










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versão impressa ISSN 1646-5830
Acta Obstet Ginecol Port vol.13 no.3 Coimbra out. 2019
CASE REPORT/CASO CLÍNICO
Vaginal breech delivery seen from a different perspective - a case series
Parto pélvico vaginal visto de uma perspetiva diferente - uma série de casos
Andreia Fonseca1, Nuno Clode2
Departamento de Obstetrícia, Ginecologia e Medicina da Reprodução, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte
1. Assistente Hospitalar em Medicina Interna.
2. Director do Serviço de Obstetrícia, Departamento de Obstetrícia, Ginecologia e Medicina da Reprodução Hospital de Santa Maria, Centro Hospitalar Lisboa Norte
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Term breech presentation is a common indication for cesarean delivery. However, concern over the implications of planned cesareans on maternal morbidity and complications for future pregnancies as well as the limitations attributed to the Term Breech Trial have shed new light on the vaginal breech delivery, with different approaches being attempted. We report three cases of term vaginal breech delivery in the upright position, one of them requiring Piper’s forceps for fetal head delivery. No other relevant complications occurred. As with deliveries in lithotomy position, clinical expertise and case selection are prerequisites for favorable maternal and neonatal outcomes.
Keywords: Breech Presentation; Vaginal Delivery.
Introduction
Delivery of the term breech fetus has been a controversial issue in modern Obstetrics. The Term Breech Trial (TBT), published in 2001, caused a major change in practice with cesarean section becoming the preferred mode of delivery1,2. However, methodologic limitations found in the TBT and growing concern over the implications of a planned cesarean delivery in future pregnancies have brought back awareness to the vaginal breech delivery3-6.
Vaginal delivery of the breech fetus is commonly performed in lithotomy position, although most guidelines are not strict concerning positioning7-9. Obstetricians are trained to assist deliveries in this position and, if required, several maneuvers are described to solve potential complications9. Yet, new techniques for the vaginal delivery of the breech fetus have been described and attempted, such as the delivery in the upright position described by Frank Louwen10,11. A recent Cochrane review on maternal position during second stage in women with epidural analgesia considers as upright all positions in which the main axis of the parturient’s body is more than 45 degrees from the horizontal plane12.
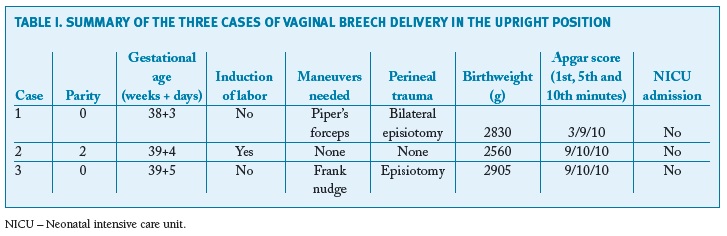
We present 3 cases of vaginal breech delivery in the upright position performed at our hospital (Table I).
Clinical cases
Case 1
Thirty-two-year old nulliparous woman admitted in labor at 38 weeks and 3 days. She was healthy and had a pre-pregnancy body mass index (BMI) of 20.6. The pregnancy was uneventful with a fetal growth estimate on the 50th centile at 32 weeks of gestation and there was no external cephalic version trial. At admission she was 6cm dilated, with complete breech presentation and, after discussion of mode of delivery, she opted for a vaginal delivery. She had epidural analgesia. The second stage of labor took place in the operating room under an oxytocin infusion and with the parturient kneeling and with her hands on the elevated head of the delivery bed. An episiotomy was performed. Delivery of the fetal body was spontaneous. Triple nuchal cord was identified. The head did not deliver spontaneously and the Frank nudge maneuver, described by Frank Louwen, was tried without success. Assuming head entrapment, the parturient was placed in lithotomy position and the Mauriceau-Smellie-Veit maneuver was performed, but also unsuccessful. The cord was clamped and cut, Piper's forceps were applied and a contralateral episiotomy was performed, leading to successful delivery of the head. Birthweight was 2830g. Apgar score was 3/9/10 at 1st, 5th and 10th minute respectively and the umbilical cord blood acid-base analysis revealed a pH of 7.204 with a base excess of -9.7. Besides postpartum anemia (postpartum hemoglobin 9.6g/dL), there were no other maternal complications. Due to jaundice requiring phototherapy, the newborn was discharged only at the seventh day of life. No other neonatal complications occurred and, at 3 years of age, psychomotor development is normal.
Case 2
Thirty-six-year old multiparous woman with two previous normal vaginal deliveries (birthweight 2850g and 3250g) admitted for labor induction at 39 weeks and 4 days. Previously healthy and with a pre-pregnancy BMI of 17.2, she had an uncomplicated pregnancy with an unsuccessful external cephalic version trial. The estimated fetal weight at 36 weeks was in the 12th centile. At admission, the fetus was in frank breech presentation and the cervix was 1cm dilated. Oxytocin was used for labor induction. She had epidural analgesia and delivered spontaneously in the upright position, on her knees and leaning on the headboard. Delivery took place in a delivery room equipped for emergent cesarean deliveries, but no maneuvers were required. There was no need for episiotomy and no perineal trauma ensued. The newborn weighted 2560g and Apgar score was 9/10/10 at 1st, 5th and 10th minute, respectively. No maternal or neonatal complications occurred. The baby is currently healthy, presenting normal development at two and a half years old.
