










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versão impressa ISSN 1646-5830
Acta Obstet Ginecol Port vol.12 no.1 Coimbra mar. 2018
CASE REPORT/CASO CLÍNICO
Adjuvant radiotherapy for endometrial cancer in a patient with pelvic kidney
Radioterapia adjuvante no cancro do endométrio em doente com rim pélvico
Cátia Pedro*, Pedro Silva*, Catarina Travancinha**, Paula Pereira***, Filomena Santos****
Serviço de Radioterapia - Instituto Português de Oncologia de Lisboa Francisco Gentil, E.P.E.
*Interno de Formação Específica em Radioncologia, Serviço de Radioterapia do Instituto Português de Oncologia de Lisboa Francisco Gentil, E.P.E
**Assistente de Radioncologia, Serviço de Radioterapia do Instituto Português de Oncologia de Lisboa Francisco Gentil, E.P.E
***Assistente Graduada de Radioncologia, Serviço de Radioterapia do Instituto Português de Oncologia de Lisboa Francisco Gentil, E.P.E
****Assistente Graduada Sénior de Radioncologia, Serviço de Radioterapia do Instituto Português de Oncologia de Lisboa Francisco Gentil, E.P.E
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
There is currently few data regarding radiation tolerance of a transplanted kidney. We report on a patient with renal transplant, submitted to surgery for endometrial cancer, followed by chemotherapy and radiotherapy. She was treated with Intensity-Modulated Radiation Therapy(IMRT) to a dose of 45Gy to the target volume and a mean dose of 6,4Gy to the graft. After one year of follow-up, she remains free of disease and has normal renal function. Pelvic radiotherapy in the setting of a transplanted kidney is feasible with IMRT. A mean dose of 6,4Gy to the graft seems to be safe to preserve renal function.
Keywords: Radiotherapy; Renal transplantation; Radiation tolerance.
Introduction
Kidney transplantation is one of the main treatments for patients with end-stage renal disease. The use of immunosuppressive agents has led to the reduction of acute graft rejections and the increase of survival. However, the prolonged immunosuppression is associated with increased risk of cancer. In fact, malignancy is the third most common cause of death in renal transplant recipients1.
In the literature, there are only case reports and small series with patients with transplanted kidney who were submitted to pelvic radiation therapy. When planning radiotherapy, the presence of a pelvic kidney near the radiation field must be taken into consideration to adequately treat the cancer, while preserving graft function.
Regarding endometrial cancer, surgery is the standard care. However, radiotherapy and chemotherapy are also indicated as adjuvant treatment for patients with intermediate risk, high risk or unfavorable histology, for their improvement in local control and progression-free survival2-5.
We report the case of a patient with renal transplant, who received pelvic radiation therapy in the setting of adjuvant treatment for endometrial cancer.
Case report
A 54-year-old female patient with history of renal transplantation due to chronic kidney disease, under immunosuppressive treatment with mycophenolate and sirolimus.
She presented with post-menopause metrorragia. During gynecologic examination, an endocervical polyp was detected and biopsies of the polyp, cervix and endometrium were performed. The diagnosis was endometrioid carcinoma of the endometrium. Imaging studies showed a large mass in the uterine fundus that extended to the left uterine ostium, without suspicious lymph nodes or distant metastases. A single kidney was present on the right iliac fossa.
The patient was submitted to total hysterectomy with bilateral salpingectomy and oophorectomy and bilateral pelvic lymphadenectomy. Histopathological examination revealed mixed carcinoma of endometrium with a predominant endometrioid component (moderately differentiated, 95%) and a serous component (5%). Invasion of the cervical stroma was present, but not parametrial involvement. The left ovary was invaded. None of the ten lymph nodes dissected had cancerous cells. The tumor was staged as pT3a pN0 M0 and as International Federation of Gynecology and Obstetrics (FIGO) stage IIIA.
The patient was then submitted to four courses of carboplatin/ paclitaxel chemotherapy, which were well tolerated, followed by radiation therapy.
Before radiotherapy, initial laboratory tests were taken and renal function was found normal. The patient was informed of the benefits and risks of radiation therapy. For treatment planning, a computed tomography with 3-millimeter slices was obtained, with a full bladder and empty rectum. The clinical target volume (CTV) and organs at risk (bladder, rectum, renal graft, femoral heads and bowel bag) were contoured. CTV was defined according to RTOG (Radiation Therapy Oncology Group) 0418: it included the upper 3 cm of the vagina and 1 cm bellow the obturator foramen, paravaginal soft tissues and the common, external iliac, internal iliac and presacral lymph node regions6. Planning Target Volume (PTV) was obtained expanding the CTV of the tumor bed with a 10 mm margin and the CTV of the lymph node regions with a 7 mm margin, both in all directions.
