










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPsicologia, Saúde & Doenças
versão impressa ISSN 1645-0086
Psic., Saúde & Doenças vol.16 no.1 Lisboa mar. 2015
https://doi.org/10.15309/15psd160211
Incentive schemes for prevention of overweight and systems information: Tempest case study
Sistemas de incentivo para prevenção de sobre peso e sistemas de informação: Tempest estudo de caso
T.Gaspar1,2,3, M.G.Matos2,3,4, T.Santos2,3,4,5 F.Albergaria1, G.Tomé2,3, M. Ferreira2, & Equipa Aventura Social
1 - Universidade Lusíada de Lisboa
2 – Aventura Social, Faculdade de Motricidade Humana/U. Lisboa
3-ISAMB/U. Lisboa
4 - WJCR /ISPA, Lisboa
5-Doutoranda Ciências da Saúde, Educação para a Saúde
Endereço para Correspondência
ABSTRACT
The European project TEMPEST (Temptations to Eat Moderated by Personal and Environmental Self-regulatory Tools) (www.tempestproject.eu), took place from 2009 to 2013 in nine countries, including Portugal. The main objectives of the project focused on the identification and analysis of new incentive schemes for prevention of obesity in children and adolescents, to obtain greater insight into the role of self-regulatory competence in the management of non-healthy food choices ("temptations") and to contribute to the development of intervention programs focused on effective prevention, in different social settings.This article focuses on outcomes of the first objective, presenting an analysis of incentive schemes for the prevention of obesity in Portuguese children and adolescents, through the identification and characterization of the existent programs/policies in the country. After the research, several programs were identified, mostly multidimensional that aimed, above all, to increase the awareness about the prevalence of this clinical condition, seeming to indicate that Portugal demonstrates good practices and programs related to eating behavior, through the Ministries of Education and Health, of interventions and policies applied in schools and health care.
Keywords -children and adolescents; obesity prevention; Portuguese programs and policies; Portuguese systems information; TEMPEST Project
RESUMO
O projecto europeu TEMPEST (Tentações Alimentares Moderadas por Estratégias de Auto-regulação Pessoais e Ambientais) (www.tempestproject.eu) decorreu entre 2009 e 2013 em 9 Países, incluindo Portugal. O objectivo central do projecto centra-se na identificação e análise de novos esquemas de incentivo na prevenção da obesidade em crianças e adolescentes, de forma a obter maior conhecimento sobre o papel das competências de auto-regulação na gestão de escolhas alimentares não saudáveis (“tentações”), e, na contribuição para o desenvolvimento de programas de intervenção focados em prevenções eficazes, em diferentes settings sociais.
O presente artigo focou-se nos resultados verificados ao nível do objectivo 1, apresentando uma análise dos esquemas de incentivo para a prevenção da obesidade em crianças e adolescentes portugueses, através da identificação e caracterização do conjunto de programas/políticas existentes no país. Após a pesquisa realizada, foram identificados vários programas, na sua maioria multidimensionais e que visam, sobretudo, aumentar o conhecimento sobre a prevalência desta condição clínica. Foram também apresentados dados estatísticos e informações relativas ao sistema Português, recolhida através dos Ministérios da Educação e da Saúde sobre intervenções e políticas aplicadas em escolas e serviços de saúde.
Palavra-chave- crianças e adolescentes; prevenção da obesidade; programas e políticas Portuguesas; Projecto TEMPEST; Sistema de informação Português.
Obesity is still growing at an alarming rate all over the world. It is estimated that around 250 million people are obese (WHO, 1998) and that in 2025, 50% of the population will be obese (Chopra & Darnton-Hill, 2002). Since the 80’s, in Europe, the numbers have tripled and in the last 10 years the increase, in some countries, has been of 10-14% with associated comorbidities (OMS, 2006) and increased severity (Flegal, Caroll, Ogden, & Johnson, 2002). The projections indicated that in 2010 there would be around 10 million overweight and obese children and adolescents (Branca, 2007), with the young people from East Europe the least affected, followed by Central, West and North Europe and, with the highest obesity rates the children and adolescents from Southern Europe (Janssen et al., 2005; Lobstein & Frelut, 2003). These numbers are alarming mainly because, in most cases, obesity persists throughout adulthood (Magarey, Daniels, Boulton, & Cockington, 2003) and is associated to severe clinical situations, low levels of schooling and poverty (Dietz, 1998).
Portugal is no exception to this reality and, in 2008, data indicate that 53.6% of the Portuguese adult population is overweight or obese (do Carmo et al., 2008), with an increase in child obesity. In children with 7 to 9 years of age, 20.3% are overweight and 11.3% are obese. With the total number of 31.6% children overweight or obese this number indicates a high prevalence when compared with other European countries that used the same methods to define weight and obesity (Padez, Fernandes, Mourão, Moreira, & Rosado, 2004). The fact that Portugal also presents lower levels of physical activity (when compared to the rest of Europe), and associated to an unbalanced diet, leads to a progressive increase of obesity (Martinez-Gonzalez et al., 2001). The Portuguese reality eventually lead the Health Department, through an Information Bulletin nº09/DGCG dated 25/03/04 (Direcção-Geral de Saúde, 2004), to consider obesity a chronic illness, with a multifactorial basis that requires continued efforts to be controlled, a threat for health and an important risk factor for the development and aggravation of other illnesses; it affects men and women of all ages and ethnicities and requires long term strategies for its prevention and effective control.
