










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMotricidade
versão impressa ISSN 1646-107X
Motri. vol.16 no.1 Ribeira de Pena mar. 2020
https://doi.org/10.6063/motricidade.16461
ORIGINAL ARTICLE
The effect of three different training programs in elderly women's isokinetic strength
António M. Monteiro1,3, Pedro Miguel Forte1,2,3[*], Joana Carvalho4
1 Instituto Politécnico de Bragança, Bragança, Portugal
2 Department of Sport Sciences, Higher Institute of Educational Sciences of the Douro, Penafiel, Portugal
3 Research Center in Sports, Health and Human Development, CIDESD, Vila Real, Portugal
4 Research Centre in Physical Activity Health and Leisure, Faculty of Sport, University of Porto, Porto, Portugal
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
This study aimed was to assess the effects of three different training protocols in quadriceps and hamstrings isokinetic muscle strength of independent elderly women. Eighty women were recruited for this study and divided into four groups of twenty subjects: the control group, the multi-component group, the muscle power group, and the muscular resistance strength group. The isokinetic strength was measured in both lower limbs with a dynamometer at 60°/s and 180º/s. The multivariate analysis (ANOVA) and the Bonferroni test assessed the group and time effect. Significant and positive effects were observed in the time and group interaction in the power group at 180°/s and 60°/s knee flexion in the dominant (p = 0.004, respectively) and non-dominant (p = 0.046 and p = 0.041, respectively) lower limbs. The Control group had significant and negative effect on the time x group interaction at 180°/s and 60°/s on the extension of the dominant knee (p = 0.008 and p = 0.001, respectively) and non-dominant (p = 0.003 and p< 0.001, respectively). The muscle power training seems to be the most effective to increase the isokinetic strength in older independent women. All the training programs appear to contribute to decreasing the age-related loss on isokinetic strength.
Keywords: Elderly, Women, Strength, Isokinetic, Lower Limbs
Introduction
Aging process is related to muscle size reduction (muscular atrophy), motor unit's loss, and reduction of the contraction speed. These lead to muscular strength, power, and resistance reduction (Arakelian et al., 2018; Frontera et al., 2000; Traczyk et al., 2018). The literature describes that sarcopenia affects motor and muscular performance (Frontera et al., 2000; Greenlund & Nair, 2003; Moran, Ramirez-Campillo & Granacher, 2018; Vandervoort, 2002). The muscular function losses can reduce physical fitness and independence in daily life activities. Even more, the elderly's high dependency levels are positively associated with a higher risk of falls (Carrasco-Poyatos et al., 2019; Cress & Meyer, 2003).
Muscular power and resistance play an important role in the elderly's autonomy. Some studies suggested that the lower limbs power reduction might compromise elderly's functional mobility and fall prevention (Bean et al., 2003; Cadore et al., 2014; Kiely, et al., 2002; Marsh et al., 2006; Suetta et al., 2004). Several authors (Bean et al., 2003; Reid & Fielding, 2012) reported that the difficulty of accomplishing some daily life activities such as climbing, go down stairs or chairs and walk faster may have a higher relation with power loss than with muscular strength. Moreover, other studies suggested that muscular power exceeds the strength reduction with age (McNeil et al., 2007; McPhee et al., 2018). Different studies describe that it is possible to improve the post-training muscular functionality (Aquino et al., 2002; Carvalho et al., 2010). Others appointed that the resistance also improves muscular power (Henwood et al., 2008; Hurley & Roth, 2000). Training programs that required a higher velocity execution are positively related with the muscular power increase, and the power training has been characterized by (Bean et al., 2009; de Vos et al., 2005; Henwood & Taaffe, 2005; Marsh et al., 2009; Orr et al., 2006): (i) Concentric repetitions as faster as possible; and (ii) eccentric phases during two or three seconds. This training method presents benefits in muscular strength and power. However, the literature seems to be scarce in with the elderly's data (Chodzko-Zajko et al., 2009; Henwood et al., 2008).
Otherwise, multi-component training has been recommended for elderlies (Carvalho et al., 2010; Worm et al., 2001). However, it is hard to find studies with this training method with concordant data. As for as our understanding goes, some authors reported that multi-component training does not have any effect in muscular function (Nelson et al., 2004; Puggaard, 2003). However, others suggest that this methodology has benefits in muscular function (Toraman et al., 2004; Worm et al., 2001).
The resistance strength training effects seems to be consensual. However, the strength power training and multi-component training have presented contradictory results. Most of the studies that evaluate the training effects used evaluation methods based on functional and clinical tests (Carvalho et al., 2009; Henwood et al., 2008). Isokinetic evaluation is one of the most precise tests for strength evaluation (Suetta et al., 2004). However, it has an associated high cost, in comparison to other tests (ACSM, 2006).
