










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkAngiologia e Cirurgia Vascular
Print version ISSN 1646-706X
Angiol Cir Vasc vol.15 no.3 Lisboa Sept. 2019
CASOS CLÍNICOS
Superficial Femoral Artery Aneurysmal Degeneration - Sixteen years after superficial femoral artery endarterectomy and vein patch angioplasty
Degenerescência aneurismática da artéria femoral superficial - Dezasseis anos após endarterectomia da artéria femoral superficial e encerramento com patch de veia grande safena
Gabriela Teixeira1, Joana Martins1, Arlindo Matos1, Inês Antunes1, Carlos Veiga1, Daniel Mendes1, Carlos Veterano1, Henrique Rocha1, João Castro1, Rui Almeida1
1 Angiology and Vascular Surgery Department, Centro Hospitalar Universitário do Porto, Oporto, Portugal
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Superficial femoral artery (SFA) aneurysms are rare clinical disorders, with few case reports and small series published concerning atherosclerotic aneurysms. We report a clinical case a giant aneurysm of the SFA, in a patient previously submitted to extensive SFA endarterectomy and vein angioplasty.
A 73-year-old man presented at a routine vascular surgery consultation. The patient had been submitted to a right SFA endartectomy and vein patch angioplasty, sixteen years ago, for intermittent claudication. Physical examination demonstrated a large pulsatile mass of the right thigh. His right pedal pulse was palpable. Ultrasound and computed tomography scan confirmed a 78x71x240mm aneurysm of the right superficial femoral artery.
He was proposed to aneurysmectomy and femoro-popliteal bypass. During operative intervention, proximal and distal control was obtained and the aneurysm opened. A large amount of thrombus was removed and a femoro-popliteal bypass was performed using the ipsilateral great saphenous vein. The postoperative period was uneventful, as was the patient recovery.
In our report, the aneurysmal area matched precisely to the endarterectomised area and no other aneurysms were found. So we are facing an uncommon case of a SFA degeneration into a giant aneurysm after extensive endarterectomy and vein angioplasty.
Keywords: Superficial femoral artery aneurysm; Vein aneurysmal degeneration; Superficial femoral artery endarterectomy
RESUMO
Os aneurismas da artéria femoral superficial (AFS) são entidades clínicas raras, com poucos casos clínicos e pequenas séries publicadas, normalmente relativas a aneurismas de etiologia aterosclerótica. Nós reportamos o caso clínico de degenerescência aneurismática da artéria femoral superficial, num doente previamente submetido a endarterectomia da AFS e encerramento com patch de veia grande safena.
Um homem de 73 anos apresentou-se numa consulta de rotina de cirurgia vascular. O paciente tinha sido submetido a endarterectomia da AFS e angioplastia com patch de veia, dezasseis anos atrás, por claudicação intermitente. Ao exame físico, o doente apresentava uma massa pulsátil na coxa direita. O pulso pedioso era palpável e amplo. O ecodoppler e AngioTC confirmaram o diagnóstico de aneurisma da AFS com 78x71x240mm.
O doente foi proposto para aneurismectomia e pontagem femoro-poplítea. Durante o procedimento, foi realizado o controlo proximal e distal da AFS, e o aneurisma foi aberto. Após remoção de quantidade considerável de trombo, foi realizado uma pontagem femoro-poplítea inlay, com recurso à veia grande safena ipsilateral.
No caso descrito, a zona aneurismática coincidia precisamente com a extensão de AFS endarterectomizada e nenhum outro aneurisma foi detectado. Este é um caso incomum de degenerescência aneurismática da AFS após endarterectomia e angioplastia com patch de veia.
Palavras-chave: Aneurisma da artéria femoral superficial; Degeneração aneurismática de veia; Endarterectomia da artéria femoral superficial
Introduction
Superficial femoral artery (SFA) aneurysms are rare clinical disorders, with few case reports and small series published concerning atherosclerotic aneurysms. We report a clinical case of a giant aneurysm of the SFA, in a patient previously submitted to extensive SFA endarterectomy and vein angioplasty.
Case Report
A 73-year-old man with a past medical history of diabetes, atrial fibrillation, dislipidemia and prostatic neoplasm presented at a routine vascular surgery appointment. The patient had been submitted to an extensive right SFA endartectomy and a vein patch angioplasty with ipsilateral great saphenous vein (GSV), sixteen years before, for intermittent claudication. There was no familiar history of aneurysms. His pertinent medications included acenocoumarol and statin. The physical examination demonstrated a large pulsatile mass of the right thigh (Figure 1). His right pedal pulse was palpable, but posterior tibial pulse was absent. Contralateral signs of peripheral arterial disease, with absent popliteal and distal pulses, were observed. The duplex ultrasound examination and the computed tomography angiography scan (angioCT) confirmed a SFA aneurysm of 78x71x240mm size (Figure 2). Other aneurysms were excluded.