Despite the recognized role of genetic factors in the dramatic increase of the number of children and adolescents with obesity, research has shown that a big part of the responsibility is also associated to behavioral factors, such as inappropriate diets (excessive consumption of high calorie beverages and foods) and low levels of physical activity, related to social changes (Branca, 2007; Raynor & Epstein, 2001). In fact, the current social scenery presents little opportunities for children and adolescents to practice sports and physical activity outdoors (mainly in urban areas), with the most frequent activities to be watch television, play with video games and computers, among other sedentary activities. To this, the substitution of healthy diets with large portions of fast-food, snacks and sodas, is also associated.
The most convincing explanation for the strong increase of obesity among European children and adolescents in the last decade, placing the issue as one of the most important in Europe (European Commission, 2007; WHO, 2007), results in the unbalance between the ingested energy and the used energy, based in the expression ‘toxic’ eating (Wadden, Brownell, & Foster, 2002) or obese environment (Swinburn, Egger, & Raza, 1999). The environment in which most European children and adolescents are living is characterized by a great variety of unhealthy options/choices, very tasty and with high levels of calories, very accessible and with a deep impact in their eating habits and physical activity practices. The concept of eating temptations may be an explanation to justify the influence that the environment has in children and adolescents’ choices.
Part of the adaptive past, the innate sensation of pleasure of eating that humanity learnt to internalize as a form of protection against hunger is now harmful to our health, in a society where super caloric and good looking food is ad libitum, and the mere presence of food may be experienced as a temptation (Peters, Wyatt, Donahoo, & Hill, 2002; Pinel, Assanand, & Lehman, 2000).
It is important not to forget that children and adolescents seem to be more vulnerable to this environment because: 1) the knowledge about long term risks for their health are not totally consolidated; 2) the identification processes and autonomy may reinforce them to go with their own choices, and not in favor of adult recommendations (Darling, Reeder, McGee, & Williams, 2006; Gibbons, Gerrard, & Lane, 2003).
The greatest challenge in the prevention of obesity will be the encouragement of new ways to deal with food temptations and physical inactivity (Gaspar, Matos, Santos, & Albergaria, 2012).
THE TEMPEST PROJECT
The TEMPEST project (www.tempestproject.eu) runs between 2009 and 2013, in a total period of 48 months, in 9 countries. In Portugal (partner 7) the work has been developed through the Social Adventure Project (Faculty of Motricidade Humana/Universidade Técnica in Lisboa and Centre of Malaria and Tropical Diseases/Hygiene and Tropical Medicine Institute, Universidade Nova de Lisboa).
The project has the following main objectives: 1) analyze the already existing and new strategies for obesity prevention in children and adolescents; 2) gain more knowledge on the role of self-regulation skills in the management of non-healthy food choices (temptations) and research in what way its promotion can allow children and adolescents to deal with these less healthy and tempting choices, present in their environment; 3) contribute for the development of efficient intervention programs for the prevention of this chronic disease, in different social settings.
The TEMPEST also has four specific goals: (1) Develop and validate a Self-Regulation Skills Questionnaire related to child and adolescent health, culturally valid in European countries; (2) Determine the impact of strategies with or without financial incentives, based on the analysis of the already existing strategies; (3) Examine the influence of new and experimental incentive strategies; (4) Determine the impact of temptations on self-regulation skills and behaviors associated to weight, in social contexts that differ in terms of the value of those self-regulation skills and test experimental interventions, based on their results.
Previous results of the TEMPEST project offer the conceptualization of innovative approaches in the prevention of obesity in European youth that are promoted through the website, pamphlets for the public in general, manuals for professionals, a validated and reliable self-regulation questionnaire, presentation in international conferences and research articles (Gaspar, Matos, Santos & Albergaria, 2012).
The present article will focus on the analysis of incentive strategies, through the characterization of existing programs and policies in Portugal.
METHOD
The research was conducted through online research on official/government websites, scientific publications and interviews to representatives from Health and Education Ministry, and specialists in the promotion and dissemination of these programs/policies. Were also contacted professional organizations, as well as, policy makers, health professionals and school, student and teen organizations.
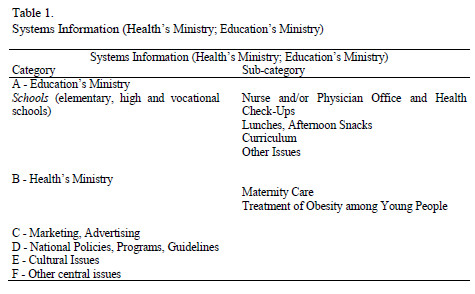
The system information data was organized by categories and subcategories. (see Table 1).
The institutions that were contacted can be organized into: 1) Health promotion and Care taking (ENSP/UNL, Escola Nacional de Saúde Pública; FCM/UL, Faculty of Medical Sciences); 2) Youth Care Taking and Education (D. Estefânia Hospital; Portuguese Youth Institute-IPJ); 3) Political and Government Institutions (Ministry of Education; Ministry of Health; Platform Against Obesity–Ministry of Health; Oeiras city hall); 4) Individual Initiatives (Lusófona University; Tropical Science Research Institute – Global Development Program; Faculty of Sport/UP); 5) Consumer/patient movements (ADEXO – Portuguese Association of Obese and former obese); 6) Industry and Marketing (FIPA - Federation of Portuguese Food Industries).The contacts for data collection include the Ministry of Education (Board of Curricula Development and Innovation) and City Halls of Loures, Odivelas, Oeiras, Silvesand Beja.