Case 3
Thirty-five-year old healthy nulliparous woman admitted in labor at 39 weeks and 5 days with a frank breech fetus. Pre-pregnancy BMI was 19. No pregnancy complications were reported and, at 35 weeks, estimated fetal weight was in the 27th centile. External cephalic version was tried and unsuccessful. At admission she was 5cm dilated and opted for a vaginal delivery. She had epidural analgesia and an oxytocin infusion was started during second stage. Delivery occurred in a delivery room equipped for emergent cesarean deliveries with the woman on her knees and leaning on the headboard. An episiotomy was performed and fetal body was delivered spontaneously. Frank nudge was used for delivery of the head as spontaneous delivery did not occur with maternal pushing. Birthweight was 2905g and Apgar score was 9/10/10 at 1st, 5th and 10th minute, respectively. There were no maternal or neonatal complications. Today, at two years old, the baby is healthy with normal development.
Discussion
We report three cases of successful vaginal breech delivery in the upright position, only one of them requiring change in position for delivery of the head.
Although it is currently standardized, vaginal delivery did not always take place with the woman in lithotomy position13,14. Recent magnetic resonance imaging (MRI) pelvimetry studies have shown that the kneeling-squat position can significantly increase maternal pelvic diameters15. Such position is comparable to the McRoberts’ maneuver, known to flatten the sacral promontory and used to solve shoulder dystocia in cephalic vaginal deliveries16. Besides changing pelvic dimensions, maternal upright positioning, such as sitting, squatting, standing or staying on all fours with the upper body elevated, promotes the effect of gravity on fetal descent, creates a straighter passage for the fetus and decreases aortocaval compression10.
Based on these arguments, Frank Louwen developed a new technique to perform vaginal breech deliveries, having the woman assume an upright position10,11. Maneuvers for assisting the delivery in the event of extended arms or trapped aftercoming head were described by the author10. In the latter, the Frank nudge maneuver tried in case 1 and successfully used in case 3, the fetal shoulders are pushed against the maternal symphysis promoting the flexion of the head.
Compared to delivery in lithotomy position, the new technique required less maneuvers to deliver the fetus and was associated with less neonatal morbidity10,17. Second stage of labor was also shorter when the woman delivered in the upright position10. Vaginal breech deliveries in the upright position had similar neonatal outcomes when compared to planned cesarean deliveries10.
As with lithotomy position vaginal breech delivery, appropriate case selection and clinicians’ expertise in vaginal breech delivery play a major role on a successful outcome18,19. Maternal wish for a vaginal delivery is a quintessential requirement in case selection as is the exclusion of contraindications for vaginal delivery. Most authors recommend assessment of fetal weight, while some also consider performing x-ray or MRI pelvimetry, in which several pelvic measurements, such as the conjugata vera and the interspinous diameter have been considered predictors of success18,20. Others defend that, in the lack of contraindications for vaginal delivery, favorable progress of labor is the best predictor of success21. An adequate setting is also required. Continuous heart rate monitoring as well as the conditions and team available for an emergent cesarean delivery, should it be needed, are mandatory. Furthermore, a neonatologist should also be available. Regardless of maternal position, all these conditions should be reunited for a safe delivery9.
Some peculiarities pertaining to the cases presented must be pointed out. The two authors were always members of the labor ward team assisting all three deliveries. The first author has learned from Frank Louwen the technique and maneuvers required for vaginal breech delivery in the upright position. The second author has vast experience assisting vaginal breech deliveries in the conventional lithotomy position. The fact that case number 1 was the first vaginal breech delivery in the upright position we performed at our hospital might have influenced the management of head entrapment, as it was also the first time dealing with such a complication in this position. All women were highly motivated for a vaginal delivery and gave their consent for delivery in the upright position. They were also informed that a change in position could occur during delivery. Prior to delivery and during the course of labor, the team assessed all cases for contraindications for vaginal delivery and established a plan for effective management of complications that could ensue. No radiologic pelvimetry studies were carried out. All deliveries occurred with continuous fetal heart monitoring. If signal loss was frequent after rupture of membranes, the team resorted to internal monitoring by placing an internal lead in the fetal buttock.
While the three cases presented resulted in good outcomes for both mothers and newborns and delivery in the upright position is frequently entirely spontaneous, it also requires, as with delivery in lithotomy, expertise in management and assistance.
The current text presents a small case series. However, its publication represents an opportunity to support vaginal breech deliveries. Moreover, in the era of patient-centered medicine, when decisions are shared and parturients’ preferences matter, this case series presents the use of a new technique in Portugal and its favorable outcomes.