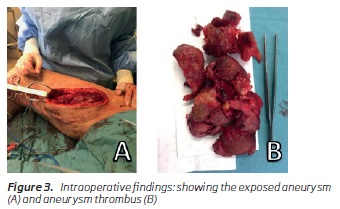
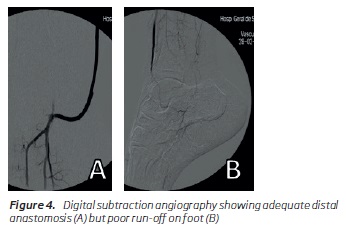
The patient was proposed to aneurysmectomy and femoro-popliteal bypass. Vein mapping showed a non-expected GSV in the thigh suitable for bypass (patient had been submitted to angioplasty of the SFA with thigh’s GSV sixteen years ago - as there was no incisions of vein harvesting in the leg or contralateral limb - so we presume patient must had a GSV duplication). During operative intervention, proximal and distal control of the SFA was obtained. After systemic heparinization with 5000 units of unfractionated heparin, proximal and distal SFA were clamped and the aneurysm was opened. A large amount of thrombus was removed (Figure 3). A femoro-popliteal bypass was performed using the reversed ipsilateral GSV. The proximal anastomosis was done to the proximal disease-free SFA segment. The proximal popliteal artery was not suitable to distal landing, because the disease-free popliteal artery was too deep into the popliteal fossa. The GSV was subcutaneously tunneled and the distal portion of popliteal artery was used for the distal anastomosis. Final angiographic control showed adequate distal anastomosis, but poor foot run-off (Figure 4). A distal anterior tibial artery embolectomy was performed with 2and 3-Fr Fogarty with recovery of a small amount of thrombus and good back-flow. After artery closure the foot was well perfused and pedal pulse was palpable. The patient was kept under anticoagulation with unfractionated heparin perfusion, and then switched to enoxaparin at postoperative day 3. The postoperative period was uneventful, as was the patient recovery. Patient was discharged at postoperative day 7 under enoxaparin and acenocoumarol overlapping until the INR was within therapeutic range. At one-month follow-up, he was ambulating without claudication, with palpable right pedal pulse and an ankle-brachial pressure index above 1.
Discussion
Superficial femoral artery (SFA) aneurysms are rare clinical entities, with few case reports and small series published, usually concerning atherosclerotic aneurysms(1). We report a clinical case of an aneurysm of the SFA, in a patient previously submitted to SFA endarterectomy and vein angioplasty.
There are some published cases reporting aneurysmal degeneration of GSV as a bypass conduit(2,3). Atherosclerosis was the most commonly identified histopathologic finding on examination of the excised aneurysm wall, and aneurysmal degeneration of vein grafts were far more common in patients with a history of aneurysmal disease.
In our report, the aneurysmatic area matched precisely to the endarterectomised area, no other aneurysms were found and there was no known familiar history of aneurysms.
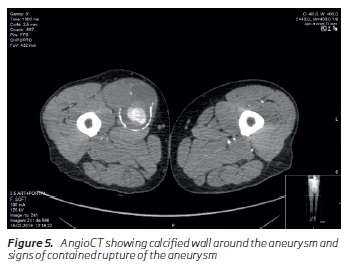
Intraoperatively, and in the angioCT (Figure 5), we found a calcified wall around the aneurysm and signs of a contained rupture. Unfortunately, no histopathological exam was performed.
We found a case report of SFA aneurysmal degeneration after remote endarterectomy with the Mollring device(4). This was a less invasive femoropopliteal revascularization, that demanded closed surveillance for the high risk of stenosis, but there was no data published before about SFA aneurysmal degeneration. In the case reported by Cameron, the procedure complicated with a 2.3 cm SFA aneurysm. Its pathogenesis remains speculative.
Surgical treatment methods for SFA aneurysms include aneurysmal excision with graft interposition or vein bypass, endovascular exclusion and ligation of the aneurysm sac. Our option for femoropopliteal bypass with endoaneurismoraphy was a good choice. It is possible that some embolization to pedal artery occurred, but it was promptly corrected with distal embolectomy. The idea of endovascular exclusion was abandoned because of the aneurysm size, which was too large to be left in place, despite no compression symptoms were expressed by the patient. Despite this invasive and extensive operative procedure, our patient made a favourable functional recovery, and graft patency was maintained.
Superficial femoral artery aneurysms are a rare but potentially fatal vascular disease. This is a rare report of a SFA degeneration into a giant aneurysm after extensive endarterectomy. We highlighted the stepwise approach to clinical evaluation, diagnosis, and surgical management of this entity.
REFERENCES
1. Jarrett F, Makaroun MS, Rhee RY, Bertges DJ. Superficial femoral arteryaneurysms: an unusual entity? J Vasc Surg. 2002 Sep;36(3):571-4. [ Links ]
2. Tao MJ, Al-Jundi W, Roche-Nagle G. Aneurysmal degeneration of vein conduit used for vascular reconstruction-Case report and literature review. Int J Surg Case Rep. 2016;28:289-292. [ Links ]
3. Cassina PC, Hailemariam S, Schmid RA, Hauser M. Infrainguinal aneurysm formation in arterialized autologous saphenous vein grafts. J Vasc Surg. 1998 Nov;28(5):944-8. [ Links ]
4. Cameron DB, Black JH 3rd, Fishman EK, Freischlag JA, Abularrage CJ. Aneurysmal degeneration of the superficial femoral artery after remote endarterectomy. J Vasc Surg. 2012 Apr;55(4):1153-5. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Correio eletrónico: Tgabrielateixeira@gmail.com (G. Teixeira).
Protection of human subjects and animals in research: The authors declare that no experiments were performed on humans or animals for this investigation.
Patients’ data protection: The authors declare that no patient data appears in this article.
Right to privacy and informed consent: The authors declare that no patient data appears in this article.
Recebido a 31 de julho de 2019
Aceite a 13 de setembro de 2019

