










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.14 no.4 Lisboa dez. 2018
ARTIGO ORIGINAL
Neuroischemic diabetic foot - the endorevolution
Pé diabético neuroisquémico - a revolução endovascular
Rita Augusto*1,2, Ricardo Gouveia1, João Vasconcelos3, Jacinta Campos1,2, Pedro Sousa1, Andreia Coelho1,2, Nuno Coelho1,2, Ana Semião1, Evelise Pinto1, João Ribeiro1, Daniel Brandão1,2, Alexandra Canedo1,2
1Serviço de Angiologia e Cirurgia Vascular, Centro Hospitalar de Vila Nova de Gaia/Espinho, Vila Nova de Gaia, Portugal
2Unidade de Angiologia e Cirurgia Vascular da Faculdade de Medicina da Universidade do Porto, Porto, Portugal
3Serviço de Angiologia e Cirurgia Vascular, Centro Hospitalar de Tâmega e Sousa, Penafiel, Portugal
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Currently, the prevalence of Diabetes Mellitus (DM) in Portugal is 13,3% in adult population. Patients with DM have a 15-25% lifetime risk of developing a foot ulcer. Additionally, diabetic angiopathy is a unique vascular disease that has predilection for below-the-knee arteries. Meanwhile, endovascular techniques have been revolutionizing the revascularization of neuroischemic diabetic foot (NIDF) patients, showing consistently higher limb salvage rates.
The survival of NIDF patients reaches 50% at 5 years after revascularization and limb salvage, but decreases to 50% at 2 years after a major amputation. With this study, the authors intend to describe their experience on endovascular revascularization for the treatment of NIDF patients.
Methods: Retrospective institutional review of consecutive patients requiring endodistal revascularization (January 2010 December 2017) - 464 limbs in 326 patients.
We evaluated demographics and co-morbidities data and performed statistic analysis to determine factors and outcomes as limb salvage, major and minor amputation rates. The primary outcome was to evaluate the technical success, the limb salvage, the rate of major and minor amputation and the global survival of this population. The secondary outcomes were to characterize the population, the endovascular procedures performed and the evolution over the last years. Operative reports were reviewed to analyze the endovascular procedures and techniques.
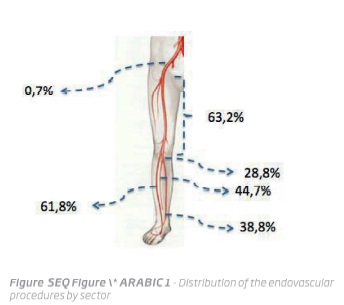
Results and conclusions: The technical success was achieved in 85% of the procedures. The iliac sector was only treated in 0,7% of the procedures and femoro-popliteal sector in 63,2%. Antegrade femoral approach, was obtained in 91, 3% of the procedures. A complementary retrograde distal approach was performed in 7,6% of procedures. Direct angiossomic revascularization was obtained in 60,9% of the cases. In the femoral and popliteal arteries, PTA was performed in 56,3% of the procedures and recanalization, PTA and stenting in 42,4%. During FU, 14,1% of patients was submitted to major amputation and 36,4% to minor amputation. The major amputation free-survival rate was 80,1% at 12 mo and the rate of healing at 12 mo was 63,2%. The 12 mo global survival was 79,8%. Direct angiossomic revascularization (p=0,014) and the number of tibial arteries recanalized (p=0,01) were both associated with a higher limb salvage rate and a faster healing of the ulcer. In the opposite side, there was an association between the increasing of renal dysfunction and poor healing (p=0,04). The endovascular reintervention rate was 20,4%. The results of the author’s study on endodistal revascularization, highlights the need to prioritize investigation and revascularization in NIDF patients to improve the outcome of foot ulcer, giving the possibility of salvaging a greater number of limbs.
