










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPsicologia, Saúde & Doenças
versão impressa ISSN 1645-0086
Psic., Saúde & Doenças vol.13 no.2 Lisboa 2012
Metric properties of the portuguese version of the apathy evaluation scale
Propriedades métricas da versão portuguesa da escala de avaliação de apatia
Lara Caeiro 1, Teresa Silva 2, José M. Ferro 3, José Pais-Ribeiro4, M. Luísa Figueira 5
1 Institute of Molecular Medicine, Faculty of Medicine, University of Lisbon, Portugal (laracaeiro@fm.ul.pt)
2 Centro de Reabilitação de Alcoitão, Portugal
3 Neurology Service, Department of Neurosciences, Hospital de Santa Maria, and Faculty of Medicine, University of Lisbon, Portugal
4 Faculty of Psychology and Education, University of Porto
5 Psychiatry Service, Department of Neurosciences, Hospital de Santa Maria, and Faculty of Medicine, University of Lisbon, Portugal
ABSTRACT
The clinical-rated and self-rated versions of the Apathy Evaluation Scale are validated for English language. The Apathy Evaluation Scale is useful to characterize and quantify apathy. We analyzed the metric properties of the Portuguese version of the Apathy Evaluation Scale-Clinical and of a new 10-item short version of the clinical-rated and self-rated versions Apathy Evaluation Scale. We included, 156 healthy participants, 40 healthy elderly participants, 21 patients with dementia, and 21 patients with depression, comprising a sample of 238 individuals. We studied reliability using Cronbach Alpha (a) and Split-half method, and construct validity using principal component analysis with Varimax rotation. The clinical-rated and self-rated Portuguese versions of the AES are valid instruments to measure apathy in Portuguese speaking individuals. Both the clinical-rated and the self-rated versions Apathy Evaluation Scale can be used instead of the long versions of the Apathy Evaluation Scale.
Key words- Apathy, Depression, Motivation, Neuropsychiatry, Psychometric, Mood, Aboulia
RESUMO
As versões clínica e de auto-avaliação da Escala de Avaliação da Apatia estão validadas na versão original inglesa. A Escala de Avaliação da Apatia é utilizada para caracterizar e quantificar a apatia. Nós analisámos as propriedades métricas das versões portuguesas da Escala de Avaliação da Apatia, e também de uma versão reduzida da escalas clínica e de auto-avaliação , mas com apenas 10-items. Incluímos 156 participantes saudáveis, 40 participantes idosos saudáveis, 21 pacientes com demência, e 21 pacientes com depressão, fazendo uma amostra total de 238 indivíduos. Estudámos o nível de fidelidade suportado pelo Alpha (a) de Cronbach e com o método Split-half, e a validade de construto através da análise dos componentes principais com rotação de Varimax. Na sua versão Portuguesa, tanto a Escala de Avaliação da Apatia clínica como a de auto-avaliação são instrumentos válidos para medir a apatia em sujeitos portugueses. As versões clínica e de auto-avaliação reduzidas de 10-items podem ser utilizadas em substituição das versões mais longas da Escala de Avaliação da Apatia.
Palavras Chave- Apatia, Depressão, Motivação, Neuropsiquiatria, Psicométrico, Humor, Aboulia
Apathy is a lack of motivation with simultaneous decrease in behavioural, cognitive and emotional concomitants of goal-direct behaviour (Marin, 1991; Marin, Biedrzycki & Firinciogullari, 1991) which could lead to an indifference and lack of response to ones surroundings (American Psychological Association, 2007, pp. 65). Apathy is a neurobehavioral syndrome and may comprise aboulia (an extreme loss of will, but expressed by an absence/reduction of spontaneous acting, and thinking), avolition (failure to engage in goal direct-behaviour), athymormia (loss of motor and/or affective auto-activation but not of heteroactivation), and/or affective indifference to any stimulus (American Psychiatric Association (APA), 2002; Marin et al., 1991; Marin, 1990; Sadock & Sadock, 2003). Thus, for the evaluation of apathy it is important to ask for motivation but also observe behaviour, cognition and emotional responses (Marin et al. 1991).