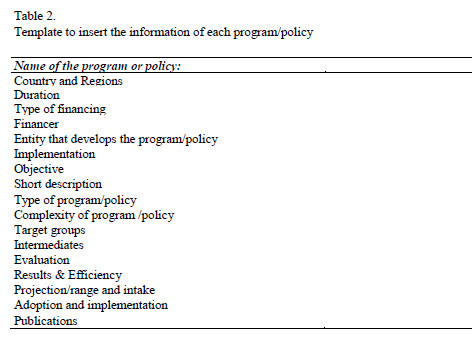
In order to present a deeper analyzes specifically related to programs and policies, a template was elaborated for each entity to fill in with data about the program and/or policy (see Table 2).
RESULTS
Systems Information (Health’s Ministry; Education’s Ministry)
The results related to Systems information’s going to be organized by the categories and subcategories presented in Table 1. Several questions related to system information were based on information collected from several fonts, such us, grey literature, official websites and interviews with specialist or Health and education Ministry representatives.
A - Schools (elementary, high and vocational schools)
A1 - Nurse and/or Physician Office and Health Check-Ups
- Are there official regulations on health promotion, to be followed by school, nurses and physicians? Yes - Student Health Support Office (Ministry of Education and Health Ministry);
- Description of health promotion at school (e.g. who provides it, is it related to health check-ups, is it provided for classes, are leaflets delivered...).
- Aim: to promote health behaviours, and to prevent diseases in children/adolescents and in school community.
In order to create and develop the Student Health Support Office, it is important to train teachers. Those offices are inside schools, where teachers or older students (mentoring/peers education) are available to help, listen and give information about health behaviour, including, eat behaviour. Those offices can also develop other activities, such us, meetings with invited specialist for school community and parents: develop events and activities involving parents and community around school. Example: students are invited to cook their own healthy meal in the canteen; or every week canteen has a special menu from different parts of the country or other countries (migrant students);
GTES (2007) Process Report:
http://www.dgidc.min-edu.pt/saude/Documents/Relatorio_progressoGTES.pdf
GTES (2007) Final Report:
http://www.dgidc.min-edu.pt/saude/Documents/GTES_RELATORIO_FINAL.pdf
A2 - Lunches, Afternoon Snacks
- Is it mandatory to provide a free school lunch? No.
- Description of school food provision system in Portugal. There is social school assistance for low socioeconomic status students, which do not pay school lunch or have discounts, depending on their income level. For instance: level A students have free school lunch; level B students pay 0.73 €/lunch; discount students pay 1.46 €/lunch.
- Is school lunch regulated trough national guidelines? Yes. There is meal (lunch) distribution at school (co-funding by Ministry of Education), respecting nutritional and quality parameters recommended in specific documents (presented below): Document A: Circular 11/DGIDC/2007 “Recommendations for school buffets”:
The school buffet represents a complementary service of school cafeteria, aimed to provide meals to students and all educational community, according to healthy and balanced diet principles. Buffets are particularly important as social work and living space, place of social norms learning and cultural reinforcement. This document appeals to the above entities to (1) the need to meet food supply in accordance with provisions, in order to have both buffet and vending machines, and, it is also important to license suppliers; (2) staff hygiene and hygiene conditions on food exposure (only allowed in buffet and cafeteria); (3) buffet timing suits actual needs of school population, (4) profit margins. The document also suggests that this should be a streamlined space, including the promotion of nutritional education related activities, sending to this purpose, posters and leaflets for parents.
Document B: Circular 14/DGIDC/2007 “School Canteen: General Standards for Food”:
The school cafeteria is crucially important in nutritional and social life of students. So, healthy and balanced diet is a key factor in health and school performance, and there are certain guidelines that need to occur. Thus this document focuses on: (1) list of permitted food, (2) menu preparation, (3) hygiene and food safety, (4) equipment and tools and (5) legislation.
Regional Education; Kindergartens Public Network; Basic Schools 1st Cycle; Schools C+S; EB 2.3; EBI's; Schools with 3rd Cycle; Private Education Settlements with Parallelism
- Is there a lot of variation between schools, concerning lunch contents? No, there are no variations on quantity or quality of the content of the lunch, but each school choose their own daily menu – they all have soup; main plate and desert (mainly fruit).
- Description of a typical lunch (beverage, bread, potato/rice/etc., vegetables, meat/fish, dessert; does it include fries or chips).
The typical lunch is: Vegetable soup; Meat or fish + rice/potatoes or pasta + salad or cooked vegetable; Bread; Fruit; Water.
- Is there a free/cheap fruit and vegetable distribution programme at schools? Yes. There is a school fruit program since 2009: distributing 1 piece of fruit, twice a week (at other times other than lunch or milk time).
- Is it mandatory to provide a free afternoon snack? Yes. The free afternoon snack is supported by both school fruit program and school milk program (the last established since 1973 (elementary school): distributing 1 milk pack, everyday (at other times other than lunch or fruit time).
- Legislation/guidelines on the type of foods available to buy in schools (kiosks, vending machines etc.)? Yes.These guidelines indicate which type of food to promote, to minimize or not to allow (not drinking machines).