Keywords: Diabetic Foot; Endovascular procedures; Stent; Angioplasty; Limb salvage; Amputation
RESUMO
Introdução: A prevalência estimada de Diabetes Mellitus (DM) em Portugal é de 13,3% na população adulta. Ao longo da sua vida cerca de 15-25% dos diabéticos desenvolvem úlcera no membro inferior. A DM é uma doença vascular única que facilita a infeção e tem predileção para o atingimento de artérias abaixo do joelho. Neste contexto, a revascularização por técnicas endovasculares dos doentes com pé diabético neuroisquémico (PDNI) é hoje considerada, pela maioria dos autores, como de primeira linha, mostrando consistentemente maiores taxas de salvamento de membro.
Estima-se que a mortalidade dos doentes com PDNI atinja os 50% aos 5 anos (após revascularização, com viabilidade do membro mantida), aumentando para 50% aos 2 anos sem revascularização e consequente amputação major. Com este estudo, os autores pretendem descrever a sua experiência na revascularização distal endovascular no tratamento de doentes com PDNI.
Métodos: Estudo restrospectivo que inclui todos os doentes diabéticos submetidos a revascularização endovascular de artérias distais (janeiro 2010 - dezembro 2017) - 464 membros em 326 doentes.
Foram avaliados os dados demográficos, co-morbilidades e processos clínicos. O objetivo primário é avaliar o sucesso técnico, a taxa de salvamento de membro assim como as taxas de amputação major e amputação minor. Como objetivos secundários os autores pretendem descrever a população tratada, os tratamentos endovasculares efetuados assim como caraterizar a evolução adquirida nos últimos anos nestas técnicas.
Resultados e conclusões: O sucesso técnico foi alcançado em 85% dos procedimentos. Foi necessária revascularização concomitante do setor ilíaco em 0,7% e do setor femoro-poplíteo em 63,2% dos casos. O acesso femoral anterógrado foi obtido em 91,3% dos casos. Foi necessária punção distal retrógrada em 7,6% dos procedimentos. A revascularização angiossómica foi obtida em 60,9% dos casos. No setor femoro-poplíteo, foi efetuada ATP em 56,3% dos procedimentos e recanalização, ATP e stenting em 42,4%. Durante o follow-up, 14,1% dos doentes foi submetido a amputação major e 36,4% a amputação minor. A sobrevida livre de amputação major aos 12 meses foi de 80,1% e a taxa de cicatrização aos 12 meses de 63,2%. A sobrevida global aos 12 meses foi de 79,8%. Encontrou-se associação entre a revascularização angiossómica (p=0,014) e o número de eixos distais permeáveis (p=0,01) com a presença de salvamento de membro e a diminuição no tempo até à cicatrização. Encontrou-se adicionalmente associação entre o estadio de disfunção renal e a ausência de cicatrização (p=0,04). A taxa de reintervenção foi de 20,4%. Os resultados do presente estudo sobre a revascularização endovascular de eixos distais em doentes diabéticos enfatiza a necessidade de um investimento apropriado nesta população, aumentando o sucesso na revascularização possibilitando a preservação de um maior número de membros.
Palavras-chave: Pé Diabético; Revascularização endovascular; Stent; Angioplastia; Salvamento de membro; Amputação
Introduction
By 2030 it is estimated that there will be 439 million people in the world living with Diabetes Mellitus (DM).(1) Presently, the prevalence of DM in Portugal is 13,3% in adult population.(2)
The annual incidence of foot ulceration is estimated to be approximately 1%-4%, and its prevalence ranges from 4% to 10%, whereas, the lifetime risk for the development of a diabetic foot ulcer in patients with diabetes ranges from 15% to as high as 25% - in case of neuropathy with peripheral artery disease (PAD).(3,4) PAD is an independent risk factor for subsequent ulceration and limb loss.(5) The prevalence of PAD is high in diabetic patients and can be found in up to 50% of cases with lower limb lesions.(6) More recently, some studies had reported up to 75% of PAD in diabetic patients.(7)
Neuroischemic diabetic foot (NIDF) generally affects patients with long duration of the disease that may also be particularly fragile and difficult to manage clinically. The high rate of co-morbidities in these patients (especially cardiovascular) means that the attention should not be exclusively focused on the foot with an ulcer, but should take into account the patient as a whole - diabetic foot is a local manifestation of a systemic condition.(5)
Diabetic angiopathy is an unique vascular disease that has a predilection for below-the-knee arteries.(8) The negative prognosis of ischemic lesions in diabetic patients is probably related to the co-existence of factors such as the anatomical distribution and severity of PAD, infection, neuropathy, renal disease and the concomitant presence of other coronary and cerebral vascular manifestations. Some studies comparing diabetic and non-diabetic patients, verified that interventions to revascularize the lower limb on diabetic have poorer results: lower technical success and worse patency rates - both in endovascular and open surgery.(9,10) Focusing only on diabetic patients, according to Hinchliffe et al.(11), the currently available literature suggests that there is no difference in clinical outcomes for patients treated with endovascular or surgical revascularization, with existing data being insufficient to recommend one method over another.