Thus, this study aimed to evaluate the effect of three different exercise programs (Multi-component versus Strength Power versus Resistant Strength) in independent elderlies' hamstrings and quadriceps isokinetic strength.
MethodsThis is a longitudinal randomized controlled trial. The participants underwent a training program three times a week for eight months. Four groups of twenty participants were part of this research, three groups were under strength training protocols, and one group was not in any type of physical exercise program.
Participants
Eighty volunteered female elderlies were recruited for this research. The subjects were divided in four groups: (i) control group (CG), not under a physical exercise program; (ii) group under a strength power-training program (PG); (iii) group under a strength resistance-training program (RG) and, (iv) group under a multi-component training program, based on physical fitness (MG).
The participants were informed and agreed to participate in this research. Written consent was obtained. All the procedures were in accordance with the Helsinki Declaration regarding human research.
The inclusion criteria were: (i) subjects with more than 65 (including) years old; (ii) that do not participate in regular physical activities (two sessions per week with moderate to vigorous intensity with 20 or more minutes per session), in the last year; (iii) do not have any chronic neuromuscular, cardiovascular and metabolic diseases that may compromise the safety of physical exercise sessions and/or evaluations; (iv) be available to participate in three weekly sessions and the different evaluation moments.
The exclusion criteria were: (i) fail at least one evaluation moment; (ii) the control group participate in any exercise program during this research; (iii) in the intervention group, fail at least 15% of the exercise sessions or 10 consecutive sessions.
The participants were advised to maintain their daily-life routine, their physical activity (PA), and nutritional pattern. The subjects that were under medication were informed to maintain it during the exercise program. The subject's attendance in the exercise sessions was about 96%. The sample characteristics are described in Table 1.

(clique para ampliar ! click to enlarge)
Intervention Programs
The physical education programs had a duration of 8 months (October to June of the next civil year) in noun-consecutive days (Monday, Wednesday, and Friday).
Strength Training Program: Each experimental group sessions of the strength training (PG and RG), started with a warm-up with 8-10 minutes walking and/or ergometric bicycle (Tectrix, Bike-Max, USA) and rowing (Concept II, Morrisville, VR, USA) with low intensity and some stretching exercises. During the principal session training part, occurred a specific strength period with six exercises in the following variable resistance machines (Nautilus Sports/Medical Industries, Independence, VA, USA): leg press, fly machine, bench press, lat pull down, leg extension, leg flection.
The Lumbar and abdominal resistance training occurred during the strength training. These resistance training were made with 3 sets of 20 repetitions. The set of recovery and stretching exercises were at the end of the session.
The muscular strength and power training followed the ACSM (2009) recommendations. The training intensity increased during the first two weeks in agreement with the linear periodization. The sessions of the first week allowed to assess the individual maximal individual repetition (1RM) and participant's adaptation to the machines. The 1RM was evaluated at the end of each two weeks during the first month. Then it was evaluated every four weeks until the end of the program. The exercise intensity was in 12 to 14 in the Borg's (1998) rate of perceived exertion.
Power Strength Program: The exercises organization were in stations. Due to the high nervous system participation and fatigue effect in these exercises, the most complex (multiarticular) were firstly performed (ACSM, 2009). The exercises execution was fast (<10seg), and the training adaptations were with 3 to 4 sets of 3 to 6 repetitions. The training intensity ranged between 40% (first 4 weeks) and 60% of 1 RM. The resting and recovery interval ranged from 3 to 5 minutes.
Resistive Strength Program: The exercises were organized in stations, and the resting time between exercised were between 1 and 2 minutes. During the adaptation time (first week), the training loads ranged between 40% and 60% of 1RM (15 to 20 repetitions). After that, the exercise intensity was between 60% and 80%, and two to three sets of 8 to 12 repetitions were performed.
Multi-component Program: This program was based on Carvalho et al. (2009) recommendations. The sessions volume ranged between 50 to 60 minutes and subdivided into five fundamental parts: 1) 5 to 8 minutes of general warm-up with walking and stretching exercises; 2) walking with aerobic exercises like jogging and aerobic gymnastic and dance (15 to 20 minutes), with a minimum of 8-10 min aerobic exercise; the intensity was between 12 and 14 in the subjective perception effort scale of Borg (1998); 3) 1 to 3 sets of exercises of muscular resistance with elastics and weights were made in circuit (with a resting period between sets of 40 to 60 seconds). These exercises requested the main muscular groups such as knees flexors/extensors, shoulders abductors and adductors, elbows flexors/extensors, pectorals, abdominals, and lumbar. To ensure exercise adaptation along with a correct breading synchronization technic, the first month had a lower intensity. The participants started with one set of eight repetitions and increased load and intensity until 3 sets of 12 to 15 repetitions; 4) Static and dynamic balance training with sticks, balls, and balloons during 5 to 8 minutes; 5) at the end of each session, was adopted an active recovery period with stretching and breading exercises.
