










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMotricidade
versão impressa ISSN 1646-107X
Motri. vol.14 no.2-3 Ribeira de Pena out. 2018
https://doi.org/10.6063/motricidade.10890
ARTIGOS DE REVISÃO
Reference values for Cobb angles when evaluating the spine in the sagittal plane: a systematic review with meta-analysis
Tássia Silveira Furlanetto1[*], Juliana Adami Sedrez1, Cláudia Tarragô Candotti1, Jefferson Fagundes Loss1
1 Universidade Federal do Rio Grande do Sul, Rio Grande do Sul, Brasil
ABSTRACT
The present systematic review of observational studies with meta-analysis aim to identify the reference values of the spinal curvatures in the sagittal plane, as evaluated using the Cobb angle in X-rays, in healthy individuals. Electronic searches were undertaken in MEDLINE, Scopus, ScienceDirect and LILACS. Studies that evaluated the spinal curvature of healthy children, adolescents, adults, and elderly using Cobb method and presented reference values for those curvatures were incluced. Thirty-one studies were eligible for inclusion. The reference values found (confidence interval 95%) were: for children, thoracic (28.7°-37.9°), lumbar L1-L5 (34.5o-44.8º), and lumbar L1-S1 (41.7o-54.1o); for adolescents: thoracic (31.5o-39.2o), lumbar L1-L5 (39.8o-45.6o), and lumbar L1-S1 (51.9o-59.1o); for adults: thoracic (33.7o-40.3o), lumbar L1-L5 (38.1o-45.6o), and lumbar L1-S1 (54.2o-61.7o); and for the elderly: thoracic (37.7º-50.4o), and lumbar L1- S1 (56.6º-65.9o). For the cervical region, it was impossible to establish consistent reference values. The present study supports that precise reference intervals were identified for the sagittal curvatures of the thoracic and lumbar spine in healthy children, adolescents, adults and elderly, as evaluated by means of the Cobb Method.
Keywords: kyphosis, lordosis, radiograph, reference values.
Introduction
In individuals without musculoskeletal dysfunction and apparently healthy, the spine is usually structured by successive opposed convexities in the sagittal plane (Perriman et al., 2010). The magnitude of each curve varies from individual to individual, however, when maintaining the upright position, they should result from a balance of muscular forces and external loads (Singh, Bailey & Lee, 2010). An accentuated curvature may cause the intervertebral disks to protrude, while an excessively straight spine may lead to overload on “articular facets” (Singh, Bailey & Lee, 2010). Thus, the spine should be neither excessively curved nor straight, but within a range of normality. Based on values that quantify the deviation and its progression (for example, increasing spinal curvature), quantitative postural evaluation procedures are used to identify subtle alterations to the spinal curvature or accompany treatment (Oliveira et al., 2012).
The sagittal curvature of the spine can be measured using several invasive and/or non- invasive postural evaluation methods. The gold standard evaluation method for the sagittal plane is the latero-lateral X-ray (Zaina, Donzelli, Lusini & Negrini, 2012), in which the Cobb angles, represented by the crossing of tangents originating from the cranial and caudal vertebral bodies, are calculated (Briggs et al., 2007; Goh, Price, Leedman & Singer, 2000).
Regarding the range of normality, the literature is extremely divergent. For example, in the lumbar spine, the range of normality is found to vary from 26° to 58° Cobb-angle (Prospst- Proctor & Blac, 1983), or from 13° to 78° Cobb- angle (Bernhardt & Bridwell, 1989). Thus, the range of sagittal spinal curvature considered to be within the normal range when measured using the Cobb method is very wide, varying by up to 60° (Briggs et al., 2007; Chaise et al., 2011; Goh et al., 2000; Oliveira et al., 2012; Zaina et al., 2012). Hence, the absence of adequate parameters may compromise the diagnosis and, consequently, the feasibility of effective intervention (Zubovic, Davies, Berryman & Pynsent, 2008).
It should be noted that this broad spectrum of normal curvature values is due to the variability of the human being, while also being dependent on, for example, age range and the vertebral bodies considered when calculating the curvature. Therefore, it would be useful to objectively synthetize the normal values arising from studies that have adopted the Cobb measurement in healthy individuals. Moreover, in clinical practice, the definition of a narrower range of normality, mainly for children and adolescents, would increase the chances of early diagnosis and might improve preventive strategies and interventions (Monticone et al., 2014).
Therefore, based on a systematic review with meta-analysis, this study aims to identify the reference values of the spinal curvature in the sagittal plane, as evaluated using the Cobb angle in X-rays, in healthy individuals.
METHOD
Identification and selection of studies
A systematic review with meta-analysis of observational studies presenting reference values of the sagittal curvature of the spine, determined using the Cobb angle in X-rays was conducted. This systematic review followed the recommendations proposed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher, Liberati, Tetzlaff & Altman, 2009). The Project was registered in the PROSPERO of the Centre for Reviews and Dissemination at the University of York (http://www.crd.york.ac.uk/PROSPERO), under the number CRD42015025691.
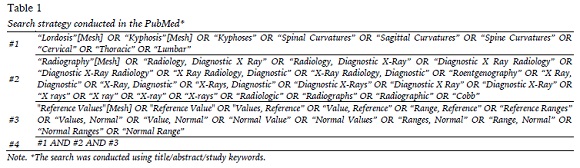
A systematic search was carried out by two independent investigators and in duplicate for studies in the following databases: MEDLINE (Medical Literature Analysis and Retrieval System Online) accessed by PubMed; Scopus; ScienceDirect; and LILACS (Literatura Latino- Americana e do Caribe em Ciências da Saúde) accessed by BVS (Biblioteca Virtual em Saúde), in the month of June 2016. The search strategy adopted in the PubMed data base is presented in Table 1. No year of publication restriction was used in the systematic search. The studies should be written in English, Spanish or Portuguese.