Apathy secondary to a medical condition such as in schizophrenia, depression, Alzheimers dementia, vascular dementia or fronto-temporal dementia, Parkinsons disease, and stroke, was defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) (APA, 2002) as a personality disturbance. Apathy interferes with a patients ability to fulfil daily and social activities (Iancu, Tschernihovsky, Bodner, Piconne, & Lowengrub, 2010). If patients start rehabilitation programs the Apathy Evaluation Scale (AES) may be used for monitorization (Resnick, Zimmerman & Adelman, 1998).
The original English version of the AES was developed and validated by Marin et al. (1991). The original AES aimed to characterize and quantify apathy in patients older than 55 years old, with the AES clinical-rate (AES-C), AES self-rated (AES-S) and AES informant rate, in a healthy sample and in samples of patients with depression or dementia. For the principal components, factor analysis Marin et al. (1991) identified three factors. Internal consistency was high for the clinical rate (coefficient a=.90) and for the self-rated version (coefficient a=0.86) (Marin et al. 1991). The two versions were highly correlated (r=.72, p=<.01). Following the Marin et al. (1991) publication, data from 31 healthy controls revealed that participants would be apathetic if scoring a mean of 26 points, (SD= 6.2), in the AES-C and a mean of 28.1 points, (SD=f 6.4), in the AES-S.
The AES was validated in Chinese and German languages (Lee, Wen, Chao, Chen & Yen, 2008; Lueken et al., 2006). Lee et al. (2008) showed that the Chinese version of the AES-C had high internal consistency (Cronbach a=.90). For the Chinese sample of 31 normal individuals, a mean of 27.9 points, (SD = 7.6), in the AES-C would identify apathetic patients. Lueken et al. (2006) reported high internal consistency for the German version of the AES-C and AES-S (Cronbach a=.92). In this German publication, based on data from 37 controls, participants would be apathetic if they scored a mean of 20.2, (SD= 2.7), in the AES-C, and a mean of 23.5, (SD = 5.8), in the AES-S. The use of the AES was extended to neurologic and psychiatric disorders; Sagen, Faerden, Haug, Melle, Finset, & Dammen (2010) studied factor structure of the Norwegian version of the AES-S in 85 stroke patients and of the AES-C in 76 subarachnoid haemorrhage patients, and of both scales in 104 psychotic patients and Lane-Brown and Tate (2009) validated AES-C in 34 patients with severe traumatic brain injury.
More recently, Lueken et al. (2007) validated a short version of the AES, with items 1 to 4, 6 to 9, 17 and 18, in 356 demented nursing home residents. This short version identified apathetic patients if they had a mean of 14.7 points, (SD = 9.8). Sagen et al. (2010) studied factor structure of a second 10-item version of the AES, with items 1, 2, 4 to 7, 9, 16 to 18, in the follow-up of stroke, subarachnoid haemorrhage and psychotic patients. However, these short versions were not adequate for patients in an acute hospital setting. In the Neurology Service of Hospital Santa Maria in Lisbon, we evaluate acute neurologic patients, and because some of the AES items are not appropriate for a context as a hospital ward for acute patients, we develop a new short version of the AES.
The first aim of this study was to analyze the metric properties of the clinical-rated and self-rated Portuguese version of the AES. The second aim of this study was to analyze the metric properties of a clinical-rated and self-rated 10-item version scale of the AES.
METHOD
Participants
We included two groups of participants which were a) caregivers of patients attending the Neurologic Outpatient Clinic (Healthy participants) aged between 18-80 years old, and b) subjects older than 60 years old from a Day Centre for the elderly (Elderly participants).
Inclusion criteria for healthy participants and elderly participants were: 1) independent in daily activities, 2) fluency in Portuguese and understanding the purpose of the study, 3) living anywhere in Portugal. Exclusion criteria for healthy participants and elderly participants were the presence of any psychiatric disorder or of a cognitive impairment, based on the DSM-IV-TR clinical criteria (APA, 2002).
We also included two groups of patients that were: a) patients attending the Dementia Outpatient Clinic (Dementia patients), and b) patients attending the Psychiatric Outpatient Clinic (Depression patients), at the Hospital Santa Maria in Lisbon.