The most severe complication of NIDF is the need of limb amputation. Besides dramatically affecting functional status, amputation of a limb significantly increases the risk of death compared to surgical bypass or endovascular revascularization.(12) The prognosis of NIDF is severe since 30%-50% may require a major amputation and up to 20% die of cardiovascular disease within 1-year.(13)
The survival of neuroischemic diabetic foot patients reaches 80% at 2 years and 50% at 5 years after revascularization and limb salvage, but decreases to 50% at 2 years after a major amputation.(14)
In the last decade, endovascular techniques have been revolutionizing the revascularization of neuroischemic diabetic foot patients.(5)
Several studies have evaluated the role of percutaneous transluminal angioplasty (PTA) in NIDF, especially in infra-popliteal vessels disease. The overall results are favorable in terms of feasibility, technical efficacy, reduction number of complications and limb salvage rates.(15-21)
Although long-term patency is better after bypass surgery than after angioplasty, the last one can also be proposed for patients who cannot be candidates for a bypass because of significant co-morbidities, a reduced life expectancy, infection or gangrene in the possible sites of distal anastomoses, the unavailability of suitable veins or the absence of an adequate ‘landing zone’ for the distal part of the bypass.(15-17,22) Additionally, for critical limb ischemia, the goals of treatment are relieving ischemic pain, healing ulcers, preventing limb loss, improving patient function and quality of life, and prolonging survival, even if the middle and long-term patency of the arteries submitted to endovascular angioplasty could be worse.
Accordingly, with this study, the authors intend to describe the experience of their Vascular Surgery Department on endovascular revascularization for the treatment of NIDF patients.
Methods
Retrospective institutional review of consecutive patients requiring endodistal revascularization performed by vascular surgeons (January 2010 - December 2017). We evaluated demographics and co-morbidities data and performed statistic analysis to determine factors and outcomes as limb salvage, major and minor amputation rates. Major amputation was defined as amputation proximal to the ankle joint whilst minor amputation was defined as amputation distal to the ankle joint. The primary outcome was to evaluate the technical success, the limb salvage, the rate of major and minor amputation and the global survival of this population. The secondary outcomes were to characterize our population, the endovascular procedures performed and the evolution over the last years. Operative reports were also reviewed to analyze the endovascular procedures and techniques.
Categorical variables are presented as frequencies and percentages and continuous variables as means and standard deviations, or medians and interquartile ranges for variables with skewed distribution. Normal distribution was checked using Kolmogorov Smirnov test or skewness and kurtosis. All reported P values are two-tailed, with P value of 0,05 indicating statistical significance. Analyses were performed with the use of SPSS software, version 22.
Results
This study included 326 patients, which corresponded to 464 limbs. Only endodistal revascularizations in limbs without surgical bypass were included.
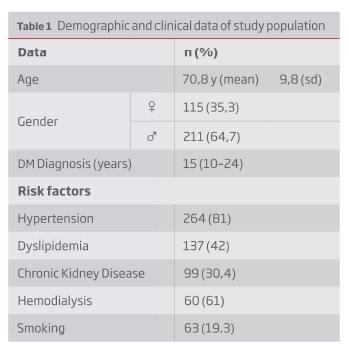
The mean age population was 70,8 years old (yo); 64,7% were men, with a mean time of diagnosed diabetes of 15 years (10-24). The comorbidities presented were hypertension (81%), hypercholesterolemia (30,4%), chronic kidney disease (30,4%; on hemodialysis: 57,6%) and smoking (19,3%) - Table 1. Isolated rest pain with no ulcer was present in only 4,1% of the patients.