The PICO model was adopted to establish the inclusion criteria, where the “P” (Patient, Population, or Problem) is defined as children, adolescents, adults and the elderly; the “I” (Intervention, Prognostic Factor, or Exposure) is the sagittal curvature assessment based on applying the Cobb method to X-ray images; the “C” (Comparison or Intervention) is not applicable to this review; and the “O” (Outcome) is the range of normal values regarding the sagittal curvature of the cervical, thoracic and lumbar spine.
Thus, the inclusion criteria were studies that:
1) evaluated the spinal curvature using the two- or four-line Cobb method; 2) evaluated the sagittal curvatures of the spine (lumbar, thoracic or cervical); and 3) presented reference values for those curvatures. The exclusion criteria were studies that: 1) solely revised the literature; and 2) evaluated non-healthy populations with specific pathologies.
The titles and abstracts of the studies identified using the search strategy were independently assessed in duplicate by two investigators (T.S.F and J.A.S). Those studies in which the abstracts contained sufficient information regarding the inclusion and exclusion criteria were selected for full evaluation of the article. In the second stage, the same investigators, independently and in duplicate, assessed the full texts and made the selection according to the eligibility criteria. Disagreements between investigators were resolved by consensus, and when disagreements persisted, a third investigator (C.T.C.) evaluated the article. In addition, the reference sections of the selected studies were checked in an attempt to find suitable studies not revealed by the electronic search.
Assessment of characteristics of studies
Two investigators (T.S.F. and J.A.S.), independently and in duplicate, extracted the data referring to the methodological characteristics and findings, and evaluated the risk of bias. Disagreements were resolved by consensus or by a third investigator (C.T.C.). Using a standard form, the following information was extracted: spine regions assessed, level used to calculate the Cobb angle, assessed population and reference values reported for spinal curvatures.
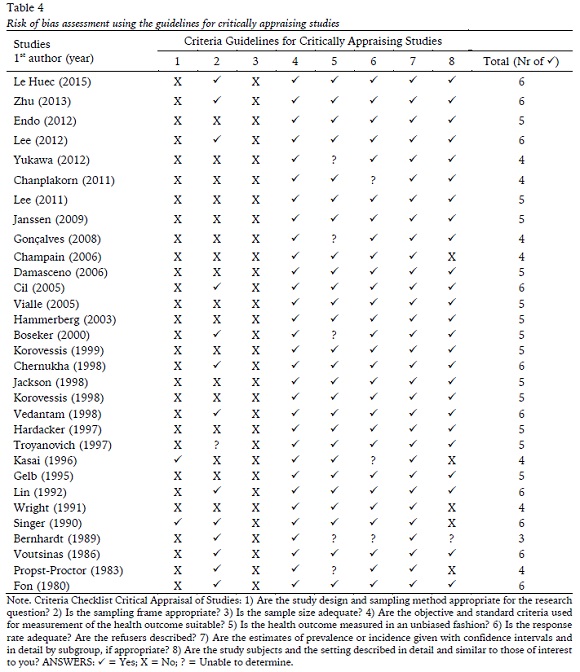
The studies that fulfilled the inclusion criteria were assessed regarding risk of bias using the Guidelines for Critically Appraising Studies, which consists of a check list of 8 criteria that can be answered “yes”, “no” or “impossible to determine” (Loney, Chambers, Bennett, Roberts & Stratford, 1998). This checklist was developed and validated to critically appraise research studies that estimate the prevalence or incidence of a disease or health problem (Loney et al., 1998), and investigates three main areas: 1) the internal validity (design, sampling frame, sample size, outcome measures, measurement and response rate); 2) the interpretation of the results; and 3) the applicability of the findings. The risk of bias of the studies is presented according to the total number of criteria classified as “yes” in each article. Each criterion was given a point and each study was scored out of a total of eight (Davoren, Demant, Shiely & Perry, 2016).
Data analysis
To better organize the extracted data, with a view to the meta-analysis, the studies were grouped according to the assessed population: children (under 12 years), adolescents (between 12 and 17 years), adults (between 18 and 59 years) and the elderly (60 plus). Also, in the lumbar region, the studies were grouped according to the vertebral levels used in the evaluation of the Cobb angle: between vertebra L1 and L5, and between vertebra L1 and S1. This division according to vertebra levels in lumbar spine came about because the Cobb angles calculated based on a sacral vertebra presented a considerable discrepancy in relation to those calculated based on lumbar vertebrae. The large inclination of the sacrum in relation to lumbar vertebrae is mainly responsible for this discrepancy (Marty et al., 2002). Thus, the groups were: 1) Cervical Children, 2) Cervical Adolescents, 3) Cervical Adults, 4) Cervical Elderly, 5) Thoracic Children, 6) Thoracic Adolescents, 7) Thoracic Adults, 8) Thoracic Elderly, 9) Lumbar Children L1-L5, 10) Lumbar Children L1-S1, 11) Lumbar Adolescents L1-L5, 12) Lumbar Adolescents L1-S1, 13) Lumbar Adults L1-L5, 14) Lumbar Adults L1-S1, 15) Lumbar Elderly L1-L5, and 16) Lumbar Elderly L1-S1.
The Comprehensive Meta-Analysis software (CMA, www.metaanalysis.com) was used in the meta-analysis. The studies were grouped according to the assessed population and, only in the case of lumbar curvature, the level of the vertebra used to evaluate the Cobb angle. The means and 95% confidence intervals (CI) were calculated for the angles of the cervical, thoracic and lumbar curvatures with random effect models for the different populations. The Z test was used to evaluate the statistical significance of the means and the confidence interval for the analyzed curvatures. The significance value of 0.05 was adopted.