Evaluation Procedures
Isokinetic strength: The isokinetic muscle strength of knees flexors and extensors were assessed in booth lower limbs with a dynamometer (Biodex System 2, NY, USA) at 60º/s and 180º/s. The lower limbs articular position and alignments followed the instructions of Biodex Medical System, Inc (Wilk, 1991). The bands were placed at the elderly's trunk, hip, and thigh to stabilize the movements and isolate knees flection and extension. The alignment of the dynamometer rotation axis was with the femoral epicondyle. The dynamometer load cell was 2cm above the internal malleoli. The angular anatomical knee reference was obtained with a goniometer. Possible errors were taken into account in the torque by the gravitational force. The correction was based on the lower limb weight at 0º/s, and calculated by the equipment software.
Before the test, the elderlies warmed up in an ergometer bicycle (Monark, Sweden) during 5 minutes at 60 rotations per minute. The ergometer load was calculated with 2% of the participant’s bodyweight. The subjects had an adaptation period with 10 submaximal repetitions of knee flexion/extension at the test speed. The subjects had a resting period of 2 minutes between exercises.
To assess the isokinetic strength, each participant made five maximal repetitions at 180º/s and three at 60º/s, resting 2 minutes between tests. The range of motion varied between 90º of knees flection to the maximal and possible extension and strength. During the execution, feedback was given to help participants to reach their maximal possible strength. The following parameters were considered for booth lower limbs: Maximal moment (peak torque - N.m); Extensors/flexors ratio (hamstrings/quadriceps - %) that represented the ratio between the maximal knee flection and extension moment.
The lateral dominance was self-reported by the subjects. The answer (right or left) was obtained by the question "What is your favourite leg?" or "Which leg do you use to kick objects?".
Statistical Analysis
The distributions normality was tested with the Kolmogorov-Smirnov test, and the Levene test allowed to evaluate the homoscedasticity (Maroco, 2007). The following conditions were tested: (1) the dependent variable presented normal distribution; (2) the population variances presented homoscedasticity. The normality and homoscedasticity assumptions were verified.
The repeated measures multivariate analysis (ANOVA) was made to assess the four groups' differences in the two different moments. The test allowed to evaluate the differences in each group and moment. Bonferroni's test allowed multiple means comparisons (group x time). The perceptual changes (changes %) were calculated by the equation [(post-test - pre-test)/pre-test) x100].
The adopted statistical significance was p<0.05. The analysis was made in Statistical Package for Social Sciences version 19.0 (SPSS 19.0).
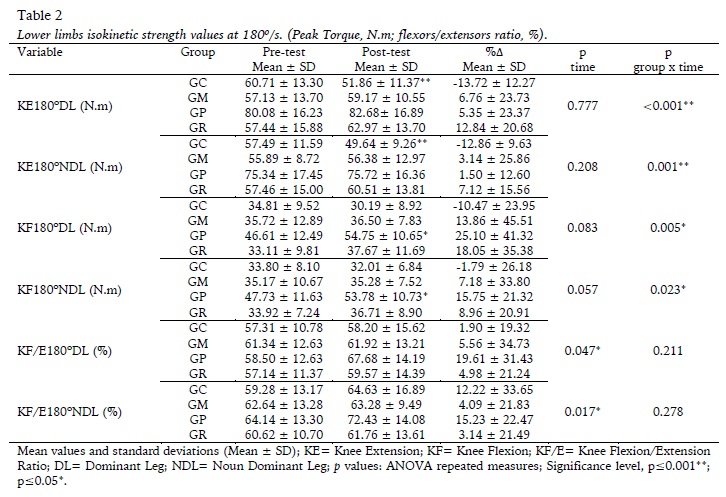
ResultsThe ANOVA analysis revealed a significant effect in time x group interaction and for the following isokinetic variables at 180º/s: Knee extension at 180º/s of the dominant leg (KE180DL) (F(3; 76) = 7.351, p <0.001); Knee extension at 180º/s of the noun dominant leg (KE180NDL) (F(3; 76) = 5.831, p=0.001); Knee flection at 180º/s of the dominant leg (KF180DL) (F(3; 76) = 4.685, p=0.005); and Knee flection at 180º/s of the noun dominant leg (KF180NDL) (F(3; 76) = 3.379, p=0.023).
