










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.14 no.1 Lisboa mar. 2018
ARTIGO ORIGINAL
Digital subtraction phlebography using a “homemade” carbon dioxide delivery system
Flebografia de subtração digital utilizando um sistema de libertação de dióxido de carbono “homemade”
Joana Ferreira1, Vânia Pinto2, Jorge Morais2, Lígia Mendes3, Artur Martins2, José Moniz4, Marta Pinto4, Pedro Sousa5
1 Angiologia e Cirurgia Vascular, Centro Hospitalar de Trás-os-Montes e Alto Douro/EPE;
2Bloco Operatório, Centro Hospitalar de Trás-os-Montes e Alto Douro/EPE;
3Escola Superior de Tecnologia de Saúde do Porto (ESTSP) - Instituto Politécnico do Porto
4Internos do Ano Comum, Centro Hospitalar de Trás-os-Montes e Alto Douro/EPE;
5Radiologia, Centro Hospitalar de Trás-os-Montes e Alto Douro/EPE;
Autor para correspondência
ABSTRACT
Introduction and objectives: Carbon dioxide (CO2) is a non-nephrotoxic contrast media. Due its advantages and to the lack of dedicated CO2 delivery system in some hospitals, homemade CO2 delivery systems have been developed in several institutions. The authors describe a CO2 “homemade” delivery system developed with resources available in the author's hospital and present the preliminary results of its application.
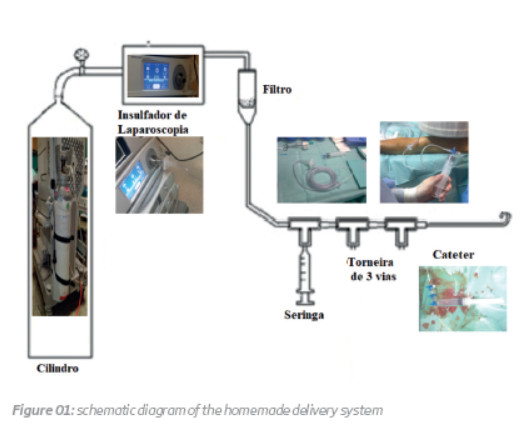
Material and Methods: A disposable aluminum cylinder containing 99.9% pure CO2 is connected to a laparoscopic tower. In the connecting tube, between the laparoscopic tower and a 50 mL syringe there is a filter. The syringe is connected to the connecting tube and to the diagnostic catheter with three three-way stopcock fixed together in line.
Results: From October 2015 and February 2016, six phlebographies, in four patients with dysfunctional arteriovenous fistulas were performed. The procedures were: angioplasty at the cephalic arch stenosis (one intervention); angioplasty at multiple focal stenosis at the basilic vein (two interventions) and angioplasty at multiple focal stenosis at the basilic vein (three interventions). A case of cerebral gas embolism was recorded.
Conclusion: The delivery system we use is useful to maintain the patency of arteriovenous fistula in pre-dialysis patient. However, CO2 injection rate should be reduced, to avoid cerebral gas embolism.
Keywords: Phlebography; Carbon dioxide; homemade.
RESUMO
Introdução e objectivos: O dióxido de carbono (CO2) é um meio de contraste que não causa nefrotoxicidade. Pelas suas vantagens e pela inexistência em alguns centros hospitalares de sistemas “dedicados” de libertação de CO2, têm sido desenvolvidos sistemas “homemade”. Os autores descrevem uma técnica de flebografia de subtração digital utilizando um sistema de libertação de CO2 desenvolvido no seu centro hospitalar. Apresentam ainda os resultados preliminares da sua aplicação.
Material e métodos: Foi utilizado um cilindro de CO2 medicinal (99,9% de pureza), conectado a um insuflador de laparoscopia. O insuflador de laparoscopia está conectado a um tubo de insuflação, que por sua vez está ligado a um filtro.
O filtro está ligado a um sistema venoso e este a três torneiras de três vias alinhadas em série, conectadas a uma seringa de 50 mL e ao cateter de diagnóstico.
Resultados: De outubro de 2015 a fevereiro de 2016 foram realizadas seis flebografias em quatro doentes com fístulas arteriovenosas disfuncionantes. Os procedimentos realizados foram: angioplastia de estenose da crossa da cefálica (uma intervenção); angioplastia de estenoses focais ao longo da veia basílica (duas intervenções), angioplastia de múltiplas estenoses ao longo da veia cefálica (três intervenções). Foi registada uma complicação: embolia cerebral gasosa.
Conclusões: O sistema de libertação de CO2 que usamos é uma mais valia nos doentes insuficientes renais em pré-diálise. Contudo a velocidade de injeção deverá ser adaptada para evitar embolia cerebral gasosa.
Palavras-chave: Flebografia; Dióxido de carbono; “Homemade”.