The iliac sector was concomitantly treated in just 0,7% of the procedures and femoro-popliteal sector in 63,2%. Figure 1 presents the distribution of the endovascular procedures according the sector that suffered revascularization.
Femoral antegrade approach was always attempted and was obtained in 91,3% of the procedures and the others were obtained by retrograde femoral approach. The retrograde distal approach was made when the anterograde revascularization failed to cross the occlusion, and usually according to the angiosome concept (7,6% of procedures). The technical success - crossing the lesion, recanalizing the vessel and reaching adequate foot run-off at least in one artery - was achieved in 85% of the procedures.
Direct angiossomic revascularization was obtained in 60,9% of the cases.
In the femoro-popliteal sector, PTA was performed in 56,3% of the procedures, 1,3% with drug eluting balloon - DEB, and recanalization, PTA and stenting in 42,4%. Tibial arteries stenting was performed in 1,9% of procedures, as a bail-out technique, with drug eluting stent (DES) over a 0,014 guide wire plataform.
The median follow-up (FU) time was 11 months (mo), with an interquartile range of 16 mo. During FU, 14,1% of patients was submitted to major amputation and 36,4% to minor amputation.
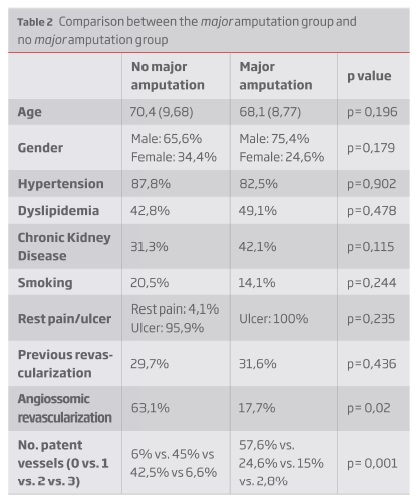
In Table 2, the authors present the data comparing the group of patients who suffered amputation and the group with limb salvage, both after revascularization. There were no significant differences between the two groups regarding some criteria, such as cardiovascular risk factors, age or previous endovascular intervention. In the opposite way, there were association between angiossomic revascularization (p=0,014) and the number of tibial arteries recanalized (p=0,01) with the presence of limb salvage and the faster healing of the ulcer.
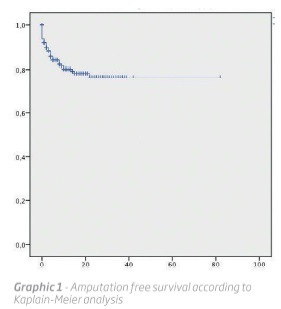
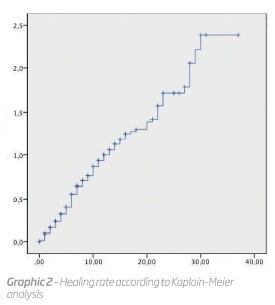
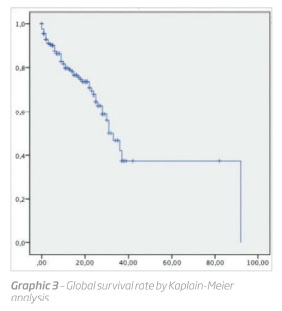
The major amputation free-survival rate was 80,1% at 12 mo (graphic 1) and the rate of healing at 12 mo was 63,2% (graphic 2). The 12 mo global survival was 79,8% (graphic 3).
The endovascular reintervention rate was 20,4% and the median time was 205 days after the first procedure. The technical success achieved in reinterventions was 90,2 and major amputation was required in 13,4% of these patients. Balloon angioplasty (POBA) was the most common modality used for reintervention - 84,5% of cases. In 12.6% there was deployment of stents and in the minority of cases - 2,9% - there was used DEB. Each patient of this group needed approximately 1,5 endovascular procedures after the first one.