The statistical heterogeneity for each meta- analysis was assessed using the Cochran Q test and inconsistency test I2. For the purpose of interpretation, an I2 value close to 0% indicates no heterogeneity among the studies, close to 25% indicates low heterogeneity, close to 50% indicates moderate heterogeneity, and close to 75% indicates high heterogeneity among the studies (Higgins & Thompson, 2002; Higgins, Thompson, Deeks & Altman, 2003).
RESULTS
Flow of studies through the review
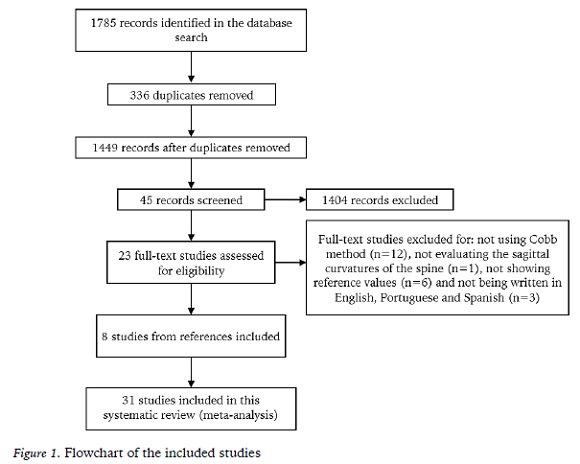
Of the 1785 potentially relevant studies recovered from the electronic data bases and found in the references, 31 met the inclusion criteria (Figure 1).
Characteristics of studies
Table 2 summarizes the main features of the included studies: age, number of subjects and the protocols for the X-ray examination and Cobb angle calculation. In relation to age, most of the studies assessed young adults, while the least assessed population was the elderly. The good reproducibility of the two- or four-line Cobb method was confirmed in most of analyzed studies.
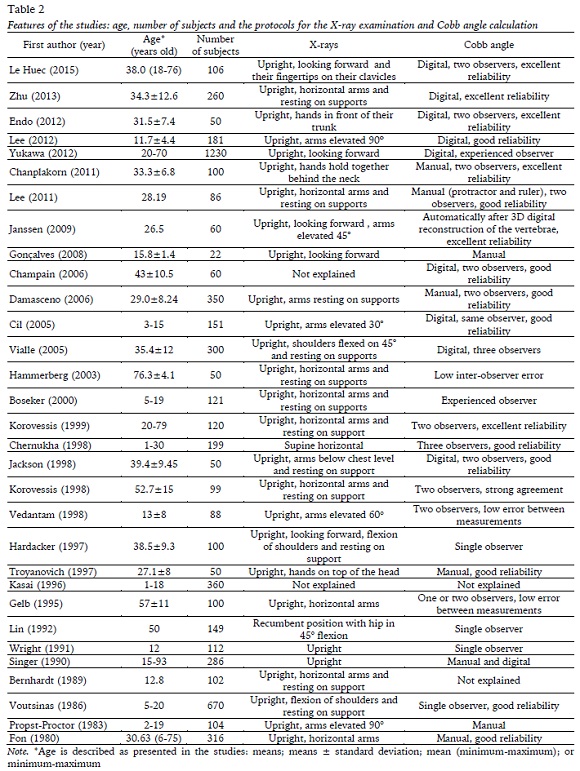
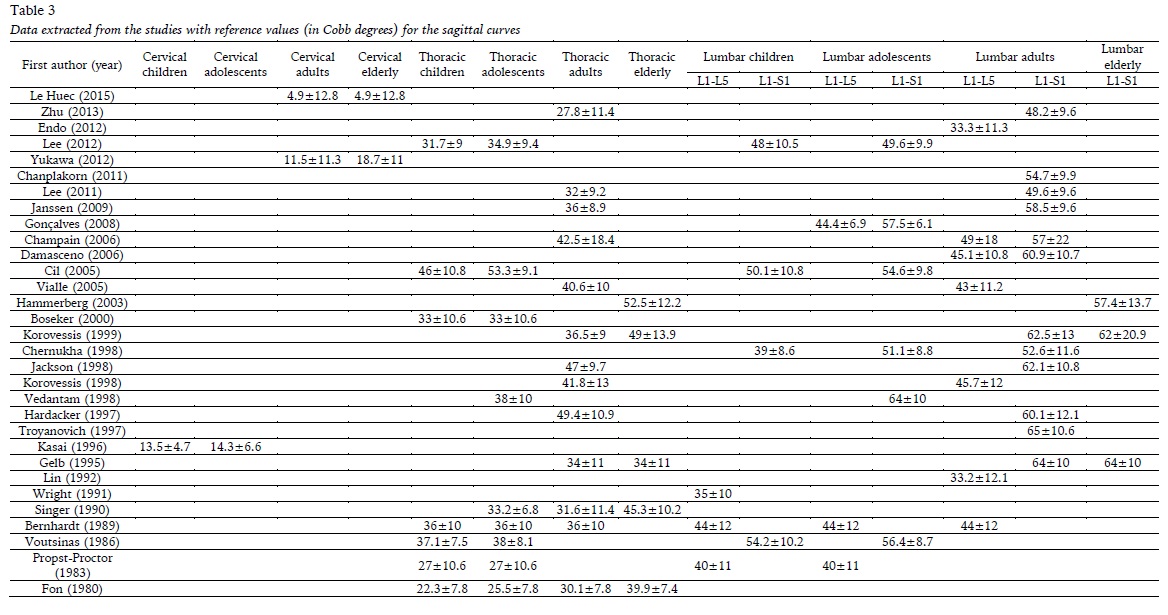
Table 3 shows the reference values (in Cobb degrees) of the sagittal curves. Few studies assessed the cervical curvature, with only one study being found involving children and adolescents (Kasai, Ikata, Katoh, Miyake & Tsubo, 1996). Therefore, it was not considered in the meta-analysis. The lumbar curvature of the elderly population was only assessed using L1-S1 vertebral levels. Therefore, in the elderly, vertebral level L1-L5 was not used in the meta- analysis. In general, the Cobb angles calculated on basis of the sacral vertebra (L1-S1) are greater than those calculated on lumbar vertebrae alone (L1-L5). This issue is raised in the studies by Champain et al. (2006) and Damasceno et al. (2006) which analyze the same sample using different methods (Table 3).
