










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versión impresa ISSN 1646-706X
Angiol Cir Vasc vol.15 no.4 Lisboa dic. 2019
ARTIGO ORIGINAL
Perioperative outcomes and long term survival after carotid endarterectomy in elderly patients
Resultados peri-operatórios e sobrevida a longo prazo após endarterectomia carotídea em doentes de idade avançada
Mário Moreira1, Vânia Constâncio1, Joana Silva1, Pedro Lima1, Mafalda Correia1, Luís Antunes1, Joana Moreira1, Manuel Fonseca1
1 Angiology and Vascular Surgery Department Centro Hospitalar e Universitário de Coimbra
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Stroke is a major health problem. Overall, 10-15% of all strokes are related to a previous asymptomatic carotid stenosis >50%. Carotid endarterectomy (CEA) is effective in stroke prevention; risk/benefit assessment is less apparent for elderly. The authors evaluate department CEA outcomes in elderly population aged 75 years and older, focusing in perioperative outcomes and long term survival.
Material and methods: Retrospective unicentric analysis was performed, encompassing 156 surgeries in 149 patients aged 75 years and older, between January 2010 and December 2017.
Results: Perioperative stroke/mortality was 2.6% (4.0% for symptomatic, 0% for asymptomatic); perioperative morbidity was 6.4%; estimated five-year survival was 71.9%.
Conclusion: CEA continues to be a low-risk approach to treat carotid bifurcation atherosclerosis, even in elderly population, with perioperative morbidity and mortality resembling international standards for general population. Long term survival is quite good and age alone should not be a reason to refrain from offering carotid endarterectomy to this patients.
Keywords: Carotid; Endarterectomy; Elderly
RESUMO
Introdução: O acidente vascular cerebral constitui um problema de saúde significativo. Globalmente, 10-15% de todos os acidentes vasculares cerebrais estão relacionados com uma estenose carotídea >50% previamente assintomática. A endarterectomia carotídea é eficaz na prevenção do acidente vascular cerebral; o risco/benefício é menos evidente em doentes idosos. Os autores avaliaram os resultados de endarterectomia carotídea do Serviço em doentes de idade igual ou superior a 75 anos, focando nos resultados peri-operatórios e na sobrevida a longo-prazo.
Material e métodos: Estudo retrospectivo, unicêntrico, englobando 156 cirurgias em 149 doentes de idade e75 anos, entre Janeiro de 2010 e Dezembro de 2017
Resultados: O acidente vascular cerebral/mortalidade peri-operatória foi de 2.6% (4.0% em sintomáticos, 0% em assintomáticos); a morbilidade peri-operatória foi de 6.4%; a sobrevida estimada a 5 anos foi de 71.9%.
Conclusão: A endarterectomia carotídea é uma abordagem de baixo risco no tratamento da aterosclerose da bifurcação carotídea, mesmo em doentes de idade avançada, com morbilidade e mortalidade perioperatória comparável com os padrões internacionais para a população em geral. A sobrevida a longo prazo é bastante boa e a idade per se não deve ser impeditivo da realização de endarterectomia carotídea nestes doentes.
Palavras-chave: Carotídea; Endarterectomia; Idoso
Introduction
Stroke is a major health problem. Overall, 10-15% of all strokes are related to a previous asymptomatic carotid stenosis >50%. Carotid endarterectomy (CEA) is effective in stroke prevention. Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS) released in 2017 recommend carotid endarterectomy for symptomatic carotid stenosis e50%; regarding asymptomatic patients, carotid stenosis e60% can be an indication for carotid endarterectomy in average surgical risk patients with at least 5-year life expectancy(1). Risk/benefit assessment is less apparent for elderly and women.
Advanced age has been a controversial topic in the management of atherosclerotic carotid disease; regarding asymptomatic patients, advanced age was an exclusion criteria for some randomised trials. Twenty percent (n=650) of patients from Asymptomatic Carotid Surgery Trial 1 (ACST-1)(2) had more than 75 years of age; this subgroup analysis showed reduced benefit from CEA compared to younger patients, considering higher perioperative risk and reduced stroke risk on medical therapy. Five year survival for this subgroup was about 50%.
On the other hand, pooled data analysis(3) from trials on symptomatic patients showed greatest risk reduction in ipsilateral stroke conferred by CEA in patients aged 75 years and older. Another meta analysis(4) found little effect of age on CEA periprocedural risk.