In the time x group interaction, significant differences were observed between the pre and post-test in a negative direction in the CG for KE180DL (13.72%; p=0.008) and KE180NDL (12.86%; p=0.003). The power group presented significate differences in KF180DL (25.1%; p=0.05) and KF180NDL (15.75%; p<0.046). The hamstrings/quadriceps ratio did not present significant differences. The lower limbs isokinetic strength values at 180º/s are presented in Table 2.
(clique para ampliar ! click to enlarge)
Mean values and standard deviations (Mean ± SD); KE= Knee Extension; KF= Knee Flexion; KF/E= Knee Flexion/Extension Ratio; DL= Dominant Leg; NDL= Noun Dominant Leg; p values: ANOVA repeated measures; Significance level, p≤0.001**; p≤0.05*.
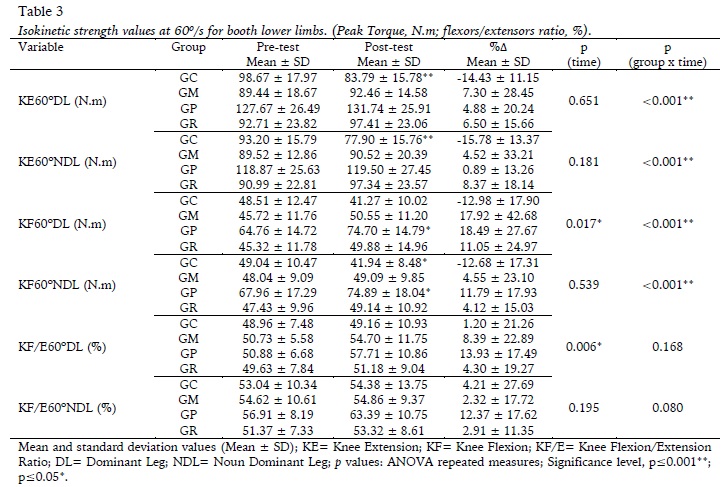
Mean and standard deviation values (Mean ± SD); KE= Knee Extension; KF= Knee Flexion; KF/E= Knee Flexion/Extension Ratio; DL= Dominant Leg; NDL= Noun Dominant Leg; p values: ANOVA repeated measures; Significance level, p≤0.001**; p≤0.05*.
The ANOVA revealed a significant effect in the group x time interaction for following isokinetic variables at 60º/s: Knee extension at 60º/s of the dominant leg (KE60DL) (F (3; 76) = 7.655, p<0.001); Knee extension at 60º/s of the noun dominant leg (KE60NDL) (F (3; 76) = 7.130, p<0.001); Knee flection at 60º/s of the dominant leg (KF60DL) (F (3; 76) = 8.619, p<0.001); and Knee flection at 60º/s of the noun dominant leg (KF60NDL) (F (3; 76) = 7.613, p<0.001). At 60º/s, it was possible to observe an alteration in all muscular groups and evaluated movements; however, no differences were observed in the hamstrings/quadriceps ratio in the evaluated limbs.
The interaction: group x time, presented significant differences between pre and post-test in a negative direction in the CG at KE60DL (14.43%; p=0.001), KE60NDL (15.78%; p=0.001) and in KF60NDL (12,68%; p=0.032). In the PG, were possible to observe significant gains in the isokinetic strength in KF60DL (18,49%; p=0.004) and KF60NDL (11,79%; p=0.041). Table 3 presents the isokinetic strength values at 60º/s for booth lower limbs (LL).
(clique para ampliar ! click to enlarge)
Discussion
The aim of this study was to assess the knee flection and extension strength after eight months of training in independent elderlies. It is possible to verify significant changes in knee flexion and extension isokinetic strength after eight months of power training in independent elderlies. However, it was also possible to observe that the control group decreased the flexion and extension knee movement in booth velocities (60º/s and 180º/s). This fact is concordant with the literature (ACSM, 2009; Wilmore & Costill, 2004); hence the strength levels decrease with age. Even more, in comparison to the group without any type of strength training program, the training programs presented significant changes in the isokinetic strength levels. Thus, a frequency of three sessions per week during eight months seems to maintain or diminish the strength levels decrease due to aging. The obtained data highlights the influence of different training programs on independent elderly women.
In the multi-component training group, no significant differences between pre and post-training program isokinetic strength were found. However, the strength levels increased, and there were also gains in the Peak Torque. To the author's best knowledge, only four studies used the multi-component training program (Carmeli et al., 2000; Carvalho et al., 2010; Rubenstein et al., 2000; Worm et al., 2001) and only one used the isokinetic test to assess the muscular strength (Carvalho et al., 2010). Carvalho et al. (2010) reported that multi-component training with two sessions per week had a limited effect on isokinetic strength. This might be due to the strength training in a multi-component program that only represents part of the exercise session. Moreover, exercise sessions based on body weight, weights, and elastic bands do not have the same specificity effect as the resistance machines. In the same study (Carvalho et al., 2010), strength exercises were combined with the elderly's multi-component training program, and both males and females improved the lower limbs isokinetic strength at booth speeds (180º/s e 60º/s). The possible lack of specificity of the generalized training in the multi-component program and the lower loads may explain the noun significant effect of this type of training in the different physical fitness components.