Inclusion criteria for demented or depressive patients were: 1) having an exclusive diagnosis of mild Alzheimers dementia or of mild cognitive impairment for the dementia group, or 2) having an exclusive diagnosis of major depressive disorder or of a dystimic disorder based on the DSM-IV-TR clinical criteria (APA, 2002) for the depressive group, 3) fluency in Portuguese, 4) understanding the purpose of the study, 5) older than 50 years old for the dementia group and older than 18 years old for the depression group, and 6) living anywhere in Portugal.
Both participants and patients were invited to participate in the study and gave their informed consent. The Ethics Committee of the Faculty of Medicine, University of Lisbon, approved the study.
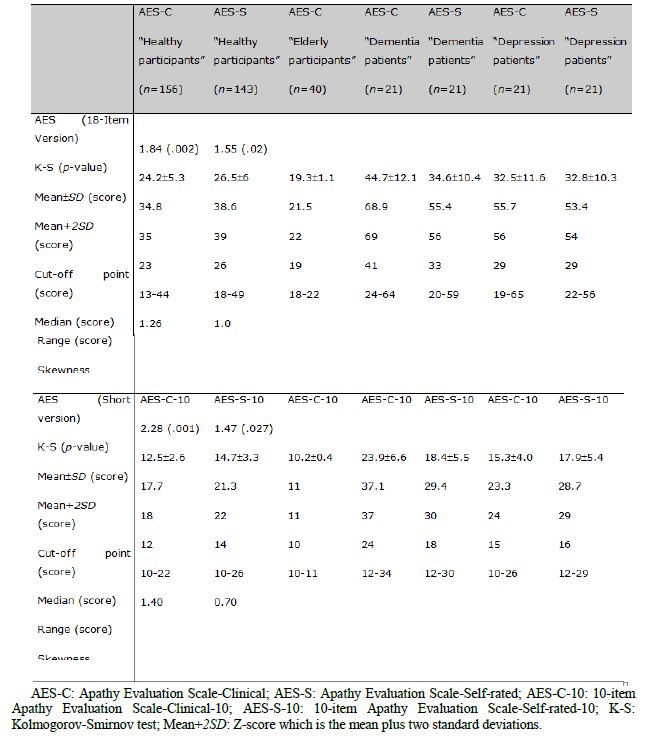
A total sample of 238 individuals voluntarily participated in this study and included 156 healthy participants and 40 elderly participants, 21 patients with dementia and 21 patients with depression. (Table 1)
Demographic characteristics of participants and patients included in each group of patients to evaluate the clinical-rated and self-rated versions of the AES
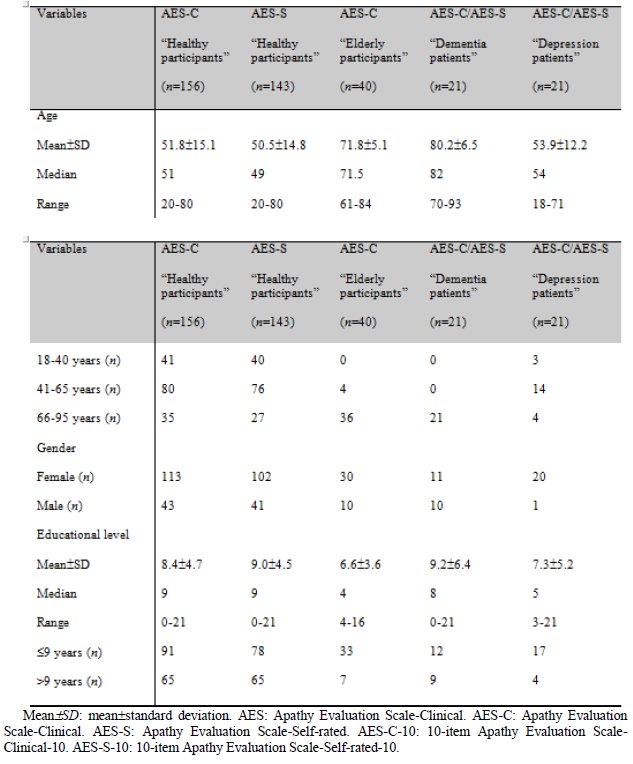
As expected elderly participants and dementia patients were older than healthy participants and depression patients (F(3,237)=47.1, p=.0001; Bonferroni p<.001). Women formed the majority in the group of patients with depression and were less frequent in the group of patients with dementia (?2(3)=9.93, p=.02).
