










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
Print version ISSN 1646-5830
Acta Obstet Ginecol Port vol.13 no.2 Coimbra June 2019
CASE REPORT/CASO CLÍNICO
Meigs Syndrome with elevated CA 125: case report
Síndrome de Meigs com CA 125 elevado: a propósito de um caso clínico
Ana Lopes Gonçalves1, Miriam Blanco2
Serviço de Medicina Interna, Unidade Local de Saúde do Nordeste, SNS. Bragança.
1 Assistente Hospitalar em Medicina Interna.
2 Assistente Hospitalar Graduada em Medicina Interna
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Meigs syndrome is a rare medical entity. It is defined by a triad of a benign ovarian tumor, ascites and pleural effusion that resolves after tumor resection. This syndrome in known since the 19th century, but its pathophysiology it stills unclear.
It has a progressive incidence from the third decade of life until the menopausal age. Its clinical importance relays on the fact that it is a benign condition with an excellent prognosis, contrary to other ovarian malignancy with peritoneal and pleural metastasis.
The present article aims to report a clinical case of Meigs syndrome.
Keywords: Meigs Syndrome; Pleural effusion; CA 125; Ovarian tumor.
Introduction
Ovarian tumors are known as the sixth prevalent cancer in women, usually diagnosed in the sixth decade of life, and thereby, it is predominantly a disease of postmenopausal women. Ovarian fibromas represent approximately 2-5% of surgically removed ovarian tumors, and Meigs´syndrome occurs in only 1-2%1.
Tumor marker serum levels of CA 125 can be elevated in many diseases, some malignant and some physiologic conditions. In Meigs´ syndrome, it does not correlate with malignancy, the reason why, it is not used as a screening test and it demands histological confirmation of the preoperative diagnosis2.
Clinicians should be aware of this clinical entity because of its benignity and differential diagnosis with malignant ovarian tumors that can be similar at presentation and biochemical results, but have a different approach in treatment and prognosis.
Clinical Case
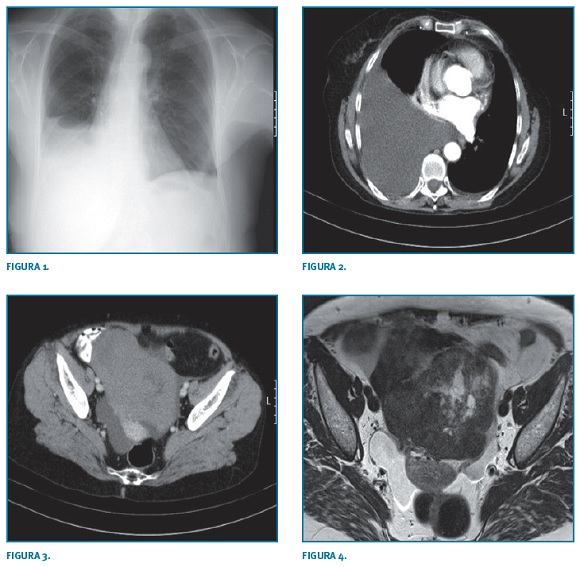
A 67-year-old woman referred to hospital with progressive dyspnea, thoracic and abdominal pain in the right lower quadrant associated with increased abdominal circumference. On physical examination, there was decreased pulmonary murmur on the right side, blown abdominal with a palpable mass in the pelvic region, with certain mobility and ascites. A complete hematological study was carried out, presenting with elevation of inflammatory markers and serum CA125 of 588 IU/ml. Liver and renal functions as other tumor markers were normal. On radiological examination, bilateral pleural effusion was observed.
The thoracic- abdominopelvic CT scan, revealed a solid heterogeneous mass in pelvic midline related with the right adnexa with ascitic fluid and bilateral pleural effusion more relevant on the right. An abdominal MRI was performed after CT for better understanding of the pelvic mass, and showed a lobulated nodular lesion, suggesting cystic degeneration/necrosis, without internal hemorrhagic zones and a moderate enhancement after intravenous contrast, compatible with fibroma/fibro-tecoma.
During the first days of admission it was performed a thoracentesis revealing an exudate and ascitic fluid aspiration which was negative for gram and acid fast stains and showed no malignancy. The patient was submitted to exploratory laparotomy and abdominal hysterectomy with bilateral salpingo-oophorectomy. Pathological examination of specimen was not performed on site, and showed a benign fibroma/thecoma.