Carmeli et al. (2000), verified significant changes in the knee’s extensors isokinetic strength. However, the sample was composed of institutionalized elderlies. The sample characteristics may explain the differences in our study. In this work, community living female elderlies composed the sample. Probably, training adaptation may differ from elderly nursing homes. The institutionalized elderlies may have a lower baseline; thus, the subjects may obtain a higher increase due to the isokinetic strength training. The institutionalized elderlies in Carmeli at al. (2000) study, presented a strength baseline the dominant lower limb, lower than our data (i.e., KE60: 80±18 N.m vs. 89.44±18.67 N.m; KF60: 44±18 N.m vs. 45.72±11.76 N.m)
Rubenstein et al. (2000) also founded a significant isokinetic strength increase in the right knee extension at 60°/s. However, the difference was not significant when compared to the control group. The authors explained that the significant increase was due to the baseline values. The experimental group only presented a higher baseline in the right knee flexion at 60º/s in comparison to the control group. In the left knee extension at 60 º/s and booth member's flexion at 60 º/s, the baseline values were higher in the control group. Again, the authors explained that the high baseline values might explain the noun significant differences.
Considering the strength-training group (SG), the eight months of training were not enough to induce positive gains in the isokinetic strength. No differences in the peak torque or hamstrings/quadriceps ratio were founded. However, contradictory results can be found in literature, assessing the strength training effects by isokinetic evaluation (Binder et al., 2005; Carvalho et al., 2004; Galvão & Taaffe, 2005; Westhoff et al., 2000). That may be due to the strength training program intensities, which did not improve the peak torque.
Strength exercises with moderate intensity, two times per week was sufficient to increase the isokinetic strength in healthy elderlies (Carvalho et al., 2010). It was also possible to verify that the knees muscular strength increased in booth lower limbs after 16 weeks of resistance strength training (three times per week) (Westhoff et al., 2000). Binder et al. (2005) concluded that after three months of progressive strength training, the maximal knee isokinetic strength increased. Even more, Galvão and Taaffe (2005), reported that after twenty weeks of strength training, the knee extensors maximal isokinetic strength increased. Thus, independently of the variations in the training program frequency and duration, the referred studies presented a significant increase in strength levels. In comparison to our study, the differences might be explained by: (i) in this study the mean age between groups ranged from 66.30 (± 3.87) and 68.70 (± 6.51), whereas in other studies the mean age was near 75 years old; (ii) the baseline values of isokinetic strength may be influenced by the mean age; (iii) the independency level of the recruited subjects for this study can, possibly, be higher than in other studies; (iv) the strength training effects might be minimized by the baseline strength in our study due to age; (v) the strength training was not high in intensity.
The power group presented significant improvements in the strength levels over time. However, it was only possible to observe it in the noun dominant knee flexion movement at 180º/s and for booth members at 60º/s. In our research, it was not founded any study that assessed the isokinetic strength after a power training session in elderlies. Thus, it seems that power training has been less studied in elderlies and could be another option to improve physical fitness in this age group (Henwood et al., 2008). Even more, it is appointed that the power training may have a higher importance in the risk of falls prevention (Evans, 2000), and to maintain and/or improve mobility and physical fitness (Bean, Herman, et al., 2002; Bean et al., 2003; Foldvari et al., 2000).
The isokinetic muscular strength has limited improvements with different training programs. Thus, the physical education sessions prescription may include specific exercises with a different stimulus to improve muscular strength. Our study reinforces the importance of the training specificity, volume, and intensity adapted to each elderly physical fitness (ACSM, 2009; Mazzeo & Tanaka, 2001).
The statistical analysis presented a limited influence of the training programs to improve the isokinetic strength. However, the experimental groups improved or maintained strength levels over time. This trend has a higher impact when the control group is analysed. In CG, in opposition with other studies (Binder et al., 2005; Carmeli et al., 2000; Rubenstein et al., 2000; Westhoff et al., 2000; Worm et al., 2001), was observed a significant isokinetic strength decrease at 60º/s and 180º/s. These results confirm that the absence of physical exercise helps to decrease muscular strength. Otherwise, the practice of physical exercise, independently of the training program type, may maintain the strength levels in elderlies.