INTRODUCTION
Arteriovenous fistula should ideally be created six months before starting haemodialysis1. If an endovascular intervention is required in this pre-dialysis patients, iodine contrast should be avoided1. Gadolinium is not advisable due to the known risk of nephrogenic systemic fibrosis2. Therefore, carbon dioxide (CO2) digital subtraction phlebography is an option with remarkable advantages1,3,4. The gas is not nephrotoxic, is inexpensive, easily available and demonstrates a specificity of 97% and sensitivity of 85% in assessing upper limb vein patency and stenosis1,4,5. Before the advent of dedicated CO2 delivery systems, for more than 30 years, many hospitals developed their own systems to deliver the CO21,3,5,6.
The main objective of this paper is to describe a CO2 “homemade” delivery system developed with resources available in the authors hospital. The second end-point is to present the preliminary results of its application.
MATERIAL AND METHODS
Description of the homemade CO2 delivery system
A disposable aluminum cylinder containing 99.9% pure CO2 from Gasin is connected to a laparoscopic tower (Stryker's® 45 L PneumoSure). In the connecting tube between the laparoscopic tower and a 50 mL syringe there is a 0.22 ųm (Bausch + Lomb®) filter. The syringe is connected to the connecting tube and to the diagnostic catheter with three three-way stopcock fixed together in line (figure 1). All injections were performed by hand.
Patients
The record of patients submitted to CO2 digital subtraction phlebography between October 2015 and February 2016 were reviewed. All were pre-dialysis patients with clinical and ultrasound suspicion of hemodynamic significant stenosis in upper limb arteriovenous fistulas.
None had intracardiac right-to-left shunt or severe chronic obstructive pulmonary disease.
In all cases the CO2 was injected in the vein of the arteriovenous fistula, under local anesthesia. The arterial pressure, the heart rate, the oxygen saturation, the conscience state and electrocardiogram were checked during the procedure.
RESULTS
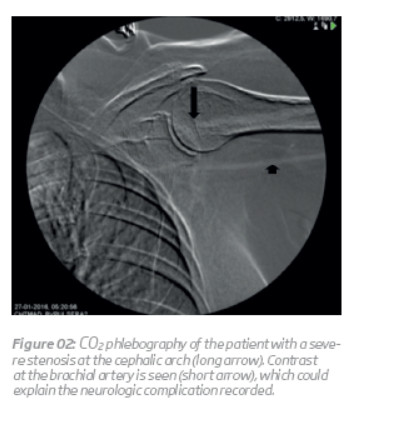
Six phlebographies, in four male patients with a mean age of 81±10.1 years were performed. The mean seric creatinine was 3.33±1.45 mg/dL. Two were brachiocephalic and two were brachiobasilic fistulas. The procedures performed were: angioplasty at the cephalic arch stenosis (one intervention) (figure 2); angioplasty at multiple focal stenosis at the basilic vein (two interventions), angioplasty at multiple focal stenosis at the basilic vein (three interventions). A case of seizures in a patient with a severe cephalic arch stenosis was recorded. No other complications were verified.
DISCUSSION
Advantages and indications:
The major advantages of CO2 angiography is the absence of renal toxicity and anaphylactic reaction2,3,5,6,7,8. In this way, it could be safely used in patients with renal failure or with allergy to iodine contrast2,3,5. For these reasons we consider this technique particularly valuable in the diagnostic and angioplasty of arteriovenous fistula stenosis in pre-dialysis patients.
CO2 is also an inexpensive contrast medium compared with nonionic iodinated contrast and could be combined with iso-osmolar contrasts3,5,6,7,8. Due to its solubility CO2 is rapidly absorbed by the blood and eliminated by the lungs and consequently a huge quantity of CO2 can be used, without adverse consequences2,6,7. These proprieties could be helpful in order to avoid large volumes of iodine contrast in complex procedures57.
Another benefit of this contrast agent is its low viscosity3,5,7,. As a result it can be injected in catheters with an inner diameter of 0.533 mm; between the catheter and guidewire and through the side ports of the stent delivery system3. This characteristic is a major advantage in the detection of gastro-intestinal or traumatic hemorrhage, in identifying previous undetected collaterals, tumor vessels and arteriovenous fistulas3,5,7.
CO2 also prevents the clot formation in the catheter, because it is insoluble in the blood3.
CO2 contrast could be used in any vein or artery and in any intervention, except in the arteries above the diaphragm, being useful for renal interventions (particularly in transplant kidneys) and in pre-operative venous mapping, in pre-haemodialysis patients1,3,5,7,8.
Contraindications and complications:
CO2 - related complications are extremely rare4. Paresthesia, pain at the injection artery, abdominal pain, nausea, tenesmus, seizures, loss of consciousness, bradycardia and hypotension3,5 have been described.
CO2 angiography is contraindicated in cerebral vessels, thoracic aorta and coronary arteries due to the risk of neurotoxicity and myocardial ischemia3,5,7.
It should not be performed with concomitant nitrous oxide sedation or in patients with right-to-left intracardiac shunts5,7. It is relatively contra-indicated in patients with chronic obstructive lung disease and with pulmonary hypertension3,5. To avoid complications in these patients, CO2 injections should be separated by 3 to 5 minutes and the dose of CO2 should be reduced3,7.