Life expectancy continues to increase over the last decades; Portuguese population(5) life expectancy at birth is 81 years (Male:78; Female:83); moreover, life expectancy at age 65 is 19 years (Male:83, Female:86). Decision about performing CEA can be challenging in this aging population.
Therefore, the authors intend to evaluate department CEA outcomes in elderly population, focusing in perioperative morbidity and mortality and long term survival.
Material and Methods
Retrospective unicentric analysis encompassing CEA performed in patients aged 75 years and older, between January 2010 and December 2017. Demographic and clinical data were collected; outcomes were perioperative morbidity and stroke/mortality as well as long term survival. Age was stratified in two subgroups: 75-79 and e80 years and tested in cross tabulation with chi-square test like gender and symptom status for the outcomes perioperative morbidity and stroke/mortality. Survival analysis was performed using logrank test for gender, stratified age and number of studied comorbidities. Carotid stenosis was obtained from preoperative CT angiogram or carotid Doppler ultrasound using North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria. Transcranial cerebral oximetry was used for intraoperative neurologic monitoring.
All statistical analyses were performed with the SPSS 20.0 statistical software package. Statistical significance was inferred for p < 0.05.
Results
We performed 156 surgeries in 149 patients aged 75 years and older, representing 32.4% of carotid endarterectomies performed in our centre in the studied period. Demographic and clinical variables are summarized in Table I.
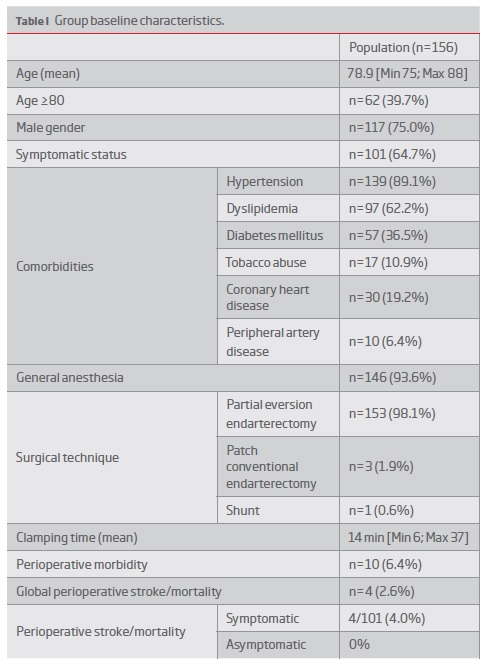
Perioperative morbidity and stroke/mortality are detailed in Table II.
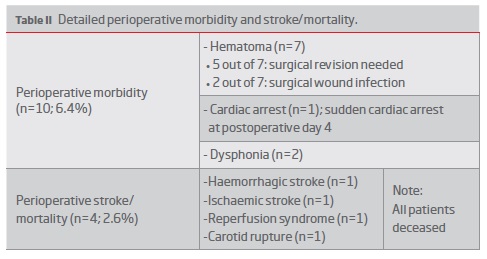
Regarding perioperative morbidity, statistical significant association with gender (male vs female; p=1), age (75-79 vs e80; p=0.64) and symptom status (symptomatic vs asymptomatic; p=0.74) were not found.
Concerning perioperative stroke/mortality analysis, results are as follows: gender (male vs female; p=0.05), age (75-79 vs e80; p=0.65) and symptom status (symptomatic vs asymptomatic; p=0.30).
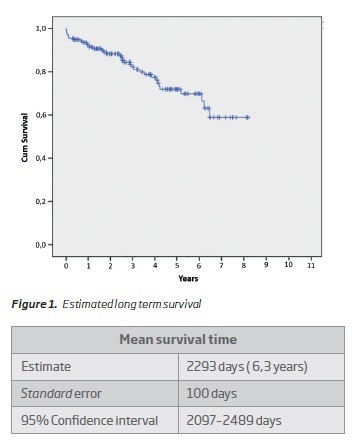
Estimated 5-year survival (Figure 1) was 71.9% (standard error - 0.046) and not associated with gender (p=0.59), age (p=0.14) and number of studied comorbidities (p=0.50).
Discussion
Elderly patients represent a significant portion of clinical practice concerning management of atherosclerotic carotid stenosis. CEA proved safe for this population aged 75 and older with perioperative stroke/mortality within international standards.