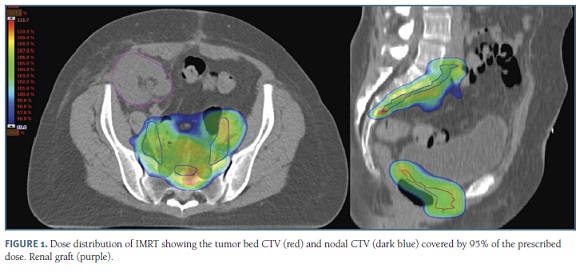
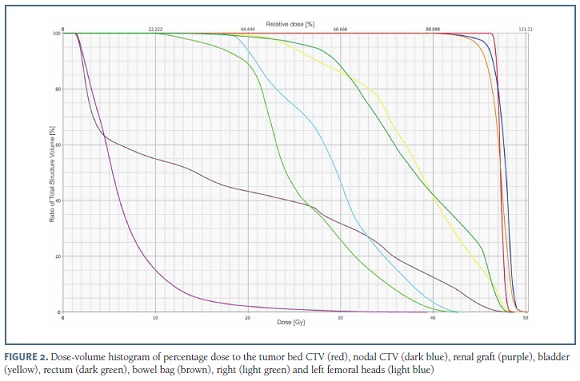
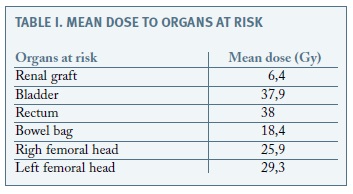
Forty-five Gy at 1,8 Gy per fraction (25 fractions) were prescribed using IMRT (Intensity-Modulated Radiation Therapy) (Figure 1). This allowed the delivery of a therapeutic dose to the target volume, with an adequate coverage of the PTV (95% of the volume of PTV received 99,1% of the prescribed dose) and a reduced dose to the organs at risk (within tolerable constraints defined by RTOG 0418 and QUANTEC (Quantitative Analyses of Normal Tissue Effects in the Clinic8)) (Figure 2). The graft received a mean dose of 6,4 Gy and 28% of its volume received a maximum dose of 7,5 Gy (Table I).
After external beam radiation therapy, the patient was submitted to high-dose-rate vaginal brachytherapy, with 15 Gy at 5 Gy per fraction (3 fractions). Both radiation treatments were well-tolerated.
After one year of follow-up, the patient remains free of disease and maintains normal renal function.
Discussion
Radiotherapy is one of the most commonly used treatments given to cancer patients. However, it is associated with adverse effects and, in the particular case of patients with kidneys near the radiation field, there is an increased risk of nephrotoxicity. Therefore, in patients with renal transplant submitted to pelvic radiation therapy, graft function preservation is also a goal to achieve. Since critical organs should not have their dose tolerance exceeded due to the increased risk of toxicity, the dose received by the renal graft must be carefully taken into consideration during treatment planning. However, data regarding tolerance dose of the transplanted kidney is sparse.
Among the studies currently used as reference to indicate tolerance dose of critical organs, none considers the existence of a single kidney. Both QUANTEC, Emami et al. and RTOG consensus establish tolerance constraints while considering the presence of bilateral kidneys6-8. And among the few case reports and small series with patients with transplanted kidney treated with pelvic radiotherapy9-15, we only found three articles that had any dosimetric information about the graft. Dahlke et al. did a retrospective analysis of nine patients with renal transplant and pelvic cancer (prostate, rectal, anal carcinoma and Hodgkin lymphoma) treated with radiotherapy13. The mean dose to the graft was between 0,1 Gy and 6,4 Gy. No one had transplant failure. Mohiuddin et al. reported on a patient with a transplanted kidney submitted to adjuvant radiotherapy for cervical cancer14. No more than 28% of the graft received 10 Gy and she also did not have any decrement in renal function. Detti et al. described a case of a patient with prostate cancer that maintained normal renal function after receiving a mean dose of 1,88 Gy to the transplanted kidney15.
In order to reduce the dose to the graft, as well as the remaining critical organs located in the vicinity of the treatment volume (such as bladder, rectum, femoral heads and bowel bag), the technique of radiotherapy must also be chosen carefully. IMRT is a technique that produces a more conformal volume than conventional 3D-conformal radiation therapy, providing an optimized coverage of the target volume, with a rapid fall-off gradient between the target and the surrounding normal tissues, reducing the dose to the organs at risk16. Previous studies have shown that it is associated with less acute17-18 and chronic18-19 toxicity than 3D-conformal radiation therapy.
The patient was also submitted to high-dose-rate vaginal brachytherapy, where a radioactive source is placed temporarily inside the vagina. This gives an additional boost with high-dose localized radiation to the vagina and, because it has a steep dose gradient, the surrounding organs receive a very low dose20.
In conclusion, even though the presence of a renal graft near the radiation field may have an adverse impact on treatment delivery, it possible to treat patients with pelvic cancer and kidney transplant. IMRT can provide an adequate target coverage, while sparing the organs at risk, including the graft. To preserve graft function, its dose should be as low as possible, without compromising the target volume. A mean dose of 6,4 Gy seems to be well-tolerated by the graft in order to maintain normal renal function.