Proportion of schools having snack machines?All.
Proportion of schools having soft drink machines? None.
A3 - Curriculum
- Home Economics? Not included in curriculum
Are healthy eating aspects included?
- Health Education? Yes.
Minimum/maximum hours /week at different class levels*
There is no specific curricular unit, but it is included in schools areas, such as “civics training”, “project area” and “accompanied study”.
- Physical Education? Yes.
Minimum/maximum hours /week at different class levels*
3 to 4h1/2 h
- Other subjects targeting health issues? Yes.
There is no specific curricular unit, but it is included in schools areas, such as “civics training”, “project area” and “accompanied study”.
* The weekly hours depend on the class.
- Are there national regulations/guidelines on afternoon activities, clubs (physical activity)? Yes.
Physical Activities and Sports in School: important to promote inclusion and contribute to fight against academic failure and school dropout and also relevant for the acquisition of health and education habits of young people in school age; provides access for all students to physical activity and sport, as an essential contribution to the education and national sports development. Include 120 different sportive modalities (http://www.desportoescolar.min-edu.pt/).
B - Health Care
B1 - Maternity Care
- Is maternity care free of charge? Yes, in public hospitals/maternities.
- Is public maternity care governed by guidelines? All people have a referral hospital in accordance with residence/home area. So, pregnant women are followed in those hospitals/maternities and frequently have their children there (they also can choose a private hospital, but there they have to pay it or to have an insurance). Usually, if childbirth is well, mother and baby stay there for 48 hours; if the delivery was caesarean, mother and baby stay there for 72 hours. If problems occur they stay there as long as they need. Mother and baby may receive visitors (3 hours/day just two person at the same time; fathers have 2 extra hours alone). Mothers and baby are visited every day by doctors and several mothers and respective babies share the same bedroom. Nurses are available if they call them and their objective is instructing the mother to take care of the baby (bath, etc.) and promote breastfeeding.First baby obligatory vaccines are done in the hospital/maternity.
- Is there health counselling at maternity care (related to eating and physical exercise of mother, child or family)? Not obligatory, but if mother asks for it, there are nurses available and in some maternities they have support related to breastfeeding.
B2 - Treatment of Obesity among Young People
- Are there clinics, in public health care, specialized in obesity treatment among young people? Yes. There are not specific clinics, but hospitals do surgical obesity treatments just for severe cases (these patients are subjected to gastric band). Recently, if the treatment is not available in the public system, it can be done in private hospitals/clinics, supported by public health care system.
- Are there private clinics specialized in obesity treatment among young people? Yes. There are no formal data concerning the number of clinics and patients.
C - Marketing, Advertising
- Are the International Chamber of Commerce (ICC) guidelines on adopted advertising? There is an International Chamber of Commerce and the Portuguese Delegation exists since 1934.
- Are there domestic restrictions/laws on youth marketing (TV, magazines, radio etc.)? Not yet, but in 2009 it was made an agreement between Portuguese Agro Food Federation (FIPA) and Portuguese Announcements Association (APAN), involving 5 commitments:
- FIPA: incentive to diverse more healthy food/nutrients (less salt; less sugar and saturated fat, etc.);
- More and clear information, about nutritional and other components described in the products;
- Conduct code in publicity and marketing related to children;
- Promote physical activity and healthy life styles, in collaboration with municipals, public authorities, and other partners and campaigns;
- Partnerships: collaborate with time and resources to support initiatives, programs and other non-governmental activities and governmental institutions, related to health promotion and healthy eat behaviour and politics.
- Are there any regulations/policies concerning what can be sold in gathering places for young people? Yes. Tobacco and alcoholic drinks cannot be sold to young people with less than 16 years old. It is forbidden to sell alcoholic drinks in cafes/restaurants etc., and to consume alcoholic drinks near schools (the distance is established by municipals).
- Are there any guidelines/laws on how nutrition contents of food products must be labelled? Yes, there are laws concerning how products must be labelled. The information should be clear, so he consumer can identify correctly the product and not to be induced in error. All nutritional information about the product and other components must be also included, especially information related to food intolerance (such us, almonds, milk, etc.).
Taxation Policies
The tax for alcoholic drinks and soft drinks is 23%. Related with food, health food (goods of first necessity) have 6% tax, other food (healthy and unhealthy) have 23% tax. As a curiosity related to Physical activity, such us, Gyms have 23% tax.
D - National Policies, Programs, Guidelines
- Medical associations or other national guidelines related to treatment or prevention of childhood/adolescence obesity: Platform against Obesity/Health Ministry; ADEXO (Obese and Ex-obese Association); Association for the study of obesity (SPEO).
- Awareness and use of the guidelines among physicians and nurses.
Intervention on eating habits and particularly overweight approach among children and young people is an urgent public health problem. Initiatives should fit and be coordinated with the National Health Plan, and the objectives of the program should integrate determinants of health-related living life styles; also coordinated with the National Program to Combat Obesity, the National School Health and other programs forming the National Health Plan. This plan recommends initiatives falling into three key areas: eating habits, physical activity and body weight.
The scientific evidence tells us that to achieve these goals and objectives, strategies should be developed at different levels:
- School and Family: promoting food education in the family, school and community, providing food and food preparations more appropriated and respecting the Mediterranean food traditions.
