
Protection of people and animals
The authors state that for this research no experiments were performed on humans and / or animals.
Data Confidentiality
The authors state that no patient data appear in this article.
Right to privacy and written consent
The authors state that no patient data appear in this article.
Conflict of interests
The authors declare no conflict of interest.
Recebido a 13 de janeiro de 2020
Aceite a 16 de março de 2020