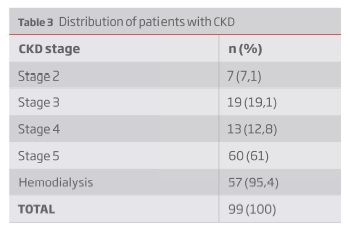
Considering the subgroup of patients with chronic kidney disease (CKD), 57,6% of the population was in hemodialysis program. The distribution of the different stages of CKD is presented in Table 3. According to the author’s data, considering only patients with CKD, there were no association between the stage of CKD and the increasing of the mortality (p=0,13) and major amputation (p=0,844). On the opposite side, we verified that the increasing of renal dysfunction was associated with the absence of ulcer healing (p=0,04). There were no significant statistic differences between the group of patients in hemodialysis and the group of patients in CKD stage 5 with no renal replacement therapy.
Comparing the group of patients with CKD and the group with normal renal function, the authors found significant statistic differences related with mortality rate, with the patients with CKD having more mortality (p=0,01). No significant statistic differences were found concerning the major amputation rate (p=0,130) between these two groups.
The global mortality rate in the present study regarding the patients with CKD was 26,8% and the major amputation free-survival rate at 12 mo was 75,9%, demonstrating the complexity of arterial disease of these patients and the challenge presented to vascular surgeons to promote the limb salvage.
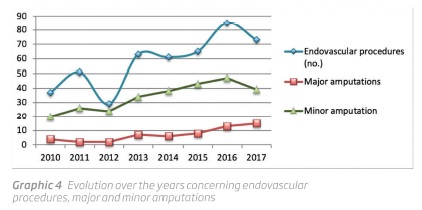
Between 2010 and 2017 the authors verified in the population of NIDF who were submitted to endovascular revascularization, the increasing of endovascular procedures as the minor amputation and the declining of major amputations (Graphic 4).
They performed a division of the population into 2 groups: group A - endovascular revascularizations between 2010 - 2014 and group B between 2015 - 2017. The authors verified some interesting conclusions that reflect the progress and work over the last years. Despite of the first group including more years, they verified very similar numbers on endovascular revascularizations - group A: 241 procedures and group B: 223 procedures. Over the last years these population have comparable characteristics but it was verified more patients with CKD in group B (63 vs. 86). One of the most interesting aspect that the authors highlight is the crescent use of other techniques - as retrograde approaches - for the last years - group A: 7 and group B: 25 - reflecting more aggressive alternatives to achieve limb salvage - a point that revealed a statistic difference between the two groups (p=0,001). The technical success in group A is similar to group B (171 vs. 183) and both groups are similar concerning the healing rate. The authors verified over the years the increase of endovascular procedures, followed by a bigger number of minor amputation surgeries. The results additionally show that the Center have invested in more complex patients, with more comorbidities and consequently the group B have a major mortality comparing to the other group.
Discussão
Several different techniques are available for revascularization in NIDF: infrainguinal bypass and endovascular techniques, which have evolved greatly over the past few years - additionally with recent use of DEBs and coated stents. Nowadays, infrapopliteal endovascular revascularization constitute a first line treatment for BTK arterial occlusive disease, since they promote a high limb salvage rates and a low morbidity and mortality.(23)
Taylor and Palmer first described the angiosome concept, in which human tissue is delineated into blocks according to how they are fed by specific arterial and venous sources.(24)
Regarding this concept, it has further increased the success rate and major amputation-free survival of the endovascular interventions. According to this principle, the ankle and foot are divided into six distinct three-dimensional vascular territories supplied by the posterior tibial artery, the anterior tibial artery or the peroneal artery. Some authors report that in patients with ischemic wounds, direct revascularization of the source artery seems more effective than revascularization of a nonspecific artery with reliance on collateral arteries. Other studies documented that clinical outcome of the foot has been demonstrated to be favorably affected by increasing numbers of patients crural arteries at the end of the endovascular treatment. However, all of these results rely on retrospective data.(23)
Angiossomic revascularization is not always feasible and it is imprecisely defined between institutions.
It appears that this technique results in approximately a 10-15% increase in wound healing rates relative to non-angiossomic revascularization.(25) In this study, angiossomic revascularization was associated with the presence of limb salvage and the faster healing of the ulcer.