Apathy Evaluation Scale - The AES is an 18-item scale developed by Marin et al. (1991). The clinical rate (AES-C) and self-rated (AES-S) versions of the AES have 18 items each. Responses to each item can be Not at all characteristic (4 points), Slightly characteristic (3 points), Somewhat characteristic (2 points) or Very characteristic (1 point). Items 6, 10 and 11, as negative sentences were scored as Not at all characteristic (1 point), Slightly characteristic (2 points), Somewhat characteristic (3 points) or Very characteristic (4 points). Marin et al. (1991) defined that a higher total score indicated greater severity of apathy, ranging from a minimum of 18 points and a maximum of 72 points.
AES: Adaptation to the Portuguese language - A professional translator translated the English version of the AES-C to Portuguese, and another professional translator translated this Portuguese version into English. The final Portuguese and the corresponding English translations were e-mailed to the original author (Prof. RS Marin) to obtain his approval (Appendix 1). The author approved the translation of the 18-item AES-C version.
Construction and adaptation to the Portuguese language of a short version of the AES
Most of the patients admitted to an acute care hospital have a short stay. During their hospitalization, patients cannot answer if they do things, if they like to start or finish things, because they have to follow the hospital routine and pathways of care. Therefore, we excluded those items from the AES that we considered not to be appropriate for assessing apathy in an acute hospital setting (items 2, 3, 4, 5, 7, 8, 9 and item 16). For the adaptation of the 18-item scale into a 10-item version, we kept the same order of the items: item 1 was kept as item 1, item 6 was changed to item 2, 10 to 3, 11 to 4, 12 to 5, 13 to 6, 14 to 7, 15 to 8, 17 to 9, and item 18 to item 10. The items selected for the clinical-rated version (AES-C-10) were the same as those included in the self-rated version (AES-S-10). As in the Lueken et al. (2007) validation publication, we also excluded items 5 and 16 and as in the Sagen et al. (2010) validation publication we excluded item 3 and 8. Lueken et al. (2007) and Sagen et al. (2010) excluded items 10, 11, 12, 13, 14 and 15, but we retained these items because we thought that for acute patients being interested about and understand their medical condition, getting excited with good things, such as the improvement of their medical condition, and maintaining their interest in friends and in getting their attention during their stay in the hospital, would provide good information about their motivation, or about the possible presence of indifference or even about their engagement in getting healthier. The common items in the 3 versions of a short AES were item 1 (Interested in things), item 6 (Little effort in anything), item 17 (Has initiative) and item 18 (Has motivation).
Procedure
Healthy and elderly participants, dementia and depression patients were interviewed by two psychologists who performed a psychological and cognitive evaluation. For this purpose, we used the clinical information from the Day Centre file of each elderly participant and the Montgomery ?sberg Depression Rating Scale (MADRS) (Montgomery and Asberg, 1979) to assess depression. The Mini-Mental State Examination (MMSE) (Guerreiro, Silva, Botelho, Leitão, Castro-Caldas & Garcia, 1994) was used to assess cognition in healthy participants and elderly participants and in dementia and depression patients. After being assessed for apathy with the AES-C participants and patients filled in the AES-S. If the participants or patients could not read (due to vision problems or being illiterate) the psychologist would read the questions from the AES-S, asking for a No (Not at all characteristic) or Yes response, and if Yes either Slightly characteristic, Somewhat characteristic or Very characteristic.
Statistical Analysis
Bivariate analyses, comparing scores between 2 or all 4 samples, among the healthy, elderly, dementia and depression samples of subjects, were performed using ANOVA (F) with Bonferroni adjustment and independent t-test (t). The correlation between continuous variables was performed using Pearson correlation (r) analysis.