(clique para ampliar ! click to enlarge)
Risk of bias in included studies
In the risk of bias assessment (Table 4), the criteria that involve measurement issues (criterion 4) and confidence intervals (criterion 7) were found in all the included studies. In 28 studies (90.3%), the response rate was adequate (criterion 6); in 26 studies (83.9%) there are no unbiased assessors (criterion 5); and 25 studies (80.6%) presented detailed subject descriptions (criterion 8). Only 13 studies (40.3%) presented an unbiased sampling frame (criterion 2) and 2 studies (6.4%) presented a random sample (criterion 1). None of the studies scored in the third scale criterion (sample size), because they did not provide a sample size calculation or justification.
Meta-analyses of Exposure
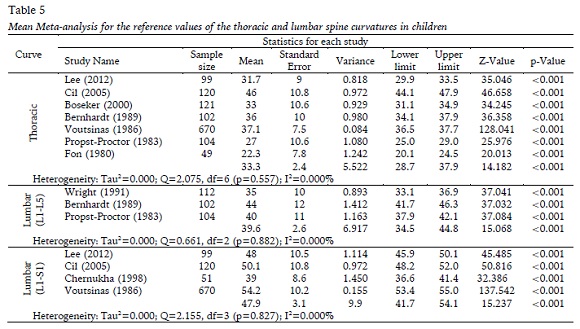
The meta-analysis of the child population presents the mean of the results found in the literature for the Cobb values of the thoracic and lumbar curves and the 95% CI (Table 5). None of the meta-analyses carried out for the sagittal curves presented heterogeneity. In the thoracic spine, the z value was 14.182 (p<0.001), while in the lumbar spine, the z values were 15.068 (p<0.001) and 15.237 (p<0.001), demonstrating that the means and confidence intervals of the reference values for both curvatures are statistically significant in children.
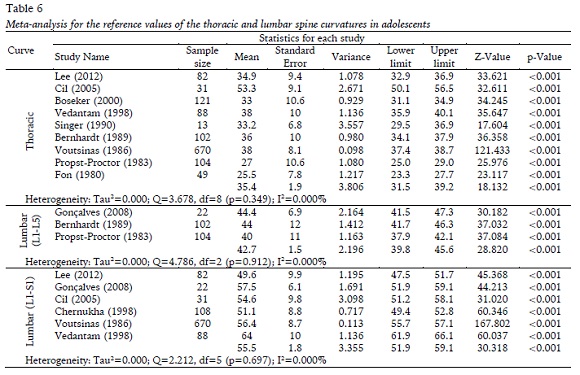
The meta-analysis of the adolescents presents the mean of the results found in the literature for the Cobb values of the thoracic and lumbar curves and the 95% CI (Table 6). None of the meta- analyses carried out for the sagittal curves presented heterogeneity. In the thoracic spine, the z value was 18.132 (p<0.001), while in the lumbar spine, the z values were 28.820 (p<0.001) and 30.318 (p<0.001), demonstrating that the means and confidence intervals of the reference values for both curvatures are statistically significant in adolescents.
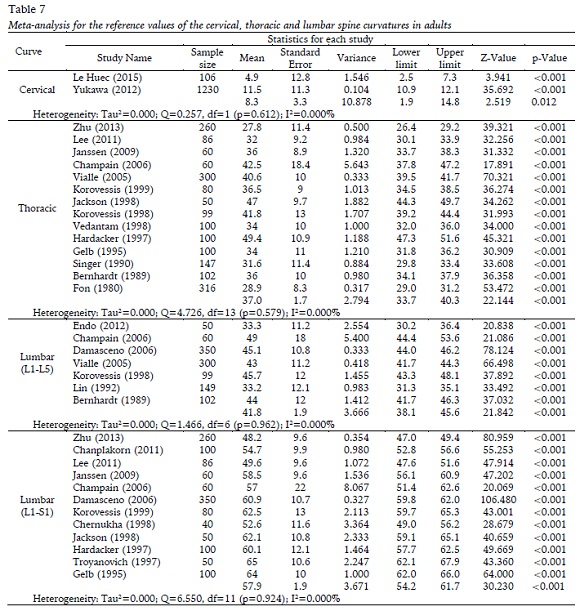
The meta-analysis of the adult population presents the mean results for the Cobb values of the cervical, thoracic and lumbar curves and the 95% CI (Table 7). None of the meta-analyses presented heterogeneity. In the cervical spine, the z value was 2.519 (p=0.012) and in the thoracic spine, the z value was 22.144 (p<0.001). While in the lumbar spine, the z values were 21.842 (p<0.001) and 30.230 (p<0.001), demonstrating that the means and confidence intervals of the reference values for the curvatures are statistically significant in adults.