One further aspect that needs to be considered is the patient’s general condition. The most important of the many factors to consider are life expectancy and the presence of co-morbidities, such as CKD. Diabetic patients with PAD may have concomitant CKD requiring hemodialysis, which means that the vascular damage is more severe and progresses more rapidly than in diabetic patients without end-stage renal disease leading to a poorer prognosis. Renal disease is one of the most important factors underlying the unfavorable course of an ulcerative lesion, being an independent risk factor for foot ulceration and major amputation.(26,27) Distal revascularization in patients on dialysis patients is a challenge due to their vulnerability to infections, their delay in the healing and the presence of marked calcifications on their vessel walls. Furthermore, the risk of major amputation in this population is 4.7 times higher than in non-dialysed subjects.(28) Diabetic subjects with CKD also experience more perioperative complications such as sepsis and heart failure and there is a high rate of mortality (2.4-13%)(28), with the subgroup of patients in hemodialysis reaching a mortality of 49%, 1 year after an amputation.(28) Doing that analysis in the hemodialysis patients who suffered major amputation in this study, it was found a 1-year survival of 37,5%.
However, despite the complexity of the local and general management of diabetic PAD patients undergoing dialysis, recent data show that 1-year limb salvage can be as high as 65-75%.(29,30) According to these literature values, in the present study, the authors verified an 1-year limb salvage in the population on dialysis of 76,9%.
Hinchliffe et al(11) described limb salvage rates of 78% at 12 mo in endovascular revascularization of NIDF patients.
The present results are comparable to that center with a limb salvage rates of 80,1% at 1 year. Regarding wound healing, they described a 1 year rate > 60%, perfectly comparable with the observed results of 63,2%.
Low patency rates after endovascular interventions, especially in infrapopliteal arteries, and high restenosis rates have been uniformly noted, with a high rate of restenosis and requirement for reinterventions. Reinterventions have been traditionally considered to be benign and successful, without significant consequences on limb outcomes. However, the impact of distal restenosis and reinterventions in patients with critical limb ischemia has not been well characterized(31) Saqib et al.(31) described in his study (including patients without diabetes), primary patency rates at 1 year after endovascular revascularization of 59%, primary-assisted patency rate of 70% and secondary patency rate of 76%.
In the authors department, the follow-up of the revascularized diabetic patients is done by clinical observation of the lesions and evaluation of quality of Doppler pulses. If there is a deterioration of the ulcer healing with worsening of the monophasic Doppler sound or loss of pulses, the patient is routinely proposed to a secondary endovascular procedure.
Concerning the optimal medical treatment, all patients of the present study were put under dual antiplatelet therapy for minimum period of 6 months.
Conclusion
According to the national(2) and international(32) data, it is evident that the increasing use of preventive and vascular care, especially among patients with diabetes, has been associated with lower rates of major amputation(32), giving these patients a better quality of life and increasing their life expectancy.
The results of this study appear to be comparable to specialized centers in treating BTK disease. The author’s data showed that direct arterial flow - angiosomic revascularization - and the number of patent vessels are associated with better results on limb salvage. In contraposition, the presence of CKD is associated with more mortality and the increasing of renal dysfunction was related with the absence of ulcer healing - making this subgroup of patients a real challenge to vascular surgeons.
The results of this study on endodistal revascularization, highlights the need to prioritize investigation and revascularization in neuroischemic diabetic foot patients to improve the outcome of foot ulcer, giving the possibility of salvaging a greater number of limbs.