The answers given by the sample of 156 healthy participants were used for additional statistical analysis: 1) Construct validity by factor analysis of principal components with Varimax rotation, the extraction of three factors (we forced number three) and inspection of the screen plot of rotation values. 2) Internal consistency or reliability evaluation using a) Cronbach Alpha (a) and b) Split-half reliability, where results would show good inter-item correlation if a>.65. 3) Standardization: the cut-off point, which was the highest value following the value obtained by the mean plus two standard deviations (Z-score: mean+2SD), as proposed by Streiner and Norman (2003). Apathy was present if subjects scored the value of the cut-off point or above. 4) Categorization of age in three age groups: young (18-40), middle aged (40-65) and older subjects (65-80). 5) Educational levels categorized in the three groups of mandatory school education: low educational level (=4 years of school), mean education (5-9 years of school) and high education (=10 years of school).
Analysis was performed using the SPSS software and a two-tailed p-value of = .05 was considered statistically significant.
RESULTS
Metric properties of the AES-C
We included the sample of 156 healthy participants which constituted a random sequential sample of individuals without any psychiatric or neurological disease or daily living activities and who were caregivers of users of Neurologic Outpatient Clinic.
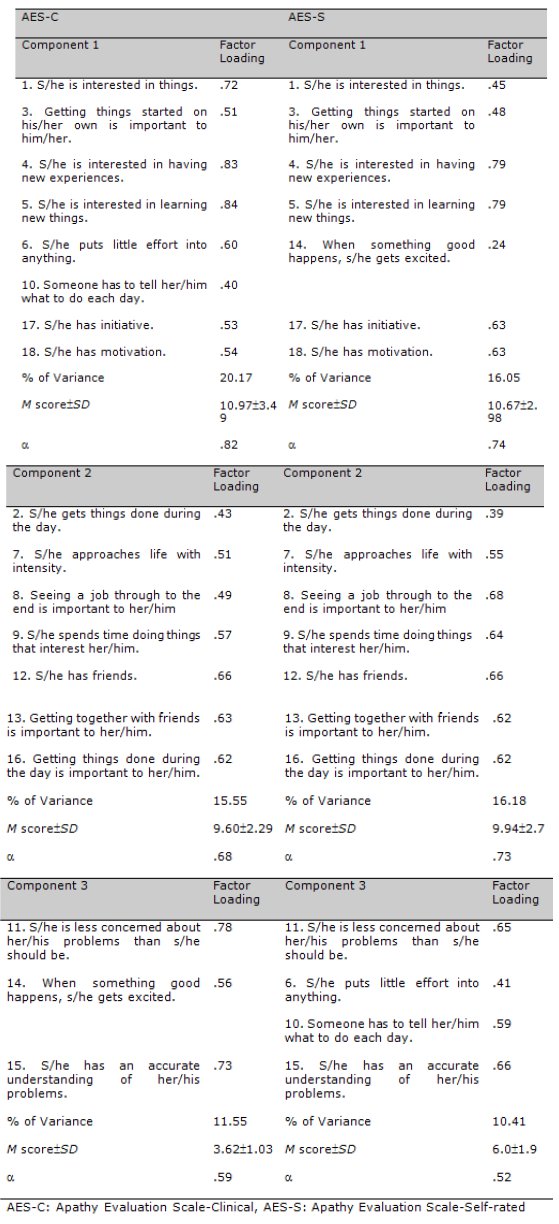
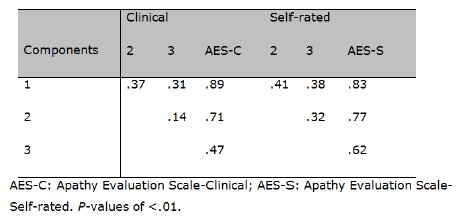
Internal consistency coefficient was high with a Cronbach a=.82 and a Split-half a=.67 (Between the 18 items: F(17,155)=27.55, p< .01). For the principal component analysis (PCA) we did not exclude any items from the scale because they all had high values of > .40. Item component distribution is similar to the original version. The three components (Kaiser Rule) accounted for 47.3% of the variance (Table 2). The three components were inter-correlated (Table 3). AES-C was highly correlated with components 1 and 2 and moderately correlated with component 3 (Table 3).