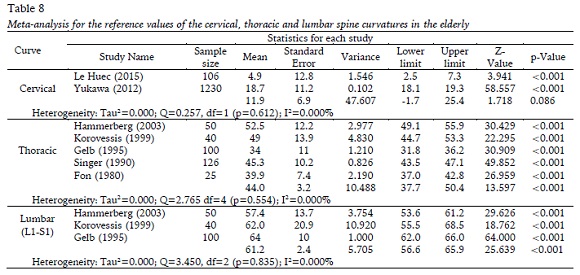
The meta-analysis of the elderly population presents the mean results for the Cobb values of the curves and the 95% CI (Table 8). None of the meta-analyses presented heterogeneity. In the thoracic spine, the z value was 13.597 (p<0.001), while in the lumbar spine, the z value was 25.639 (p<0.001), demonstrating that the means and confidence intervals of the reference values for curvatures are statistically significant in the elderly. By contrast, in the cervical spine, the z value was 1.718 (p=0.086), which demonstrates that the mean and the confidence interval of the normality values are not statistically significant.
DISCUSSION
One significant contribution of the present study, besides the systematization of the results presented in the literature, is the presentation of the intervals of normality organized according to the age of the assessed individuals in relation to each region of the spine. The lumbar curvature was the most frequently investigated, followed by the thoracic curvature. Few studies (Kasai et al., 1996; Le Huec, Demezon & Aunoble, 2015; Yukawa, Kato, Suda, Yamagata & Ueta, 2012) have attempted to evaluate the cervical spine, therefore the results are inconsistent.
The literature reports that, on average, the normal thoracic curvature is 40º (Harrison, Harrison, Troyanovich & Harmon, 2000), while that of the lumbar curvature ranges from 45º to 50º (Damasceno, Catarin, Campos & Defino, 2006), with some variation according to the population investigated. However, in general, the studies show highly variable results, with wide confidence intervals (Table 3), compromising the classification process. It can be seen that most of the studies have standard deviations greater than 10º, which results in a high 95% CI, with around 40º of variability. The result of this meta-analysis for the thoracic and lumbar curvatures is associated with the most restricted confidence interval, around 10º of variability, in the different vertebral levels and populations (Table 5 - Table 8). In fact, when a wide range of normality is used in the assessment, there is a greater chance of an individual, who in fact requires treatment, being considered normal. This situation is particularly undesirable in children and adolescents who would benefit from early diagnosis and treatment. On the other hand, a narrow range of normal values, might lead to the indication of unnecessary treatment. It should be noted that an adequate diagnosis and/or follow-up depends not only on the information regarding the angles of the spine, but also on the knowledge of the spine’s morphology, kinesiology and biomechanics. Thus, we understand that, the narrow range identified in the present meta- analysis could help clinicians to better classify the individuals within a normal range and adequately monitor treatment effects.
The results of the meta-analysis show an increase in the average thoracic and lumbar curvatures which occurs with aging, reaching the highest averages in the elderly (44º in the thoracic curvature and 61º in the lumbar curvature). These findings corroborate those in the literature which show a tendency towards postural flexion in the elderly, with consequent increase in the magnitude of the sagittal curvatures in the vertebral column, due to the increased degeneration of the intervertebral disks (Benedetti, Berti, Presti, Frizziero & Giannini, 2008).
Regarding the cervical curvature, the result of the meta-analysis was inconsistent. In the elderly, the results for the cervical spine were not statistically significant, and the normality interval encompassed a range from cervical kyphosis, indicated by the negative sign (-1.7º), to cervical lordosis, indicated by the positive sign (25.4º). In adults, despite the results being significant, the range was rather more limited (1.9º-14.8º), while the signal was always positive. Even so, there is a great variability in the magnitude of the curvature.
Physiologically, the cervical spine has a lordotic curvature (Harrison, Janik, Troyanovich & Holland, 1996) and the normal alignment of cervical lordosis is one of the most important factors for the movement and function of this region (Miyazaki et al., 2008). Moreover, the loss of normal lordosis may induce pathological changes and accelerate the degeneration of the cervical spine (Miyazaki et al., 2008), as well as cause headaches (Nagasawa, Sakakibara &Takahashi, 1993) and neckaches (Harrison et al., 2004; Miyazaki et al., 2008). Therefore, given the morphological nature of the cervical lordotic curvature, the normality values indicated for adults and the elderly by the meta-analysis appear to inadequately represent this region of the spine. Hence, it is suggested that more studies be conducted with the aim of identifying a reference interval of normality indicated for the cervical spine in different age groups.
When analyzing our findings, some limitations should be taken into account. One of which is inherent to the adopted search method, which is based exclusively on electronic data bases and in the English, Spanish and Portuguese languages, which may have failed to identify possibly eligible studies. It is important to point out that, although the included studies meet the vast majority of criteria used to evaluate risk bias, criterion 3 (sample size) was not met by any of studies, and criterion 1 (random sample) was only met by two studies. Considering the intrinsic variability of spinal curvatures, the failure to meet these criteria may explain why the studies individually present a wide range of normality. Thus, by gathering these results systematically and compiling them according to the adopted methodologies, we were able to significantly reduce the range of normality.
It should be noted that important methodological differences exist between the included studies, for example: most of the studies involving evaluation of the thoracic region report shoulder positioning close to 90º of flexion. However, there are studies that refer to shoulders positioned at 60º (Vedantam, Lenke, Keeney & Bridwell, 1998), and between 30º and 45º (Cil et al., 2005; Jackson, Peterson, McManus & Hales, 1998; Korovessis, Stamatakis & Baikousis, 1998; Vialle et al., 2005), while there are even studies that fail to mention the position of shoulders (Boseker, Moe, Winter & Koop, 2000; Champain et al., 2006; Gelb, Lenke, Bridwell, Blanke, McEnery, 1995; Korovessis et al., 1998; Singer, Jones & Breidahl, 1990; Voutsinas & MacEwen, 1986). It is believed that this positioning, as well as the support or otherwise of the arms on some surface, may alter the angle of thoracic kyphosis, leading to variation in the results.