The main limitations of this study were: (i) Only independent females participated in this study and the results cannot be associated to community and/or institutionalized elderlies; (ii) The baseline strength values seemed to limit the training effects in the final evaluations; (iii) The literature lacks research with isokinetic evaluations after power and multi-component training protocols made difficult to compare the results of this study; (iv) The noun control of daily life physical activities, did not allow to isolate the specific effect of the different training types; (v) the independency was not assessed.
It is important to highlight that the present study related three different types of training, and the evaluations were made with isokinetic strength.
ConclusionThe power strength training, three times per week, seems to be the most effective to increase the isokinetic strength after eight months of training. The resistance and multi-component training groups did not present significant results that can be explained by the training intensity and the subjects' age. The power strength training sessions seem to be the most recommended to improve muscular strength in independent and community living elderly women.
REFERENCES
ACSM. (2006). ACSM's guidelines for exercise testing and prescription (7th Ed.). Baltimore: Lippincott Williams & Wilkins. [ Links ]
ACSM. (2009). American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Medicine & Science in Sports & Exercise, 41(3), 687-708. [ Links ]
Aquino, M. A., Leme, L. E., Amatuzzi, M. M., Greve, J. M., Terreri, A. S., Andrusaitis, F. R., & Nardelli, J. C. (2002). Isokinetic assessment of knee flexor/extensor muscular strength in elderly women. Revista do Hospital das Clínicas Universidade de São Paulo, 57(4), 131-134. [ Links ]
Arakelian, V. M., Goulart, C. da L., Mendes, R. G., Sousa, N. M. de, Trimer, R., Guizilini, S., … Borghi-Silva, A. (2019). Physiological responses in different intensities of resistance exercise-Critical load and the effects of aging process. Journal of Sports Sciences, 37(12), 1420-1428. DOI: 10.1080/02640414.2018.1561389. [ Links ]
Bean, J. F., Herman, S., Kiely, D. K., Callahan, D., Mizer, K., Frontera, W. R., & Fielding, R. A. (2002). Weighted stair climbing in mobility-limited older people: a pilot study. Journal of the American Geriatrics Society, 50(4), 663-670. [ Links ]
Bean, J. F., Kiely, D. K., Herman, S., Leveille, S. G., Mizer, K., Frontera, W. R., & Fielding, R. A. (2002). The relationship between leg power and physical performance in mobility-limited older people. Journal of the American Geriatrics Society, 50(3), 461-467. [ Links ]
Bean, J. F., Kiely, D. K., LaRose, S., O'Neill, E., Goldstein, R., & Frontera, W. R. (2009). Increased Velocity Exercise Specific to Task Training Versus the National Institute on Aging's Strength Training Program: Changes in Limb Power and Mobility. The journals of gerontology. Series A, Biological sciences and medical sciences, 64(9), 983-991. [ Links ]
Bean, J. F., Leveille, S. G., Kiely, D. K., Bandinelli, S., Guralnik, J. M., & Ferrucci, L. (2003). A comparison of leg power and leg strength within the InCHIANTI study: which influences mobility more? The journals of gerontology. Series A, Biological sciences and medical sciences, 58(8), 728-733. [ Links ]
Binder, E. F., Yarasheski, K. E., Steger-May, K., Sinacore, D. R., Brown, M., Schechtman, K. B., & Holloszy, J. O. (2005). Effects of progressive resistance training on body composition in frail older adults: results of a randomized, controlled trial. The journals of gerontology. Series A, Biological sciences and medical sciences, 60(11), 1425-1431. [ Links ]
Borg, G. (1998). Borg's Perceived Exertion and Pain Scales. Champaign, IL: Human Kinetics, 1998.