In conclusion, we consider that, in the appropriate setting, vaginal breech delivery, either in lithotomy or upright position and upon careful selection of cases, should be given a new chance.
REFERENCES
1. Hannah M, Hannah W, Hewson S, Hodnett E, Saigal S, Willan A. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet 2000;356(9239): 1375-1383.
2. Rietberg C, Elferink-Stinkens P, Visser G. The effect of the Term Breech Trial on medical intervention behaviour and neonatal outcome in The Netherlands: an analysis of 35,453 term breech infants. BJOG 2005;112(2):205-209. [ Links ]
3. Glezerman M. Five years to the term breech trial: The rise and fall of a randomized controlled trial. Am J Obstet Gynecol 2006;194(1):20-25. [ Links ]
4. Schutte J, Steegers E, Santema J, Schuitemaker N, Van Roosmalen J, on behalf of the Maternal Mortality. Maternal deaths after elective cesarean section for breech presentation in the Netherlands. Acta Obstet Gynecol Scand 2007;86(2):240-243.
5. Taylor L, Simpson J, Roberts C, Olive E, Henderson-Smart D. Risk of complications in a second pregnancy following caesarean section in the first pregnancy: a population-based study. Med J Aust 2005;183(10):515-519. [ Links ]
6. Borbolla Foster A, Bagust A, Bisits A, Holland M, Welsh A. Lessons to be learnt in managing the breech presentation at term: An 11-year single-centre retrospective study. Aust New Zeal J Obstet Gynaecol 2014;54(4):333-339. [ Links ]
7. Impey L, Murphy D, Griffiths M, Penna L on behalf of the Royal College of Obstetricians and Gynaecologists. Management of Breech Presentation. BJOG 2017; 124(7):e151-e177. [ Links ]
8. ACOG Committee Opinion No. 745: Mode of Term Singleton Breech Delivery. Obstet Gynecol. 2018 Aug;132(2):e60-e63.
9. Kotaska A, Menticoglou S, Gagnon R, Farine D, Basso M, Bos H, et al. Vaginal Delivery of Breech Presentation. J Obstet Gynaecol Canada 2009;31(6):557-566. [ Links ]
10. Louwen F, Daviss B, Johnson K, Reitter A. Does breech delivery in an upright position instead of on the back improve outcomes and avoid cesareans? Int J Gynecol Obstet 2017;136(2):151-161. [ Links ]
11. Louwen F, Leuchter L, Reitter A. Breech presentation - more than just caesarean vs. spontaneous birth. Z Geburtshilfe Neonatol 2012; 216(4):191-194. [ Links ]
12. Walker K, Kibuka M, Thornton J, Jones N. Maternal position in the second stage of labour for women with epidural anaesthesia. Cochrane Database Syst Rev 2018; Nov 9;11:CD008070. [ Links ]
13. Dundes L. The Evolution of Maternal Birthing Position. Am J Public Health. 1987; 77(5):636-641. [ Links ]
14. Liu Y. Position during labor and delivery: History and perspective. J Nurse Midwifery. 1979;24(3):23-26. [ Links ]
15. Reitter A, Daviss BA, Bisits A, Schollenberger A, Vogl T, Herrmann E, et al. Does pregnancy and/or shifting positions create more room in a woman’s pelvis? Am J Obstet Gynecol 2014; 211(6):662.e1-e9.
16. Gherman R, Tramont J, Muffley P, Goodwin T. Analysis of McRoberts’ maneuver by x-ray pelvimetry. Obstet Gynecol 2000;95(1):43-47.
17. Bogner G, Strobl M, Schausberger C, Fischer T, Reisenberger K, Jacobs V. Breech delivery in the all fours position: a prospective observational comparative study with classic assistance. J Perinat Med 2015;43(6):707-713. [ Links ]
18. Albrechtsen S, Rasmussen S, Reigstad H, Markestad T, Irgens L, Dalaker K. Evaluation of a protocol for selecting fetuses in breech presentation for vaginal delivery or cesarean section. Am J Obs Gynecol 1997;177:586-592. [ Links ]
19. Roman H, Carayol M, Watier L, Le Ray C, Breart G, Goffinet F. Planned vaginal delivery of fetuses in breech presentation at term: Prenatal determinants predictive of elevated risk of cesarean delivery during labor. Eur J Obstet Gynecol Reprod Biol 2008; 138(1):14-22. [ Links ]
20. Hoffmann J, Thomassen K, Stumpp P, Grothoff M, Engel C, Kahn T, et al. New MRI criteria for successful vaginal breech delivery in primiparae. PLoS One 2016;11(8):e0161028. [ Links ]
21. Roumen F, Luyben A. Safety of term vaginal breech delivery. Eur J Obstet Gynecol Reprod Biol 1991;40(3):171-177. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Andreia Fonseca
E-mail: andreiafonseca4@gmail.com
Recebido em: 14/09/2018
Aceite para publicação: 15/07/2019