When referring to the assessments of the lumbar region, important differences are also found, with most studies conducting X-ray examinations with the patient in the upright position. However, there are reports of examinations conducted with the patients in the supine (Chernukha, Daffner & Reigel, 1998) and dorsal decubitus (Lin, Jou &Yu, 1992) positions, as well as studies that do not report the patient’s position (Champain et al., 2006). Therefore, when the objective of the examination is to measure the spinal curvature, placing the subject in the upright position is recommended in order to minimize the variability inherent in the clinical examination.
CONCLUSION
Based on the present systematic review with meta-analysis, it was possible to identify a narrow interval of reference values for the thoracic and lumbar curvatures of the spine for healthy children, adolescents, adults and the elderly, assessed using the Cobb method with X-rays. For the cervical spine, the reference values were inconsistent due to the large variability between studies, which warrants further research.
REFERENCES
Benedetti, M. G., Berti L., Presti, C., Frizziero, A., & Giannini, S. (2008). Effects of an adapted physical activity program in a group of elderly subjects with flexed posture: clinical and instrumental assessment. Journal of Neuroengineerring Rehabilitation, 5(32), 1-11. https://doi.org/10.1186/1743-0003-5-32. [ Links ]
Bernhardt, M., & Bridwell, K. H. (1989). Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines. Spine, 14(7), 717-721. https://doi.org/10.1097/00007632-198907000-00012 [ Links ]
Boseker, E. H., Moe, J. H., Winter, R. B., & Koop, S. E. (2000). Determination of “normal” thoracic kyphosis: a roentgenographic study of 121 “normal” children. Journal of Pediatric Orthopaedics, 20(6),796-798. https://doi.org/10.1097/01241398-200011000-00019
Briggs, A. M., Wrigley, T.V., Tully, E. A., Adams, P.E., Greig, A. M., & Bennel, K. L. (2007). Radiographic measures of thoracic kyphosis in osteoporosis: Cobb and vertebral centroid angles. Skeletal Radiology, 36(8), 761-767. https://doi.org/10.1007/s00256-007-0284-8 [ Links ]
Chaise, F. O., Candotti, C. T., La Torre, M., Furlanetto,T. S., Pelinson, P. P., & Loss, J. F. (2011). Validation, repeatability and reproducibility of a noninvasive instrument for measuring thoracic and lumbar curvature of the spine in the sagittal plane. Brazilian Journal of Physical Therapy, 15(6), 511-517. https://doi.org/10.1590/s1413-35552011005000031 [ Links ]
Champain, S., Benchikh, K., Nogier, A., Mazel, C., Guise, J. D., & Skalli, W. (2006). Validation of new clinical quantitative analysis software applicable in spine orthopaedic studies. European Spine Journal, 15(6), 982-991. https://doi.org/10.1007/s00586-005-0927-1 [ Links ]
Chanplakorn, P., Wongsak, S., Woratanarat, P., Wajanavisit, W., & Laohacharoensombat, W. (2011). Lumbopelvic alignment on standing lateral radiograph of adult volunteers and the classification in the sagittal alignment of lumbar spine. European Spine Journal, 20(5), 706-712. https://doi.org/10.1007/s00586-010-1626-0 [ Links ]
Chernukha, K. V., Daffner, R. H., & Reigel, D. H.(1998). Lumbar lordosis measurement. A new method versus Cobb technique. Spine, 23(1), 74- 79. https://doi.org/10.1097/00007632-199801010-00016 [ Links ]
Cil, A., Yazici, M., Uzumcugil, A., Kandemir, U., Alanay, A., Alanay, Y., … & Surat, A. (2005). The evolution of sagittal segmental alignment of the spine during childhood. Spine, 30(1), 93-100. https://doi.org/10.1097/01.brs.0000149074.21550.32
Damasceno, L. H. F., Catarin, S. R. G., Campos, A. D.,& Defino, H. L. A. (2006). Lumbar Lordosis: a study of angle values and of vertebral bodies and intervertebral discs role. Acta Ortopédica Brasileira, 14(4), 193-198. https://doi.org/10.1590/S1413-78522006000400003 [ Links ]
Davoren, M. P., Demant, J., Shiely, F., & Perry, I. J. (2016). Alcohol consumption among university students in Ireland and the United Kingdom from 2002 to 2014: a systematic review. BMC Public Health, 16(173). https://doi.org/10.1186/s12889-016-2843-1 [ Links ]
Endo, K., Suzuki, H., Nishimura, H., Tanaka, H., Shishido, T., & Yamamoto, K. (2012). Sagittal lumbar and pelvic alignment in the standing and sitting positions. Journal of Orthopaedic Science, 17(6), 682-686. https://doi.org/10.1007/s00776-012-0281-1 [ Links ]
Fon, G., Pitt, M. J., & Thies Jr, A. C. (1980). Thoracic kyphosis: range in normal subjects. American Journal of Roentgenology, 134(5), 979-983. https://doi.org/10.2214/ajr.134.5.979 [ Links ]
Gelb, D. E., Lenke, L. G., Bridwell, K. H., Blanke, K., & McEnery, K. W. (1995). An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine, 20(12), 1351-1358. https://doi.org/10.1097/00007632-199506020-00005 [ Links ]
Goh, S., Price, R. I., Leedman, P. J., & Singer, K. P. (2000). A comparison of three methods for measuring thoracic kyphosis: implications for clinical studies. Rheumatology, 39(3), 310-315. https://doi.org/10.1093/rheumatology/39.3.310 [ Links ]