REFERENCES
1. Shaw JE, Sicrhee RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010;87(1):4-14. [ Links ]
2. Sociedade Portuguesa de Diabetologia. Diabetes: factos e numerous - relatório anual do Observatório Nacional da Diabetes. Edição de 2016. Lisboa. [ Links ]
3. Allie DE, Hebert CJ, Ingraldi A, Patlola RR, Walker CM. 24-carat gold, 14-carat gold, or platinum standards in the treatment of critical limb ischemia: bypass surgery or endovascular intervention? Journal of Endovascular Therapy. 2009;16(1_suppl):134-146. [ Links ]
4. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. J Am Med Assoc 2005;293:217e28. [ Links ]
5. Aiello A, Anichini R, Brocco E, Caravaggi C, Chiavetta A, Cioni R, et al. Treatment of peripheral arterial disease in diabetes: A consensus of the Italian Societies of Diabetes (SID, AMD), Radiology (SIRM) and Vascular Endovascular Surgery (SICVE). Nutrition, Metabolism and Cardiovascular Diseases. 2014 Apr;24(4):355-69. [ Links ]
6. Prompers L, Schaper N, Apelqvist J, Edmonds M, Jude E, Mauricio D, et al. Prediction of outcome in individuals with diabetic foot ulcers: focus on the differences between individuals with and without peripheral arterial disease. EURODIALE Study Diabetologia 2008;51:747e55. [ Links ]
7. Tresierra-Ayala M á., García Rojas A. Association between peripheral arterial disease and diabetic foot ulcers in patients with diabetes mellitus type 2. Medicina Universitaria. 2017 Jul;19(76):123-6. [ Links ]
8. Beckman JA, Creager MA, Libby P. Diabetes and Atherosclerosis. Epidemiology, Pathophysiology, and management. JAMA 2002; 15:2570e81. [ Links ]
9. Lazaris AM, Tsiamis AC, Fishwick G, Bolia A, Bell PR. Clinical outcome of primary infrainguinal subintimal angioplasty in diabetic patients with critical lower limb ischemia. Journal of Endovascular Therapy. 2004;11(4):447-453. [ Links ]
10. DeRubertis BG, Faries PL, McKinsey JF, et al. Shifting paradigms in the treatment of lower extremity vascular disease: A report of 1000 percutaneous interventions. Ann Surg 2007;246:415- 424. [ Links ]
11. Hinchliffe RJ, Andros G, Apelqvist J, et al. Effectiveness of revascularisation of the ulcerated foot in patients with diabetes and peripheral arterial disease: a systematic review. Diabetes/Metabolism Research and Reviews. 2015 doi: 10.1002/dmrr.2705. [ Links ]
12. Gatti C, Cecchini S, Fabbietti P, Romagnoli F, Ricci S. Endovascular treatment of diabetic peripheral arterial disease in older and oldest old patients: a retrospective study. Aging Clinical and Experimental Research. 2018 Feb;30(2):205-7 [ Links ]
13. Norgren L, Hiatt WR, Nehler MR, Harris KA. Fowkes FGR.on behalf of the TASC II Working Group. J Vasc Surg 2007;45(1):S5Ae67A. [ Links ]
14. Brownrigg JRW, Apelqvist J, Bakker K, Schaper NC, Hinchliffe RJ. Evidence-based Management of PAD & the Diabetic Foot. European Journal of Vascular and Endovascular Surgery. 2013 Jun;45(6):673-81. [ Links ]
15. Mingardi R, Morabito A, Piaggesi A, et al. SCAR (SCreening for ARteriopathy) Study Group. Screening for peripheral arterial disease by means of the ankle-brachial index in newly diagnosed type 2 diabetic patients. Diabet Med 2005;22:1310e4.
16. Ferraresi R, Centola M, Ferlini M, Da Ros R, Caravaggi C, Assaloni R, et al. Long-term outcomes after angioplasty of isolated, below-the-knee arteries in diabetic patients with critical limb ischaemia. Eur J Vasc Endovasc Surg 2009 Mar;37(3):336e42. [ Links ]
17. Uccioli L, Gandini R, Giurato L, Fabiano S, Pampana E, Spallone V, et al. Long-term outcomes of diabetic patients with critical limb ischemia followed in a tertiary referral diabetic foot clinic. Diabetes Care 2010 May;33(5):977e82. [ Links ]
18. Caravaggi C, De Giglio R, Pritelli C, et al. Extensive use of pe- ripheral angioplasty, particularly infrapopliteal, in the treatment of ischaemic diabetic foot ulcers: clinical results of a multicentric study of 221 consecutive diabetic subjects. J Intern Med 2002; 252:225e32. [ Links ]
19. Gargiulo M, Maioli F, Ceccacci T, et al. What’s next after optimal infrapopliteal angioplasty? Clinical and ultrasonographic results of a prospective single-center study. J Endovasc Ther 2008 Jun; 15(3):363e9.
