










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkAngiologia e Cirurgia Vascular
Print version ISSN 1646-706X
Angiol Cir Vasc vol.13 no.4 Lisboa Dec. 2017
IMAGEM VASCULAR
Catheter malposition in dextrocardia with situs solitus
Má posição de cateter in situs solitus com dextrocardia
Nuno Carvalho1
1Serviço de Cirurgia Geral, Hospital Garcia de Orta, EPE
Autor para correspondência
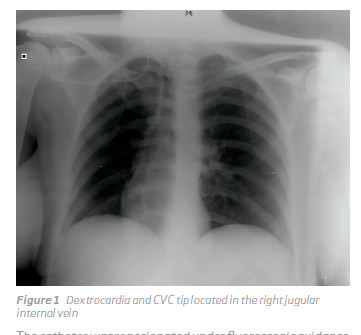
We are reporting a case of a central vein catheter (CVC) that was inserted at the right subclavian vein, without technical difficulties ona 43 year-old woman. She was admited withan extensive hemoperitoneum, and lost her peripheral venous accesses due to drugs addition. The protocoled chest x-ray showed a previously unknown dextrocardia and the CVC tip was located in the right jugular internal vein (Figure 1).
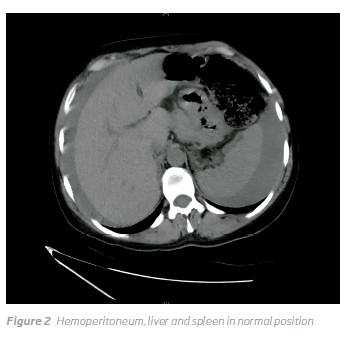
The catheter was reposionated under fluoroscopic guidance. An ectopic pregnancy rupture was diagnosed. The patient was submitted to an uneventful salpingectomy. Previous abdominal CT scan showed normal visceral position, and so dextrocardia with situs solitus was confirmed (Figure 2).
COMMENTS
Dextrocardia is an embryologic malformation characterized by the displacement of the largest axis (base to apex) of the heart to the right side of the chest, with reversion of the apical inclination. The incidence of dextrocardia associated to situs inversus, a situation characterized by the transposition of the abdominal organs, viscera and vasculature in the general population is usually 1:10,000, whereas the one associated with situs solitus, a situation where dextrocartia is associated with normal position of the thoracic and abdominal organs, is 1:30,000 live births1,2.
Many people are unaware of their unusual anatomy until they seek medical attention for an unrelated condition and only when a radiographic assessment of the patient is undertaken, as in our case the diagnosis is achieved3.
The individuals are phenotypically unimpaired, and can lead normal healthy lives, without any complications related to their medical condition4.
Central venous catheters (CVCs) are commonly utilized to gain vascular access for a varied clinical indications.
Complications are well known, namely mechanical, thrombotic and infectious 5,6.
Potential problems that can arise during the implantation procedure include catheter malposition, when the tip of the catheter is not located in superior cava vein, a well-recognized complication. If not addressed it can lead to serious complications7.
Malposition increases the risks of catheter wedging, erosion or perforation of vessel walls, local venous thrombosis, catheter dysfunction, and cranial retrograde injection, in which the infusate is directed to the head instead of the central circulation7. Reposition is almost always indicated.
In our Service, after CVC placement, a radiography of the chest is the accepted way to confirm that the tip is adequately located and to rule out complications related to the procedure. In 2.8% the cannulation failed at the attempted site.8
To our knowledge this is the first report of a CVC insertion at right subclavian vein, with tip malposition in internal jugular vein, in the emergency setting on a patient with situs solitus.
REFERENCES
1. Ahadi R, Shamshirband Two Case Reports of Situs Inversus Totalis. Anat Sci J 2013; 10(2): 111–6 [ Links ]
2. Fabíola Sawaguchi Faig-Leite, Horácio Faig-Leite. Anatomy of a Dextrocardia Case with Situs Arq Bras Cardiol 2008;91(6):e64–e66
3. Ofusori DA, Okwuonu CU, Ude RA, Adesanya Dextrocardia and situs inversus totalis in a Nigerian cadaver: A case report of rare anomaly. Int. J. Morphol., 27(3):837–840, 2009
4. Supriya, S.Saritha, Seema Madan. Situs Inversus Totalis A Case Report. IOSR Journal of Applied Physics , N: 2278-4861. Volume 3, Issue 6 (May. Jun. 2013), PP 12–16
5. Wang L, Liu ZS, Wang Malposition of Central Venous Catheter: Presentation and Management. Chin Med J. 2016;129:227-34.
6. David C. McGee, D., and Michael K. Gould, M.D. Preventing Complications of Central Venous Catheterization. N Engl J Med 2003;348:1123–33. [ Links ]
7. Carlos Roldan, Linda Paniagua. Central Venous Catheter Intravascular Malpositioning: Causes, Prevention, Diagnosis, and Correction. West J Emerg Med. 2015;16(5):658–664.
8. Wolfram Schummer, Claudia Schummer, Norman Rose, Wolf-Dirk Niesen, Samir G. Mechanical complications and malpositions of central venous cannulations by experienced operators A prospective study of 1794 catheterizations in critically ill patients. Intensive Care Med (2007) 33:1055–1059
Correio eletrónico: nunomdc@sapo.pt (N. Carvalho).
Recebido a 19 de julho de 2017
Aceite a 01 de janeiro de 2018