- Local environment: developing information strategies and people’s motivation on the importance of healthy eating habits for their well-being. Promoting policies that improve nutrition and promote physical activity in population in a sustainable manner, comprehensible and accessible, encouraging the practice of physical activity, particularly among young people.
- Department of Health: Making health professionals (particularly primary care) better prepared to identify and address health problems associated with feeding. These professionals should make a systematic detection of overweight and obesity individuals.
- Work: develop suitable workplace projects to promote health, healthy eating and physical activity, improving the adequacy of available food options.
- Food Sector: creating collaboration environments with hotels, catering and food industry towards promotion and distribution of food that can be provided as part of a healthy diet.
- Assessment and Monitoring: monitoring the implementation of plans and evaluate the obtained results in the strategy context.
Regarding childhood obesity the recommendations within the National Program to Combat Obesity, concern approach and prevention, particularly by recommending intervention at the level of health education at school. It is also important the establishment of standards and guidelines for school places, to include canteens and buffets, to involve family in appropriate food choices, to promote conditions for increasing physical activity and leisure times, and even to establish rules and controls actions for food directed marketing at children. It is also recognized that it should be implemented a comprehensive intervention involving various "actors” from the public to the private sector.
National Nutrition Recommendations Containing Sections for Young People
Platform against Obesity /Health Ministry
http://www.plataformacontraaobesidade.dgs.pt/PresentationLayer/homepage_infantil.aspx?menuid=165
Education Ministry
http://www.drel.min-edu.pt/accao_social_escolar/livro-educacao-alimentar-em-meio-escolar.pdf
Foods to promote in schools:
- Yoghurt and other fermented without added sugar, half-fat/light, giving preference to low lipids % and sweeteners;
- Chocolate milk with fruit fresh or frozen without added sugar;
- Fruit juice: and/or "100% juice, sugars and/or sweeteners added;
- Beverages that contain at least 50% fruit juice and/or vegetables without sugar and/or sweetening matter;
- Drinking public or bottled water;
- Different types of bread made from not low refined flour, but more darker flour and with less salt (e.g.: bread mix, rye bread, bran ...), simple or added, with a) light and half-fat fresh cheese, cured and fused, b) boiled egg, meat birds and mammals (chicken, turkey, pork, beef, ...) or c) tuna or other canned fish, preferably stored in water or oil, d) ham, preferably chicken or turkey, choosing those with low lipids % and always removing any visible fat, e) cooked roast;
- Fresh seasonal fruit, sliced, or even in milkshakes (e.g.: orange, tangerine, kiwi, apple, pear, peach, strawberries, cherries, melon, melon, watermelon, banana ...);
- Various vegetables in the form of salads, available in individual portions (e.g.: lettuce, tomato, carrot, cucumber, cabbage, or beans, pulses, walnuts, hazelnuts, raisins, lettuce leaves, of white cabbage, grated carrot, slices of tomato, cucumber, sprigs of parsley, celery, mint or other corn products and mushrooms).
What features justify the removal of unhealthy food? These foods do not have any nutritional characteristic that justify their presence in school buffets (or on youth feeding). Additionally, other features (not necessarily existing cumulatively) reinforce the relevance to ban them from school, including:
- The school, as an educational and health promoter, must organize itself in line with the national curriculum, which state, for example, that excessive intake of sugar and/or fat can contribute to overweight, among other misdeeds;
- So, schools should therefore be consistent not only with the terms of the programs, but also with other reference documents, including those held by professionals;
- These foods have high concentration of sugars, particularly added and rapid absorption, high fat (lipids), especially saturated and/or added. They are also reduced in fibre, have excessive sodium content, high colouring sweets and preservatives, and high doses edulcorants.
E - Cultural Issues
Bellow there is a summary of the most important ideas, discussed by students, between 12 and 16 years old.
- Is walking and bicycling considered as normal/“cool”, or stigmatized as poor people needs? Do young people bicycle because they prefer, or because they have to?*
Most Portuguese people prefer to go to a gym instead of outdoor activities, although these activities are not connected to poor people. Sometimes students do not have money to the bus ticket so they can go by bicycle or by their own foot. Young people bicycle because they need to go to places and don't have another way, or sometimes they prefer it to using bus or others. But, children and adolescents also use the bicycle and ride with friends in the neighbourhood for fun.
The use of the bicycle as a transport mean is not usual in Portuguese culture. Few people use bicycle as a way of transport, especially in big cities because there are no routs in safe condition and the distances are long. It could be considered as a sport or something to do in leisure time.
- Is physical exercise considered as normal/“cool” or negatively stigmatized?*
Physical exercise is considered normal and in some groups also “cool”, but it doesn’t mean that people do it a lot. Most young people like to do physical exercise but most times they do not have time for that (outside school). So, they just exercise inside school and the type of activity provided by the school, and, sometimes those activities are not the ones that students like best.
- Which foods and drinks are sold in places where young people gather, such as movie theatres, shopping malls, city and town centres?
Usually, fast food, especially when cultural activities are developed in big shopping centres. Fast food tastes good, it is quick and cheap.
- How are different body shapes culturally valued? Is there a strong preference for the skinny/muscular type or the more rounded shape? Any differences between boys and girls? What do body shapes signal? Affluence vs. poverty? Self-control vs. letting go? Higher vs. lower status?*
There is a strong preference for skinny or muscular type; this is general for boys and girls. People status doesn't matter in body shapes, what matters is people's will to be healthy (in this case, not very fat).