Gonçalves, G. B., & Pereira, J. S. (2008). Radiological assessment of the angular values of back-lumbar and sacral-lumbar curvature in adolescents. Acta Fisiatrica, 15(2), 92-95. [ Links ]
Hammerberg, E. M., & Wood, K. B. (2003). Sagittal profile of the elderly. Journal of Spinal Disorders & Techniques, 16(1), 44-50. https://doi.org/10.1097/00024720-200302000-00008 [ Links ]
Hardacker, J. W., Shuford, R. F., Capicotto, P. N., & Pryor, P. W. (1997). Radiographic standing cervical segmental alignment in adult volunteers without neck symptoms. Spine, 22(13), 1472-1480. https://doi.org/10.1097/00007632-199707010-00010 [ Links ]
Harrison, D. D., Janik, T. J., Troyanovich, S. J., & Holland, B. (1996). Comparisons of lordotic cervical spine curvatures to a theoretical ideal model of the static sagittal cervical spine. Spine, 21(6), 667-675. https://doi.org/10.1097/00007632-199707010-0001010.1097/00007632-199603150-00002 [ Links ]
Harrison, D. D., Harrison, D. E., Janik, T. J., Cailliet, R., Haas, J. W., & Ferrantelli, J. L. (2004). Modeling of the sagittal cervical spine as a method to discriminate hypo-lordosis: results of elliptical and circular modeling in 72 asymptomatic subjects, 52 acute neck pain subjects, and 70 chronic neck pain subjects. Spine, 29(22), 2485-2492. https://doi.org/10.1097/01.brs.0000144449.90741.7c [ Links ]
Harrison, D. E., Harrison, D. D., Troyanovich, S. J., & Harmon, S. (2000). A normal spinal position: It’s time to accept the evidence. Journal of Manipulative and Physiological Therapeutics, 23(9), 623-644. https://doi.org/10.1067/mmt.2000.110941
Higgins, J. P. T., & Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21(11), 1539-1558 .https://doi.org/10.1002/sim.1186 [ Links ]
Higgins, J. P. T., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ, 327(7414), 557-560. https://doi.org/10.1136/bmj.327.7414.557 [ Links ]
Hrysomallis, C. (2010). Effectiveness of strengthening and stretching exercises for the postural correction of abducted scapulae: a review. Journal of Strength and Conditioning Research, 24(2), 567- 574. https://doi.org/10.1519/JSC.0b013e3181c069d8 [ Links ]
Jackson, R. P., Peterson, M. D., McManus, A. C., & Hales, C. (1998). Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordosis to the pelvic radius on standing lateral radiographs of adult volunteers and patients. Spine, 23(16), 1750-1767. https://doi.org/10.1097/00007632-199808150-00008 [ Links ]
Janssen, M. M., Drevelle, X., Humbert, L., Skalli, W., & Castelein, R. M. (2009). Differences in male and female spino-pelvic alignment in asymptomatic young adults: a three-dimensional analysis using upright low-dose digital biplanar X-rays. Spine, 34(23), E826-E832. https://doi.org/10.1097/BRS.0b013e3181a9fd85 [ Links ]
Kasai, T., Ikata, T., Katoh, S., Miyake, R., & Tsubo, M. (1996). Growth of the cervical spine with special reference to its lordosis and mobility. Spine, 21(18), 2067-2073. https://doi.org/10.1097/00007632-199609150-00003 [ Links ]
Korovessis, P. G., Stamatakis, M. V., & Baikousis, A.G. (1998). Reciprocal angulation of vertebral bodies in the sagittal plane in an asymptomatic Greek population. Spine, 23(6), 700-705. https://doi.org/10.1097/00007632-199803150-00011 [ Links ]
Korovessis, P., Stamatakis, M., & Baikousis, A. (1999). Segmental roentgenographic analysis of vertebral inclination on sagittal plane in asymptomatic versus chronic low back pain patients. Journal of Spinal Disorders, 12(2), 131-137. https://doi.org/10.1097/00002517-199904000-00009 [ Links ]
Le Huec, J. C., Demezon, H., & Aunoble, S. (2015). Sagittal parameters of global cervical balance using EOS imaging: normative values from a prospective cohort of asymptomatic volunteers. European Spine Journal, 24(1), 63-71. https://doi.org/10.1007/s00586-014-3632-0 [ Links ]
Lee, C. S., Chung, S. S., Kang, K. C., Park, S. J., & Shin,S. K. (2011). Normal patterns of sagittal alignment of the spine in young adults radiological analysis in a Korean population. Spine, 36(25), E1648-E1654. https://doi.org/10.1097/brs.0b013e318216b0fd [ Links ]
Lee, C. S., Noh, H., Lee, D.H., Hwang, C. J., Kim, H.,& Cho, S. K. (2012). Analysis of sagittal spinal alignment in 181 asymptomatic children. Journal of Spinal Disorders & Techniques, 25(8), E259-E263. https://doi.org/10.1097/bsd.0b013e318261f346 [ Links ]
Lin, R. M., Jou, I. M., & Yu, C. Y. (1992). Lumbar lordosis: normal adults. Journal of the Formosan Medical Association, 91(3), 329-333. [ Links ]
Loney, P. L., Chambers, L. W., Bennett, K. J., Roberts, J. G., & Stratford, P. W. (1998). Critical appraisal of the health research literature: prevalence or incidence of a health problem. Chronic Diseases in Canada, 19(4), 170-176. [ Links ]
Marty, C., Boisaubert, B., Descamps, H., Montigny, J., Hecquet, J., Legaye, J., & Duval-Beaupère, G. (2002). The sagittal anatomy of the sacrum among young adults, infants, and spondylolisthesis patients. European Spine Journal, 11(2), 119-25. [ Links ]