Population size as well as low perioperative morbidity and stroke/mortality may hinder some statistical analysis regarding outcomes and studied variables and maybe justify absence of significant associations. It is possible that low event rate reflect case selection in favour of less frail patients.
However, analysis using age grouping (75-79 vs e80) showed no significant difference on perioperative morbidity and stroke/mortality. Similar results were reported in recent studies(6). Gender also did not show to influence perioperative outcomes, despite some propensity for higher mortality in female patients; this finding has been confirmed in multiple large studies. Concerning symptom status, no association was found to perioperative outcomes; this surprised the authors as all deaths were symptomatic patients. Yet, sample size and zero deaths in asymptomatic patients may lead to this.
In our centre, carotid endarterectomy is performed by partial/modified eversion as first option. Still more widely used patched and eversion techniques, recent reports on partial/modified eversion are encouraging(7). Despite issues on previous papers related to late restenosis, reduced clamping and operating times in this elderly patients with impaired cerebrovascular reserve must be brought to discussion.
Long term survival warrant particular attention in this population to ensure this patients live long enough to benefit from intervention. Our group estimated 5-year survival was 71.9%; despite inferior to global survival after CEA, still an excellent survival considering population under analysis(8). Age (75-79 vs e80), gender and presence of great number of studied comorbidities did not show to affect survival.
About one third of patients underwent CEA for an asymptomatic carotid stenosis; it must be taken in account that guideline recommendations in the studied time interval were more broad-minded regarding these patients. Despite no perioperative stroke/mortality in our group, current recommendations state that only selected asymptomatic patients may benefit from carotid revascularization.
Considering several data showing improvement in CEA outcomes in elderly population as well as increased life expectancy, it seems relevant to have new randomized trials evaluating atherosclerotic carotid disease outcomes across the age spectrum.
Conclusions
CEA continues to be a low-risk approach to treat carotid bifurcation atherosclerosis, even in elderly population, with perioperative morbidity and mortality resembling international standards for general population.
Long term survival is quite good and age alone should not be a reason to refrain from offering carotid endarterectomy to this patients.
REFERENCES
1. Naylor AR, Ricco JB, de Borst GJ, Debus S, de Haro J, Halliday A, et al. Management of Atherosclerotic Carotid and Vertebral Artery Disease: 2017 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018; 55:3-81. [ Links ]
2. Halliday A, Harrison M, Hayter E, Kong X, Mansfield A, Marro J, et al. 10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1): a multicentre randomised trial. Lancet 2010; 376:1074-84. [ Links ]
3. Rothwell PM, Eliasziw M, Gutnikov SA, Fox AJ, Taylor DW, Mayberg MR, et al. Carotid Endarterectomy Trialists Collaboration. Endarterectomy for symptomatic carotid stenosis in relation to clinical subgroups and timing of surgery. Lancet 2004; 363:915-24. [ Links ]
4. Howard G, Roubin GS, Jansen J, Halliday A, Fraedrich G, Eckstein H-H, et al. Association between age and risk of stroke or death from carotid endarterectomy and carotid stenting: a meta-analysis of pooled patient data from four randomised trials. Lancet 2016; 387:1305-11. [ Links ]
5. Data from PORDATA, www.pordata.pt. [ Links ]
6. Pasin L, Marrocco-Trischitta MM, Landoni G, Piras D, Nardelli P, Cornero G, et al. Operative morbidity and mortality in octogenarians after carotid endarterectomy: a propensity score matching study. J Cardiovasc Surg 2016; [Epub] [ Links ]
7. Musicant SE, Guzzetta VJ, Terramani TT, Greenwood KL, Chiodo WC, Heaney KM, et al. Modified Eversion Carotid Endarterectomy (mECEA): Analysis of Clinical and Financial Outcomes. Ann Vasc Surg 2017; 42:16-24. [ Links ]
8. Pol RA, Reijnen MPJ, Lont M, Tielliu IFJ, van Sterkenburg SMM, van den Dungen JJAM, et al. Safety and Efficacy of Carotid Endarterectomy in Octogenarians. Ann Vasc Surg 2013; 27:736-742. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Correio eletrónico: mariodpmoreira@gmail.com (M. Moreira).
Recebido a 13 de agosto de 2019
Aceite a 03 de dezembro de 2019