Most young people care about their body shape, girls would like to be skinny and boys would like to be muscular. Usually, girls care more about their body shape than boys. Some young people are fat and they do not have control in what they eat. In other hand some girls (mostly) do not eat in order to be slim.
TV series/some actors from TV and magazines are important models and standards for young people.
- How are the two ethos of current western cultures, present in youth cultures in Portugal: a) the ethos of consumption and self-fulfilment through the satisfaction of desires and b) the ethos of self-surveillance and health risk control.
I believe that young people live in conflict, they want to show the world that they just care with a), when they live concerning about how they look (b).
People are very consumerist, they do not have money, they are stressed and disappointed and do not care about health. People buy products that are cheaper and eat healthy food and have a healthy lifestyle depends on social culture and money. Young people are more interested about healthy food, and some subcultures have good and healthy lifestyles, but there is a socioeconomic difference.
- What is regarded as “healthy food” and “healthy eating”?
Healthy food regards eating vegetables, fruit, fish, meat (especially no fat meat), sugar free products, eggs, bread, etc. It also concerns about quality and quantity of food intake, not eating too much at each meal, eat many times a day (6-7 times a day), not eating unhealthy food (like sweets, refrigerants, chips, fast food).
*It must be remember that there are differences between youth subcultures.
DISCUSSION
Eating behaviour can be influenced by several external factors. At school the friends’ eating behaviour is a strong influence, young people eat some type of unhealthy food, even if doesn’t like it, only because a friend eats it too. At home, they eat what parents give them, usually what they buy and cook. The TV is another influence and youth can reply unhealthy behaviours, if they see a commercial related with unhealthy food or actors showing bad eating habits in series/cartoons. It is very difficult for youth to understand that unhealthy food and the lack of physical activities can cause long term related health problems. In Portugal there are several programs related with eating behaviour prevention at national level.
Most of those Programs are multidimensional, relating eating behaviour, psychical activity, and social support, involving several actors and contexts, children and adolescents, families, schools, community and policy makers. The main challenge was the lack of Programs/Projects/intervention evaluation, just few, presented a real evaluation and published results.
Twenty existing programs/policies, implemented in Portugal between 2002 and 2009, were identified and described. Almost all of them follow guidelines from the Ministries of Education and Health, in partnership with other institutions and governmental and non-governmental organizations (IPJ, Higher education, city halls, Industry and marketing, and associations).
Overall, the programs/policies have as objective increase knowledge on the prevalence of obesity in children/adolescents and on the practice of physical activity and healthy eating habits. Most of them are multidimensional and applied in schools, through regulation of school cafeteria policies, marketing strategies and control of obesity levels, focusing on eating behaviors, physical activity and social support. These strategies aim to promote healthy habits and lifestyles, involving different actors and contexts, such as parents/family, teachers, health professionals, specialists in formulating policies and the community in general.
The programs/policies include most of the Portuguese population, are valid and several are implemented throughout several years in the same format, or with slight modifications, aiming different levels of interventions for different goals. Primary prevention and teacher training seem to be the main focus of all programs/policies. Some were totally available online, but for deeper knowledge we found it necessary to contact the involved specialists and institutions.
However, and overall, all studies focus on the relationship between obesity risk factors, both at a macro and meso level, with no offer of new or specific strategies for the prevention of obesity. The articles that were mentioned are available through the journal itself, universities or the authors themselves.
Regarding the identified and analyzed policies/programs, we can conclude that Portugal presents several good practices and programs for the promotion of healthy eating, healthy life styles and obesity prevention, with local and national impact. However, it is important to mention the most relevant limitations that show a need of increase evaluation of each intervention and its impact, as well as the presentation and publication of results.
In fact, since the actual identification of the increase in weight/obesity and recognition of this clinic condition as a chronic disease (Chopra & Darnton-Hilll, 2002; OMS, 2006; WHO, 1998), the number of conducted studies and interventions in Portugal has increased in order to define a plan to fight, prevent and understand the factors and behaviors associated to the condition. The national scenery is characterized by the presence of many and varied eating temptations, associated to low levels of physical activity that contribute to high levels of overweight and obesity in children and adolescents (do Carmo et al., 2008; Martinez-Gonzalez et al., 2001; Padez et al., 2004). The creation of weight control programs, based on these behaviors, is part of the current referenced solution (Wadden et al., 2002), and according to the National Institute of Health – EUA (USDHHS, 1998) the treatment of obesity or overweight goes through the promotion of regular exercise, calorie restriction and include behavioral modification strategies. Therefore, the implementation of intervention programs that aim risk behavioral change and the promotion of protective factors, meaning health promotion, is essential (Elfhag & Rossner, 2005). However, reality frequently shows the protective and promoting role of healthy behaviors but, at the same time, the difficulty to adhering to them (Sheldon, Williams, & Joiner, 2003).
With this reality, it is essential to plan and implement new incentive strategies and prevention policies/programs, as well as those that include the concept of self-regulation that seems to have a fundamental role in the work with children and adolescents (Carver & Scheier, 1998; De Ridder & De Wit, 2006; Gestsdottir & Lerner, 2008; Mueller, 2008; Zimmerman, 2002).