The postoperative period was uneventful with respect to surgical complications and the patient was discharged on the seventh postoperative day due to decompensated heart failure and acute kidney injury. The serum CA125 level on the fifth day was 48U/ml. At four weeks postoperatively, the patient was asymptomatic and pleural effusion was resolved at the chest X-Ray. The patient had a normal CA125 level 4months after the operation.
Discussion
In 1937, Meigs´ and Cass widespread attention to the significance of pleural effusion and ascites associated with benign ovarian fibroma. But it is thought that back in 1934, Salmon first described the association of pleural effusion with benign pelvic tumors3.
Although Meigs´ syndrome mimics a malignant condition, it has an excellent prognosis.
Ovarian fibroma is the most common benign ovarian neoplasms and is found in 2-5% surgically removed ovarian tumors. Ascites is present in about 15% of those, specially with larger lesions.
Pleural effusion is present in 1% of the cases, and is more frequently on the right lung4.
The pathophysiology of ascites in Meigs´ syndrome remains unclear. There are theories suggesting that irritation of peritoneal surfaces could stimulate the production of peritoneal fluid4,5, meanwhile, others proposed mechanisms of direct pressure on surrounding lymphatics or vessels. Hormonal stimulation or release of mediators from the tumor that increased capillary permeability were also proposed5,6.
The pleural effusion, also has an unclear etiology. In most of the cases is located on the right side, but about 11% may also occur on the left side7,8.
CA 125 antigen is a tumor marker that can appear in many adult tissues. Is found elevated in some benign and physiologic conditions such as menstruation, peritonitis, endometriosis and cirrhosis7-9.
The association of Meigs´ syndrome with elevation of serum CA125 is thought to be caused by mesothelial expression of CA 125 rather than by fibroma7,8,10.
It is of paramount importance to remeber that the combination of pelvic mass, abdominal ascites, pleural effusion and elevated serum CA125 antigen does not always predict a menacing diagnosis. This case illustrates the importance of histopathologic confirmation of Meigs´ syndrome as a small percentage of patients will have a benign etiology despite an elevated serum CA 125 level.
REFERÊNCIAS BIBLIOGRÁFICAS
1. Yazdani S, Alijanpoor A2, Sharbatdran M3, Bouzari Z1, Abedisamakoosh M4, et al. (2014) Meig´s syndrome with elevated serum CA 125 in a case of a ovarian fibroma/thecoma. Caspian J Intern Med 5:43-45.
2. Vieira SC, Pimentel LH, Riberiro JC, de Andrade Neto AF, de Santana JO (2003) Meigs´syndrome with elevated CA 125: case report. Sao Paulo Med J 121: 210-212.
3. MEIGS JV (1954) Fibroma of the ovary with ascites and hydrothorax; Meigs´syndrome. Am J Obstet Gynecol 67:962-985.
4. D. Timmerman, P. Moerman, I. Vergote (1995) Meigs´syndrome with elevated serum CA 125 levels: two case reports and review of the literature. Gynecol Oncol, 59: 405-408.
5. Y.H. Turan, L.C. Demirel, F. Ortaç (1993) Elevated CA 125 in Meigs´ syndrome. Int J Gynaecol Obstet, 43: 64-54.
6. J.Y. Lin, C. Angel, J.Z. Sickel (1992) Meigs syndrome with elevated serum CA 125. Obstet Gynecol, 80:563-566.
7. I. Jacobs, R. C. Bast Jr. (1989) The CA 125 tumor-associated antigen: a review of the literature. Human Reprod 4:1-12.
8. E. Zuckerman, A. Lanir, E. Sabo, T. Rosenvald-Zuckerman, I. Matter, D. Yeshurun, et al (1999) Cancer antigen 125: a sensitive marker of ascites in patients with liver cirrhosis. AM J Gastroenterol 94: 1613-1618.
9. M. Benjapibal, S. Sangkarat, S. laiwejpithaya, B. Viriyapak, et al (2009) Meigs´syndrome with elevated serum CA 125: case report and review of the literature. Case Rep Oncol 2(1): 61-66.
10. JH. Liou, T. Cheng Su, JC. Hsu (2011) Meigs´syndrome with elevated serum cancer antigen 125 in a case of ovarian sclerosing stromal tumor. Taiwanese J of Obstet and Gynecol 50 (2): 196-200.
Endereço para correspondência | Dirección para correspondencia | Correspondence
Ana Lopes Gonçalves
Unidade Local de Saúde do Nordeste
Bragança, Portugal
E-mail: ana.t.gonc@gmail.com
Recebido em: 07/06/2018
Aceite para publicação: 27/08/2018