The three PCA (Kaiser Rule) for the 18-version of the AES-C and AES-S (Rotated Component Matrix)
Pearsons correlation (r) among the three components and between each of these and the AES, in the healthy Participants sample (n=156)
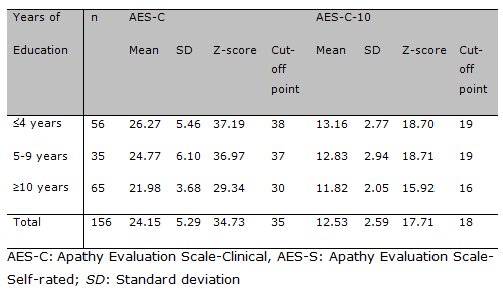
There were no differences in AES-C scale scores between genders (t(154)=0.33, p>.05) and among the three age groups (F(2, 155)=1.94, p>.05). There was a weak negative correlation between AES-C and educational level (r=-.32, p<.01) and we found some differences (F(2,155)=11.54, p<0.01; Bonferroni p<.03) among the three educational groups, with the lowest (4 years and 5-9 years of school) educated groups having higher cut-off points on the AES-C (Table 4). The cut-off point for the AES-C, independently of educational level, was 35 (Table 5) and participants scoring above would be considered as being apathetic (Eleven (5.1%) participants scored above).
Cut-off points of the AES-C and AES-C-10, based on educational levels, in the healthy Participants sample (n=156)
Metric characteristics of the AES and AES-10
Metric properties of the AES-S - From the 156 healthy participants we included 143 for analysis of the AES-S. The remaining 13 healthy participants were not included because they refused to fill in the AES-S. (Table 1)
Internal consistency coefficient was high (Cronbach a=.81; Split-half= .60; Between the 18 items: F(17, 142)= 8.56, p<.01). We computed PCA (Kaiser Rule) with three components and no item was excluded. The three components accounted for 42.6% of the variance (Table 2). The three components were correlated among each other. AES-S was moderately correlated with component 3 and it was highly correlated with components 1 and 2 (Table 3).
No differences were found in AES-S scale scores between genders (t(141)=1.89, p>.05) and among three age groups (F(2,142)=0.41, p>0.05). No correlation was found between AES-S scale scores and educational level (r=-0.81, p>.05) was find.
For the total AES-S scores (Table 5) the cut-off point was 39, thus healthy participants scoring 39 or more would be considered as apathetic (Six (4.2%) healthy participants were apathetic).
Metric properties of the short versions of the AES: AES-C-10 and AES-S-10 (Table 5)
For the AES-C-10 and the AES-S-10, we performed the same analysis but independently from the metric analysis made for AES-C and AES-S, using the healthy participants sample (n=156).
Metric properties of AES-C-10 - Internal consistency coefficient for the AES-C-10 was high (Cronbach a=.70; Split-half=.79). The PCA (Kaiser rule) with three components explained 58.6% of the variance of the 10 items. For AES-C-10, component 1 explained 23.4% of the variance and was represented by five items from the 18-item-scale version, namely: item 1 (interested in things), 6 (put little effort into things), 10 (someone has to tell what to do), 17 (has initiative) and 18 (has motivation). Component 2 explained 18.6% of the variance and was represented by three items: item 11 (less concerned about her/himself), 14 (get excited with good things) and 15 (accurate understanding of problems). Component 3 explained 16.5% of the variance and was represented by two items: item 12 (has friends) and 13 (to be with friends is important). Components 1 and 2 were moderately correlated (r=.39, p<.01), but components 1 and 3 (r=.14, p>.05) and components 2 and 3 (r=.05; p>.05) were not correlated. The AES-C-10 was positively correlated with the three components (F1: r=.83; F2: r=.66; F3: r=.53; p<.01).
There were no statistical differences in AES-C-10 scale scores between genders (t(154)=0.04, p> .05) and among the three age groups (F(2, 155)= 0.33, p>.05). There were differences (F(2, 155)=4.55, p<.01; Bonferroni p<.01) among the three educational groups (Table 4), with the lowest (?4 years and 5-9 years of school) educated groups having higher cut-off points on the AES-C-10. The cut-off point for the AES-C-10, irrespective of educational level, was 18 points. Eleven (7.1%) healthy participants scored =18 and were considered as being apathetic.