REFERENCES
1. Rama I, Grinyó JM. Malignancy after renal transplantation: the role of immunosuppression. Nat Rev Nephrol 2010;6:511-519. [ Links ]
2. Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, Jobsen JJ, Wárlám-Rodenhuis CC, et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: Multicentre randomized trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet 2000;355:1404-1411. [ Links ]
3. Keys HM, Roberts JA, Brunetto VL, Zaino RJ, Spirtos NM, Bloss JD, et al. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a Gynecologic Oncology Group study. Gynecol Oncol 2004;92(3):744-751. [ Links ]
4. Hogberg T, Signorelli M, de Oliveira CF, Fossati R, Lissoni AA, Sorbe B, et al. Sequential adjuvant chemotherapy and radiotherapy in endometrial cancer - Results from two randomised studies. Eur J Cancer 2010;46(13):2422-2431. [ Links ]
5. Greven K, Winter K, Underhill K, Fontenesci J, Cooper J, Burke T. Final analysis of RTOG 9708: Adjuvant postoperative irradiation combined with cisplatin/paclitaxel chemotherapy following surgery for patients with high-risk endometrial cancer. Gynecol Oncol 2006;103(1):155-159. [ Links ]
6. Small W, Mell LK, Anderson P, Creutzberg C, De Los Santos J, Gaffney D. et al. Consensus guidelines for delineation of clinical target volume for intensity-modulated pelvic radiotherapy in postoperative treatment of endometrial and cervical cancer. Int J Radiation Oncology Biol Phys 2008; 71(2):428-434. [ Links ]
7. Dawson LA, Kavanagh BD, Paulino AC, Das SK, Miften M, Li XA, et al. Radiation-associated kidney injury. Int J Radiat Oncol Biol Phys 2010;76(3 Suppl):S108-115. [ Links ]
8. Emami B, Lyman J, Brown A, Coia L, Goitein M, Munzenrider JE, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys 1991;21(1):109-122. [ Links ]
9. Castilho MS, Jacinto AA, Viani GA, Campana A, Carvalho J, Ferrigno R, et al. Intensity Modulated Radiotherapy (IMRT) in the postoperative treatment of an adenocarcinoma of the endometrium complicated by a pelvic kidney. Radiat Oncol 2006;1:44. [ Links ]
10. Ramamurthy R, Muthusamy V, Hussain SA. Approach to carcinoma cervix with pelvic kidney. Indian J Surg Oncol 2010; 1(4):323-327. [ Links ]
11. Mouzin M, Bachaud JM, Kamar N, Gamé X, Vaessen C, Rischmann P, et al. Three-dimensional conformal radiotherapy for localized prostate cancer in kidney transplant recipients. Transplantation 2004;78(10):1496-1500. [ Links ]
12. Konety BR, Tewari A, Howard R, Barry JM, Hodge EE, Taylor R, et al. Prostate cancer in the post-transplant population. Urology 1998;52: 428-432. [ Links ]
13. Dahlke S, Schwarz A, Bruns F, Bremer M, Miemietz M, Christiansen H, et al. Pelvic Radiotherapy after Renal Transplantation. Anticancer Res 2012;32(11):5083-5086. [ Links ]
14. Mohiuddin MM, Mahmood U, Hall AA, Rosenshein N. Adjuvant pelvic irradiation for cervical cancer in the setting of a transplanted pelvic kidney. J Cancer Res Ther 2012;8(3):427-429. [ Links ]
15. Detti B, Scoccianti S, Franceschini D, Villari D, Greto D, Cipressi S, et al. Adjuvant radiotherapy for a prostate cancer after renal transplantation and review of the literature. Jpn J Clin Oncol 2011;41(11):1282-1286. [ Links ]
16. Heron DE, Gerszten K, Selvaraj RN, King GC, Sonnik D, Gallion H, et al. Conventional 3D conformal versus intensity-modulated radiotherapy for the adjuvant treatment of gynecologic malignancies: a comparative dosimetric study of dose-volume histograms. Gynecol Oncol 2003;91(1):39-45. [ Links ]
17. Mundt AJ, Lujan AE, Rotmensch J, Waggoner SE, Yamada SD, Fleming G, et al. Intensity-modulated whole pelvic radiotherapy in women with gynecologic malignancies. Int J Radiat Oncol Biol Phys 2002;52(5):1330-1337. [ Links ]
18. Gandhi AK, Sharma DN, Rath GK, Julka PK, Subramani V, Sharma S, et al. Early clinical outcomes and toxicity of intensity modulated versus conventional pelvic radiation therapy for locally advanced cervix carcinoma: a prospective randomized study. Int J Radiat Oncol Biol Phys 2013;87(3):542-548. [ Links ]
19. Mundt AJ, Mell LK, Roeske JC. Preliminary analysis of chronic gastrointestinal toxicity in gynecology patients treated with intensity-modulated whole pelvic radiation therapy. Int J Radiat Oncol Biol Phys 2003;56(5):1354-1360. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Cátia Pedro
E-mail: catia.mpedro@gmail.com
Recebido em: 06/06/2017
Aceite para publicação: 03/08/2017