20. Jämsén T, Manninen H, Tulla H, Matsi P. The final outcome of primary infrainguinal percutaneous transluminal angioplasty in 100 consecutive patients with chronic critical limb ischemia. J Vasc Interv Radiol 2002;13(5):455e63. [ Links ]
21. Hering J, Angelkort B, Keck N, Wilde J,Amann B. Long-term outcome of successful percutaneous transluminal angioplasty of the fibular artery in diabetic foot syndrome and single-vessel calf perfusion depends on doppler wave pattern at the forefoot. Vasa 2010;39(1):67e75. [ Links ]
22. Werneck CC, Lindsay TF. Tibial angioplasty for limb salvage in high- risk patients and cost analysis. Ann Vasc Surg 2009;23(5):554e9 [ Links ]
23. Van Overhagen H, Spiliopoulos S, Tsetis D. Below-the-knee interventions. Cardiovasc Intervent Radiol. 2013 Apr;36(2):302-11 [ Links ]
24. J.Vouillarmet,O.Bourron,J.Gaudric,P.Lermusiaux,A.Millon,A.Hartemann,Lower- extremity arterial revascularization: is there any evidence for diabetic foot ulcer- healing? Diabete Metab. 42 (1) (2015) 4-15.
25. Chung J. Endovascular Devices and Revascularization Techniques for Limb-Threatening Ischemia in Individuals With Diabetes. Journal of diabetes science and technology. 2017;11(5):904-913. [ Links ]
26. Prompers L, Schaper N, Apelqvist J, Edmonds M, Jude E, Mauricio D, et al. Prediction of outcome in individuals with diabetic foot ulcers: focus on the differences between individuals with and without peripheral arterial disease. EURODIALE Study Diabetologia 2008;51:747e55. [ Links ]
27. Ndip A, Lavery LA, Boulton AJ. Diabetic foot disease in people with advanced nephropathy and those on renal dialysis. Curr Diab Rep 2010;10:283e90. [ Links ]
28. Lepäntalo M, Fiengo L, Biancari F. Peripheral arterial disease in diabetic patients with renal insufficiency: a review. Diabetes Metab Res Rev 2012;28(Suppl. 1):40e5. [ Links ]
29. Hinchliffe RJ, Brownrigg JR, Apelqvist J, Boyko EJ, Fitridge R, Mills JL et al. IWGDF guidance on the diagnosis, prognosis and management of peripheral artery disease in patients with foot ulcers in diabetes. Diabetes Metab Res Rev. 2016 Jan;32 Suppl 1:37-44. doi: 10.1002/dmrr.2698. [ Links ]
30. Graziani L, Silvestro A, Bertone V, Manara E, Alicandri A, Parrinello G, et al. Percutaneous transluminal angioplasty is feasible and effective in patients on chronic dialysis with severe peripheral artery disease. Nephrol Dial Transplant 2007 Apr; 22(4):1144e9. [ Links ]
31. Saqib NU, Domenick N, Cho JS, Marone L, Leers S, Makaroun MS, et al. Predictors and outcomes of restenosis following tibial artery endovascular interventions for critical limb ischemia. Journal of Vascular Surgery. 2013 Mar;57(3):692-9. [ Links ]
32. Goodney PP, Tarulli M, Faerber AE, Schanzer A, Zwolak RM. Fifteen-Year Trends in Lower Limb Amputation, Revascularization, and Preventive Measures Among Medicare Patients. JAMA Surgery. 2015 Jan 1;150(1):84.
Endereço para correspondência | Dirección para correspondencia | Correspondence
Correio eletrónico: rita.augusto1988@gmail.com (R. Augusto).
Ethical responsabilities
Protection of patients and animals: The authors state that for this investigation no experiments were performed on humans and / or animals.
Confidentiality of the data: The authors state that they have followed the centre's established protocols on the publication of patient data.
Right to privacy and informed consent: The authors declare that no patient data is available in this article.
Conflict of interest: The authors declare no potential confict of interest.
Recebido a 02 de julho de 2018
Aceite a 27 de janeiro de 2019