Metric properties of AES-S-10 - Internal consistency coefficient for the AES-S-10 was good (Cronbach a=0.65; Split-half=0.57). The PCA (Kaiser rule) with three components explained 51.7% of the variance of the 10 items. For AES-S-10, component 1 explained 19.8% of the variance and was represented by items 1 (interested in things), 17 (has initiative) and 18 (has motivation). Component 2 explained 16.1% of the variance and was represented by items 6 (put little effort into things), 10 (someone has to tell her/him what to do), 11 (less concerned about her/himself), 14 (get excited with good things) and 15 (accurate understanding of problems). Component 3 explained 15.7% of the variance and was represented by items 12 (has friends) and 13 (to be with friends is important). Component 1 was mildly correlated with component 2 (r=.35, p<.01) and with component 3 (r=.19, p<.05). Correlation between components 2 and 3 was not significant (r=.15, p>.05). This AES-S-10 was positively correlated with each of the three components (F1: r=.73; F2: r=.83; F3: r=.49; p<.01).
For AES-S-10 scale scores there were no differences between genders (t(141)=1.89, p>.05), among the three age groups (F(2, 142)=0.61, p>.05) or among the three groups of educational level (F(2, 142)=0.28, p>.05). The cut-off point for the AES-S-10 was 22 points and in our sample of healthy participants 5 (3.5%) reported apathy.
Correlation between scales
The correlations between the scores in the four versions of the AES showed significant moderate to high values (Table 6).
Table 6
Correlations between the two versions of the AES and the two versions of 10-item of the scales, in the healthy participants samples
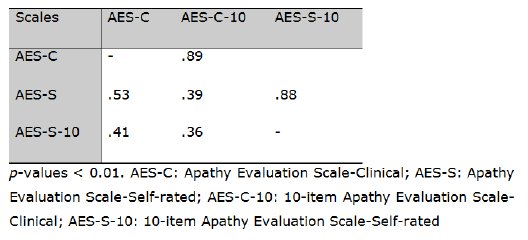
Considering the clinical versions, the AES-C and the AES-C-10, the two were highly correlated meaning that the 10-item short version of the AES-C can easily substitute the AES-C in the clinical rate of apathy.
The same high correlation was seen between the two self-rated versions of the AES, the AES-S and the AES-S-10, meaning that AES-S-10 can replace the AES-S in the self-rating of apathy.
3.6 Comparison between participants and patients samples: AES-C, AES-S, AES-C-10 AND AES-S-10 (Table 1); Graphic 1)
Graphic 1
AES-C profile of participants and patients: Percentages of participants and patients scoring positively (Range 4-2 points: Not at all to Somewhat characteristic) in each item.
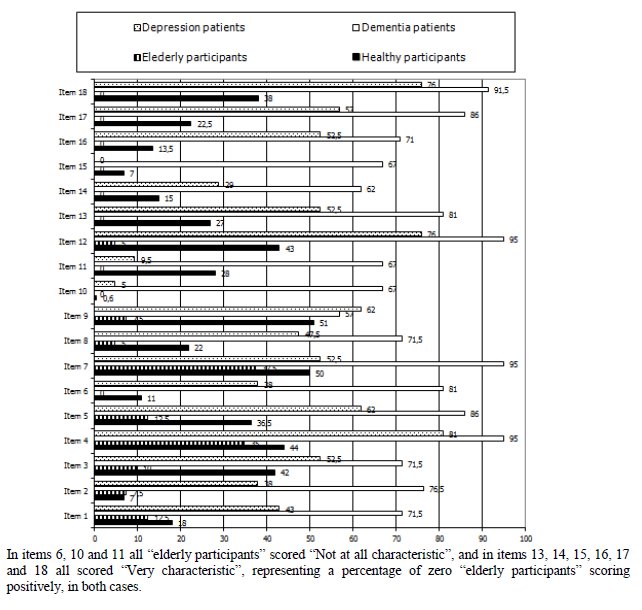
Considering the AES, there were differences in: 1) AES-C: patients with dementia showing the highest mean score, followed by the group of patients with depression (F(3, 237)=82.6, p<=.01; Bonferroni: p<.01). Dementia patients scored positively most frequently in all items, followed by the group of depression patients (Graphic 1); 2) AES-S: healthy participants showed the lower mean scale score (F(2, 184)=16.8, p<.01; Bonferroni: p<.01); 3) AES-C-10: Dementia patients showed higher mean scale scores (F(3, 237)=101.65, p<.01; Bonferroni: p<.01); 4) AES-S-10: Dementia patients showed slightly higher mean scores compared with healthy participants and elderly participants (F(2, 184)=12.97, p<.01; Bonferroni: p<.01).