The research done with overweight and obese adults also suggest several important variables, offering possible ideas to work and develop with young populations, such as:
- Self-motivation, self-efficacy and autonomy (Teixeira, Going, Sardinha, & Lohman, 2005);
- Reinforce the idea that treating overweight and obesity may have other benefits beyond health (Pasanisi, Contaldo, Simone, & Mancini, 2001: Vidal, 2002), and involve other areas such as body image, quality of life, self-esteem and depression (Blaine, Rodam, & Newman, 2007; Maciejewski, Patrick, & Williamson, 2005). These psychosocial changes may not come directly from an intervention but serve as mediators in its effect, for example, as a result and a mediator during an obesity treatment (Palmeira et al., 2009).
Based on these ideas, and taking into account the analysis of the existing policies/programs and their limitations, it is urgent to think in new paths as well as evaluate the conducted interventions and publish their results. The publication and dissemination of results may be very useful, and bring many advantages. Offer and sharing the work done with the different policies and programs, and their teams, may avoid the replication of similar interventions and create synergies through the participation of technicians form essential areas and implementation of new and innovative ideas, contributing for an improvement of what has already been done in terms of the prevention of obesity in Portuguese children and adolescents.
On the other hand, evaluation is extremely important. The interventions do not have a direct but indirect effect of behavior through its influence on intermediate or mediator factors that may act upon internal factors (motivation and skills) or external ones (opportunities, exposure to risk factors) that may stimulate or allow the independent decision making. Therefore it is important to understand if the implemented interventions are having the desired effect or if they need to have adaptations or improvement, to offer a more adapted intervention to each population in particular. Only through evaluation can this be done, between the needs of the population and characteristics of the program and making good use of the existing resources and increase of its success.
It is important to mentions that besides this post-intervention evaluation, the literature (referenced and mentioned through the TEMPEST project) also indicates a fundamental concept that must not be forgotten when planning new programs or be added to existent, which is self-regulation.
REFERENCES
Blaine, B.E., Rodman, J., & Newman, J.M. (2007). Weight loss treatment and psychological well-being: a review and meta-analysis. Journal of Health Psychology, 12, 66-82. doi:10.1177/1359105307071741 [ Links ]
Branca, F. (2007). A charter on obesity. European Journal of Public Health, 17, 117-118. [ Links ]
Carver, C. S., & Scheier, M. F. (1998).On the self-regulation behaviour. New York, NY: Cambridge University Press.
Chopra, M., Galbraith, S., & Darnton-Hill I,. (2002). A global response to a global problem: the epidemic of over nutrition. Bulletin of the World Health Organization, 80, 952-958. [ Links ]
Darling, H., Reeder, A.I., McGee, R., & Williams, S. (2006). Disposable income, and spending on fast food, alcohol, cigarettes, and gambling by New Zealand secondary school students. Journal of Adolescence, 29, 837-843. doi:10.1016/j.adolescence.2006.06.003 [ Links ]
De Ridder, D., & De Wit, J. (2006). Self-regulation in health behavior: Concepts, theories and central issues. In D. de Ridder, & J. de Wit, (Eds), Self-regulation in health behaviour (pp. 3-23). England, UK: John Wiley & Sons, Ltd. doi:10.1002/9780470713150.ch1 [ Links ]
Dietz, W.H. (1998). Childhood weight affects adult morbidity and mortality. Journal of Nutrition, 128, 411S-414S. [ Links ]
Direcção Geral de Saúde (2004). Circular Informativa nº09/ DGCG, de 25/03/04. Obesidade como Doença Crónica. In: http://static.publico.clix.pt/docs/pesoemedida/DGS_Circular_Informativa-Obesidade_como_Doenca_Cronica_2004.pdf
do Carmo, I., Santos, O., Camolas, J., Vieira, J., Carreira, M., Medina, L., ..... Galvão-Teles, A. (2008). Overweight and obesity in Portugal: national prevalence in 2003-2005. Obesity Reviews, 9, 11-19. doi:10.1111/j.1467-789X.2007.00422.x [ Links ]
Elfhag, K., & Rossner, S. (2005). Who succeeds in maintaining weight loss? A conceptual review of factors associated with weight loss maintenance and weight regain. Obesity Reviews, 6, 67-85. doi:10.1111/j.1467-789X.2005.00170.x [ Links ]
European Commission (30 May, 2007). White paper on a strategy for Europe on Nutrition, Overweight and Obesity related health issues. Online access: http://ec.europa.eu/health/ph_determinants/life_style/nutrition/documents/nutrition_wp_en.pdf
Flegal, K. M., Carroll, M. D., Ogden, C. L., & Johnson, C. L. (2002). Prevalence and trends in obesity among US adults, 1999-2000.Journal of the American Medical Association, 288, 1723-1727. doi:10.1001/jama.288.14.1723 [ Links ]