Miyazaki, M., Hymanson, H., Morishita, Y., He, W., Zhang, H., Wu, G., & Wang, J. C. (2008). Kinematic analysis of the relationship between sagittal alignment and disc degeneration in the cervical spine. Spine, 33(23), E870-E876. https://doi.org/10.1097/brs.0b013e3181839733 [ Links ]
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Annals of Internal Medicine, 151(4), 264-269. https://doi.org/10.7326/0003-4819-151-4-200908180-00135 [ Links ]
Monticone, M., Ambrosini, E., Cazzaniga, D., Rocca, B., Ferrante, S. (2014). Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial. European Spine Journal, 23, 1204-1214. https://doi.org/10.1007/s00586-014- 3241-y [ Links ]
Nagasawa, A., Sakakibara, T., & Takahashi, A. (1993). Roentgenographic findings of the cervical spine in tension-type headache. Headache, 33(2), 90-95. https://doi.org/10.1111/j.1526-4610.1993.hed3302090.x [ Links ]
Oliveira, T. S., Candotti, C. T., La Torre, M., Pelinson, P. P. T., Furlanetto, T. S., Kutchak, F. M., & Loss, J. F. (2012). Validity and reproducibility of themeasurements obtained using the flexicurve instrument to evaluate the angles of thoracic and lumbar curvatures of the spine in the sagittal plane. Rehabilitation Research and Practice, 1-9. https://doi.org/10.1155/2012/186156 [ Links ]
Oshiro, V. A., Ferreira, P. G., & da Costa, R. F. (2007). Alterações posturais em escolares: uma revisão da literatura. Revista Brasileira de Ciências da Saúde, 3(13), 15-22. [ Links ]
Perriman, D. M., Scarvell, J. M., Hughes, A. R., Ashman, B., Lueck, C. J., & Smith, P. N. (2010). Validation of the flexible electrogoniometer for measuring thoracic kyphosis. Spine, 35(14), E633-E640. https://doi.org/10.1097/brs.0b013e3181d13039 [ Links ]
Propst-proctor, S. L., & Bleck, E. E. (1983). Radiographic determination of lordosis and kyphosis in normal and scoliotic children. Journal of Pediatric Orthopaedics, 3(3), 344-346. https://doi.org/10.1097/01241398-198307000-00013 [ Links ]
Singer, K. P., Jones, T. J., & Breidahl, P. D. (1990). A comparison of radiographic and computer- assisted measurements of thoracic and thoracolumbar sagittal curvature. Skeletal Radiology, 19(1), 21-26. https://doi.org/10.1007/bf00197923 [ Links ]
Singh, D. K., Bailey, M., & Lee, R. (2010). Biplanar measurement of thoracolumbar curvature in older adults using an electromagnetic tracking device. Archives of Physical Medicine and Rehabilitation, 91(1), 137-142. https://doi.org/10.1016/j.apmr.2009.08.145 [ Links ]
Troyanovich, S. J., Cailliet, R., Jantk, T. J, Harrison, D. D., & Harrison, D. E. (1997). Radiographic mensuration characteristics of the sagittal lumbar spine from a normal population with a method to synthesize prior studies of lordosis. Journal of Spinal Disorders, 10(5), 380-386. https://doi.org/10.1097/00002517-199710000-00004 [ Links ]
Vedantam, R., Lenke, L. G., Keeney, J. A., & Bridwell, K. H. (1998). Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine, 23(2), 211-215. https://doi.org/10.1097/00007632-199801150-00012 [ Links ]
Vialle, R., Levassor, N., Rillardon, L., Templier, A., Skalli, W., Guigui, P. (2005). Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. The Journal of Bone and Joint Surgery-American, 87(2), 260-267. https://doi.org/10.2106/00004623-200502000-00004 [ Links ]
Wright, J. G., & Bell, D. (1991). Lumbosacral joint angles in children. Journal of Pediatric Orthopedics, 11(6), 748-751. https://doi.org/10.1097/01241398-199111000-00009 [ Links ]
Voutsinas, S. A., & MacEwen, G. D. (1986). Sagittal profiles of the spine. Clinical Orthopaedics and Related Research, 210, 235-242. https://doi.org/10.1097/00003086-198609000-00034 [ Links ]
Yukawa, Y., Kato, F., Suda, K., Yamagata, M., & Ueta,T. (2012). Age-related changes in osseous anatomy, alignment, and range of motion of the cervical spine. Part I: Radiographic data from over 1,200 asymptomatic subjects. European Spine Journal, 21(8), 1492-1498. https://doi.org/10.1007/s00586-012-2167-5 [ Links ]
Zaina, F., Donzelli, S., Lusini, M., & Negrini, S. (2012). How to measure kyphosis in everyday clinical practice: a reliability study on different methods. Studies in Health Technology and Informatics, 176, 264-267. [ Links ]
Zhu, Z., Xu, L., Zhu, F., Jiang, L., Wang, Z., Liu, Z., Qiu, Y. (2013). Sagittal alignment of spine and pelvis in asymptomatic adults: norms in Chinese populations. Spine, 39(1), E1-E6. https://doi.org/10.1097/brs.0000000000000022 [ Links ]
Zubović, A., Davies, N., Berryman, F., Pynsent, P., Quraishi, N., Lavy, C., Fairbank, J. (2008). New method of scoliosis deformity assessment: ISIS2 system. Studies in Health Technology and Informatics, 140, 157-160.
Acknowledgments: The author thanks CAPES for financially supporting this research.
Conflict of interests: Nothing to declare.
Funding: The present study was funded by CAPES (Brazilian government research funding agency), PhD research grant.
Manuscript received at February 19th 2017; Accepted at May 20th 2018
[*] Corresponding author: Rua Albino Paul, 45 Bairro Jardim América, São Leopoldo-RS, Brasil Email: tassiasf@gmail.com