Another limitation of CO2 contrast is the deterioration of the image quality associated with the fragmentation of the column of CO22. This problem is compounded in the abdomen because the bowel gas and peristalsis further degrade CO2 imaging3,6.
CO2 can cause spinal cord ischemia, when injected in the aorta in a patient in prone position, because the gas is buoyant and may fill the spinal and lumbar arteries37. It may also cause cerebral embolization when injected into the abdominal aorta with the patient's head in an elevated position, particularly in a hypoplastic aorta3.
Other complication described are bowel ischemia, intrapulmonary vapor lock, and death3,6.
Explanation of the homemade CO2 delivery system:
Several CO2 delivery devices have been used all over the world in the last 30 years1,2,3,5,6. However there are some common basic principles. All use a pure source of CO2, try to avoid air or particles contamination and gas explosive delivery3,7.
In our practice we use a disposable aluminum cylinder containing 99.9% pure CO2. This cylinder should not be directly connected to the diagnostic catheter, because a huge volume of CO2 under high pressure should not be delivered3,,6,,7. As CO2 is a compressible gas and its volume is inversely proportional to the pressure, we use a laparoscopic tower to determine a constant pressure of CO2 and consequently a constant volume3,6. According to the literature the pressure should be 15 mmHg, because at this pressure the volume of CO2 in the syringe will be equal to its capacity6. The syringe capacity chosen was 50 mL, because the volume of CO2 administered should be between 40-60 mL, to avoid explosive delivery3,6. The explosive delivery, results in rapid vessel distention, with consequently pain and poor image quality3)7. The filter is used to remove any particle or bacteria2,3,6. The syringe is connected to the diagnostic catheter and to the connecting tube with three, three-way stopcock fixed together in line. This arrangement in a closed system allow us to remove the residual contaminant air present in the system (the gas is purged three or four times) without disconnecting the syringe, avoiding in this way room air contamination67.
As recommended by several authors, the fluid present in the diagnostic catheter is cleared with injection of 3 to 5 mL of CO2, to decrease the risk of explosive delivery237. Moreover, to minimize this complication, the diagnostic CO2 hand injection should be performed slowly, uniformly and with lower pressure37. CO2 injections should be separated between 2-3 minutes3,6,7,8.
Results
We recorded seizures in a patient with a severe stenosis at the cephalic arch. Probably due to the severity of stenosis, the gas injected in the cephalic vein refluxed to the brachial artery and consequently to the cerebral vessels (figure 2).
To avoid this complication we recommend to lower the patient head, reduce the rate and volume of CO2 injected and manual clamping of the brachial artery.
CONCLUSION
The delivery system we use, is cheap, simple and was developed with resources available in the hospital. The CO2 phlebography is useful to maintain the patency of arteriovenous fistula in pre-dialysis patient. However, CO2 volume and injection rate should be reduced, to avoid brachial artery reflux and consequently neurotoxicity.
REFERENCES
1. Heye S, Fourneau I, Maluex G et al. Preoperative mapping for haemodialysis access surgery with CO2 venography of the upper limb. Eur J Vasc Endovasc Surg 2010;39.340-345. [ Links ]
2. Kawasaki D, Fujii K, Fukunaga M et al. Safety and efficacy of endovascular therapy with a simple homemade carbon dioxide delivery system in patients with iliofemoral artey disease. Circulation Journal 2012 doi: 10.1253/circj.CJ-11-1382. [ Links ]
3. Cho KJ. Carbon dioxide angiography: scientific principles and practice. Vasc Spec Int 2015; 31(3): 67-80. [ Links ]
4. Gahlen J, Hansmann J, Schumacher H et al. Carbon dioxide angiography for endovascular grafting in high-risk patients with infrarenal abdominal aortic aneurysms. J Vasc Surg 2001 (33): 646-649. [ Links ]
5. Funaki B. Carbon dioxide angiography. Semin Intervent Radio l 2008; 25:65-70. [ Links ]
6. Madhusudhan KS, Sharma S, Srivastava DN et al. Comparison of intra-arterial digital subtraction angiography using carbon dioxide by “home made” delivery system and convention iodinated contrast media in the evaluation of peripheral arterial occlusive disease of the lower limbs. Journal of Medical Imaging and Radiation Oncology 2009 (53):40-49. [ Links ]
7. Caridi JG, Hawkins IF, Klioze SD et al. Carbon dioxide digital subtraction angiography: the practical approach. Techniques in Vascular and Interventional Radiology 2001; 4 (1): 57-65. [ Links ]
8. Caridi JG, Stavropoulos S W, Hawkins IF. CO2 digital subtraction angiography for renal artery angioplasty in high-risk patients. AJR 1999 (173) December: 1551-1556. [ Links ]
Correio eletrónico: joana222@hotmail.com (J. Ferreira).
Recebido a 23 de outubro de 2017
Aceite a 20 de março de 2018