Cadore, E. L., Pinto, R. S., Bottaro, M., & Izquierdo, M. (2014). Strength and endurance training prescription in healthy and frail elderly. Aging and Disease, 5(3), 183-195. DOI: 10.14336/AD.2014.0500183. [ Links ]
Carmeli, E., Reznick, A. Z., Coleman, R., & Carmeli, V. (2000). Muscle Strength and Mass of Lower Extremities in Relation to Functional Abilities in Elderly Adults. Gerontology, 46(5), 249-257. [ Links ]
Carrasco-Poyatos, M., Rubio-Arias, J. A., Ballesta-García, I., & Ramos-Campo, D. J. (2019). Pilates vs. muscular training in older women. Effects in functional factors and the cognitive interaction: A randomized controlled trial. Physiology & Behavior, 201, 157-164. [ Links ]
Carvalho, J., Marques, E., Soares, J. M., & Mota, J. (2010). Isokinetic strength benefits after 24 weeks of multi-component exercise training and a combined exercise training in older adults. Aging Clinical and Experimental Research, 22(1), 63-69. [ Links ]
Carvalho, J., Oliveira, J., Magalhães, J., Ascensão, A., Mota, J., & Soares, J. M. C. (2004). Força muscular em idosos II: efeitos de um programa complementar de treino de força muscular de idosos de ambos os sexos. Revista Portuguesa de Ciências do Desporto, 4(1), 58-65. [ Links ]
Carvalho, M. J., Marques, E., & Mota, J. (2009). Training and detraining effects on functional fitness after a multi-component training in older women. Gerontology, 55(1), 41-48. [ Links ]
Chodzko-Zajko, W. J., Proctor, D. N., Singh, M. A. F., Minson, C. T., Nigg, C. R., Salem, G. J., & Skinner, J. S. (2009). Exercise and physical activity for older adults. Medicine & science in sports & exercise, 41(7), 1510-1530. [ Links ]
Cress, M. E., & Meyer, M. (2003). Maximal voluntary and functional performance levels needed for independence in adults aged 65 to 97 years. Physical Therapy, 83(1), 37-48. [ Links ]
de Vos, N. J., Singh, N. A., Ross, D. A., Stavrinos, T. M., Orr, R., & Singh, M. A. F. (2005). Optimal load for increasing muscle power during explosive resistance training in older adults. Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 60(5), 638-647. [ Links ]
Evans, W. J. (2000). Exercise strategies should be designed to increase muscle power. Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 55(6), M309-310. [ Links ]
Foldvari, M., Clark, M., Laviolette, L. C., Bernstein, M. A., Kaliton, D., Castaneda, C., Pu, C. T., Hausdorff, J. M., Fielding, R. A., & Singh, M. A. (2000). Association of muscle power with functional status in community-dwelling elderly women. Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 55(4), M192-199. [ Links ]
Frontera, W. R., Hughes, V. A., Fielding, R. A., Fiatarone, M. A., Evans, W. J., & Roubenoff, R. (2000). Aging of skeletal muscle: a 12-yr longitudinal study. Journal of Applied Physiology, 88(4), 1321-1326. [ Links ]
Galvão, D. A., & Taaffe, D. R. (2005). Resistance Exercise Dosage in Older Adults: SingleVersus Multiset Effects on Physical Performance and Body Composition. Journal of the American Geriatrics Society, 53(12), 2090-2097. [ Links ]
Greenlund, L. J., & Nair, K. S. (2003). Sarcopenia-consequences, mechanisms, and potential therapies. Mechanisms of Ageing and Development, 124(3), 287-299. [ Links ]
Henwood, T. R., & Taaffe, D. R. (2005). Improved physical performance in older adults undertaking a short-term programme of high-velocity resistance training. Gerontology, 51(2), 108-115. [ Links ]
Henwood, T. R., Riek, S., & Taaffe, D. R. (2008). Strength versus muscle power-specific resistance training in community-dwelling older adults. Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 63(1), 83-91. [ Links ]
Hurley, B. F., & Roth, S. M. (2000). Strength training in the elderly: effects on risk factors for age-related diseases. Sports Medicine, 30(4), 249-268. [ Links ]
Maroco, J. (2007). Análise estatística - Com utilização do SPSS. Edição Sílabo, Lda. Lisboa.
Marsh, A. P., Miller, M. E., Rejeski, W. J., Hutton, S. L., & Kritchevsky, S. B. (2009). Lower Extremity Muscle Function After Strength or Power Training in Older Adults. Journal of Aging and Physical Activity, 17(4), 416-443. [ Links ]
Marsh, A. P., Miller, M. E., Saikin, A. M., Rejeski, W. J., Hu, N., Lauretani, F., Bandinelli, S., Guralnik, J. M., & Ferrucci, L. (2006). Lower extremity strength and power are associated with 400-meter walk time in older adults: The InCHIANTI study. Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 61(11), 1186-1193. [ Links ]
Mazzeo, R. S., & Tanaka, H. (2001). Exercise prescription for the elderly: current recommendations. Sports Medicine, 31(11), 809-818. [ Links ]