Gaspar, T., Matos, M., Santos, T., & Albergaria, F. (2012). The European Project TEMPEST: Analysis of incentive actions in Portugal. Journal of Child and Adolescent Psychology, 3, 137-155 [ Links ]
Gestsdottir, S., & Lerner, R. M. (2008). Positive development in adolescence: The development and role of intentional self-regulation. Human Development, 51, 202-224. doi:10.1159/000135757 [ Links ]
Gibbons, R.X., Gerrard, M., & Lane, D.J. (2003).A social reaction model of adolescent health risk. In J. Suls & K.A. Wallston (Eds.), Social psychological foundations of health and illness, (pp. 107-136). Malden, MA: Blackwell .doi:10.1002/9780470753552.ch5
Janssen, I., Katzmarzyk, P.T., Boyce, W. F., Vereecken, C., Mulvihill, C., Roberts, C., ....The Health Behaviour in School-Aged Children Obesity Working Group (2005). Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obesity Reviews, 6, 123-132.doi:10.1111/j.1467-789X.2005.00176.x [ Links ]
Lobstein, T., & Frelut, M.L. (2003). Prevalence of overweight among children in Europe. Obesity Reviews, 4, 195-200. doi:10.1046/j.1467-789X.2003.00116.x [ Links ]
Maciejewski, M.L., Patrick, D.L., & Williamson, D.F. (2005). A structured review of randomized controlled trials of weight loss showed little improvement in health-related quality of life. Journal of Clinical Epidemiology, 58, 568-578. doi:10.1016/j.jclinepi.2004.10.015 [ Links ]
Magarey, A.M., Daniels, L.A., Boulton, T.J., & Cockington, R.A. (2003). Predicting obesity in early adulthood from childhood and parental obesity. International Journal of Obesity and Related Metabolic Disorders, 27, 505-513. doi:10.1038/sj.ijo.0802251 [ Links ]
Martinez-Gonzalez, M. A., Varo, J. J., Santos, J. L., De Irala, J., Gibney, M., Kearney, J., & Martinez, J. A. (2001). Prevalence of physical activity during leisure time in the European Union. Medicine and Science in Sports and Exercise, 33, 1142-1146. [ Links ]
Mueller, U. (2008). The development of self-regulation: Psychological and neuropsychological perspectives. [ Links ]
OMS (2006). Obesidade E Excesso De Peso. Organização Mundial de Saúde. [ Links ]
Padez, C., Fernandes, T., Mourão, I., Moreira, P., & Rosado, V. (2004). Prevalence of overweight and obesity in 7-9 year-old portuguese children: trends in body mass index from 1970-2002. American Journal of Human Biology, 16, 670-678. doi:10.1002/ajhb.20080 [ Links ]
Palmeira, A. L., Markland, D.A., Silva, M.N., Branco, T.L., Martins S.C., Minderico, C.S., .... Teixeira, P.J. (2009). Reciprocal effects among changes in weight, body image, and other psychological factors during behavioral obesity treatment: a mediation analysis. International Journal of Behavioral Nutrition and Physical Activity, 6, 9. doi:10.1186/1479-5868-6-9 [ Links ]
Pasanisi, F., Contaldo, F., de Simone, G., & Mancini, M. (2001). Benefits of sustained moderate weight loss in obesity. Nutrition, Metabolism, and Cardiovascular Disease, 11, 401-406. [ Links ]
Peters, J.C., Wyatt, H.R., Donahoo, W.T., & Hill, J.O. (2002). From instinct to intellect: the challenge of maintaining healthy weight in the modern world. Obesity Reviews, 3, 69-74. doi:10.1046/j.1467-789X.2002.00059.x [ Links ]
Pinel, J.P.J., Assanand, S., & Lehman, D.R. (2000). Hunger, eating, and ill health. American Psychologist, 55, 1105-1116. doi:10.1037//0003-066X.55.10.1105 [ Links ]
Raynor, H.A., & Epstein, L.H. (2001). Dietary variety, energy regulation, and obesity. Psychological Bulletin, 127, 325-341. doi:10.1037//0033-2909.127.3.325 [ Links ]
Sheldon, G., Williams, G., & Joiner, T. (2003).Self-determination theory in the clinic – Promoting physical and mental health. New Haven, CT: Yale University Press.
Swinburn, B., Egger, G., & Raza, F. (1999). Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Preventive Medicine, 29, 563-570. doi:10.1006/pmed.1999.0585 [ Links ]
Teixeira, P.J., Going, S.B., Sardinha, L.B., & Lohman, T.G. (2005). A review of psychosocial pre-treatment predictors of weight control. Obesity Reviews, 6, 43-65. doi:10.1111/j.1467-789X.2005.00166.x [ Links ]
USDHHS (1998). Clinical Guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. Bethesda, MD: NIH-National Heart, Lung, and Blood Institute.
Vidal, J. (2002). Updated review on the benefits of weight loss. International Journal of Obesity Related Metabolic Disorders, 26, S25-28. doi:10.1038/sj.ijo.0802215 [ Links ]
Wadden, T.A., Brownell, K., & Foster, G. (2002), Obesity: responding to the global epidemic. Journal of Consulting Clinical Psychology, 70, 510-25. doi:10.1037//0022-006X.70.3.510 [ Links ]
World Health Organization-WHO (2007). The challenge of obesity in the WHO European Region and the strategies for response. Copenhagen, DK: WHO Regional Office for Europe
World Health Organization-WHO (1998), Obesity. Preventing and Managing the Global Epidemic. Geneve, CH: World Health Organization.
Zimmerman, J. (2002). Achieving academic excellence: A self-regulatory perspective. In M. Ferrari (Ed.). The pursuit of excellence through education (pp. 85-110). New Jersey, NJ: Erlbaum.
Endereço para Correspondência
Universidade Lusíada de Lisboa; e-mail: tania.gaspar.barra@gmail.com
Recebido em 8 de Julho de 2013/ Aceite em 20 de Março de 2014