McNeil, C. J., Vandervoort, A. A., & Rice, C. L. (2007). Peripheral impairments cause a progressive age-related loss of strength and velocity-dependent power in the dorsiflexors. Journal of Applied Physiology, 102(5), 1962-1968. [ Links ]
McPhee, J. S., Cameron, J., Maden-Wilkinson, T., Piasecki, M., Yap, M. H., Jones, D. A., & Degens, H. (2018). The contributions of fibre atrophy, fibre loss, in situ specific force and voluntary activation to weakness in sarcopenia. Journals of Gerontology, Series A, 73(10), 1287-1294. [ Links ]
Moran, J., Ramirez-Campillo, R., & Granacher, U. (2018). Effects of Jumping Exercise on Muscular Power in Older Adults: A Meta-Analysis. Sports Medicine (Auckland, N.Z.), 48(12), 2843-2857. DOI: 10.1007/s40279-018-1002-5. [ Links ]
Nelson, M. E., Layne, J. E., Bernstein, M. J., Nuernberger, A., Castaneda, C., Kaliton, D., Hausdorff, J., Judge, J. O., Buchner, D. M., Roubenoff, R., & Fiatarone Singh, M. A. (2004). The effects of multidimensional home-based exercise on functional performance in elderly people. Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 59(2), 154-160. [ Links ]
Orr, R., de Vos, N. J., Singh, N. A., Ross, D. A., Stavrinos, T. M., & Fiatarone-Singh, M. A. (2006). Power training improves balance in healthy older adults. Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 61(1), 78-85. [ Links ]
Puggaard, L. (2003). Effects of training on functional performance in 65, 75 and 85 year-old women: Experiences deriving from community based studies in Odense, Denmark. Scandinavian Journal of Medicine & Science in Sports, 13(1), 70-76. [ Links ]
Reid, K. F., & Fielding, R. A. (2012). Skeletal muscle power: a critical determinant of physical functioning in older adults. Exercise and sport sciences reviews, 40(1), 4. [ Links ]
Rubenstein, L. Z., Josephson, K. R., Trueblood, P. R., Loy, S., Harker, J. O., Pietruszka, F. M., & Robbins, A. S. (2000). Effects of a group exercise program on strength, mobility, and falls among fall-prone elderly men. Journals of Gerontology Series A, Biological Sciences and Medical Sciences, 55(6), M317-321. [ Links ]
Suetta, C., Aagaard, P., Rosted, A., Jakobsen, A. K., Duus, B., Kjaer, M., & Magnusson, S. P. (2004). Training-induced changes in muscle CSA, muscle strength, EMG, and rate of force development in elderly subjects after long-term unilateral disuse. Journal of Applied Physiology, 97(5), 1954-1961. [ Links ]
Suetta, C., Magnusson, S. P., Rosted, A., Aagaard, P., Jakobsen, A. K., Larsen, L. H., Duus, B., & Kjaer, M. (2004). Resistance training in the early postoperative phase reduces hospitalization and leads to muscle hypertrophy in elderly hip surgery patients-a controlled, randomized study. Journal of the American Geriatrics Society, 52(12), 2016-2022. [ Links ]
Toraman, N. F., Erman, A., & Agyar, E. (2004). Effects of multi-component training on functional fitness in older adults. Journal of Aging and Physical Activity, 12(4), 538-553. [ Links ]
Traczyk, A., Kuźba, K., Chłystek, J., Potyra, K., Abramczyk, A., & Łakomski, M. (2018). Resistance training for the elderly. Review of the literature. Journal of Education, Health and Sport, 8(9), 1048-1057. [ Links ]
Vandervoort, A. A. (2002). Aging of the human neuromuscular system. Muscle Nerve, 25(1), 17-25. [ Links ]
Westhoff, M. H., Stemmerik, L., & Boshuizen, H. C. (2000). Effects of a Low-Intensity Strength-Training Program on Knee-Extensor Strength and Functional Ability of Frail Older People. Journal of Aging and Physical Activity, 8(4), 325-342. DOI: 10.1123/japa.8.4.325. [ Links ]
Wilk, K. (1991). Isokinetic Testing - Setup and Positioning. In Biodex System II Manual, Applications/Operations. Biodex Medical System, Inc, New York, USA. [ Links ]
Wilmore, J. H., & Costill, D. L. (2004). Physiology of Sport and Exercise. Champaign, IL: Human Kinetics.
Worm, C. H., Vad, E., Puggaard, L., Stovring, H., Lauritsen, J., & Kragstrup, J. (2001). Effects of a multi-component exercise program on functional ability in community-dwelling, frail older adults. Journal of Aging and Physical Activity, 9, 414-424. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
[*] Instituto Politécnico de Bragança, Campus de Santa Apolónia, 5301 - 856 Bragança. Email: mmonteiro@ipb.pt
Acknowledgments: Nothing to declare.
Conflict of interests: Nothing to declare.
Funding: This study was supported by the Portuguese Foundation for Science and Technology (FCT) to the Research Center in Physical Activity, Health and Leisure (CIAFEL) (FCT/UID/DTP/00617/2019) to the Body&Brain Project (FCT/PTDC/SAUDES/31808/2017) and by the Instituto Português do Desporto e Juventude (IPDJ).
Manuscript received at January 11h 2019; Accepted at June 15th 2019