In items 6, 10 and 11 all elderly participants scored Not at all characteristic, and in items 13, 14, 15, 16, 17 and 18 all scored Very characteristic, representing a percentage of zero elderly participants scoring positively, in both cases.
DISCUSSION
In this study of metric properties, the AES-C and the AES-S showed good construct validity and high internal consistency. The cut-off point of AES-C was 35 points. The cut-off point of the AES-S was 39 points. The items that loaded onto the ACP (Kaiser rule) for the AES-C and AES-S were quite similar, and both scales were moderately correlated. The short clinical-rated (AES-C-10) and self-rated (AES-S-10) short versions of the AES may be used instead of the long versions.
For this study, we included a sample of healthy participants of active community-dwelling Portuguese subjects. In order to have information on independent elderly subjects, we included a sample of elderly participants aged >60 years old. For a comparison with clinical samples, we included depressive patients and demented patients. Comparisons among the four groups showed differences in mean scale scores in the AES-C and in the AES-S: participants presented lower mean scale scores compared with the two clinical samples. The dementia patients had the highest means scale scores. These results confirm previous publication showing that apathy is frequent in patients with depression and in patients with dementia (Biancosino, Picardi, Marmai, Biondi, & Grassi, 2010; Clarke, et al., 2008; 2010; Reyes, 2009;).
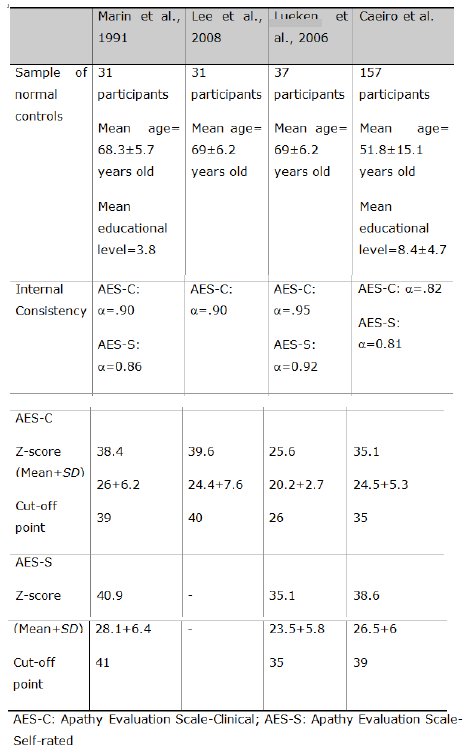
Comparing our results with these three studies (Table 7) all reported good internal consistency with similar Cronbach a values. Both Chinese and English cut-off points were higher compared with the cut-off point in our study, but in the German version cut-off points were lower. The differences between our sample of healthy participants and the Marin et al. (1991) sample of normal controls could be higher motivation in the latter, as they were paid to participate in the study. Another difference was that our sample of healthy participants was more than 10 years younger compared with the other three samples, and had 4.7 mean years of educational level more than Marin et al. (1991) normal controls. Based on educational level, the cut-off points that we found for the AES-C were higher in healthy participants with low education level, and were quite similar to the cut-off point that we calculated for the Marin et al. (1991) sample. In our study, healthy participants with a low educational level expressed themselves and were clinically scored in their daily activities and interests more frequently as not characteristic or as moderate, mildly. On the other hand, healthy participants with higher educational levels expressed themselves and were clinically scored in their daily activities and interests more frequently as being very characteristic. This was not the case on the AES-S, i.e. less educated healthy participants qualified and quantified their motivation, activity, curiosity and emotional attachment just the same as healthy participants with higher educational levels. Clarke et al. (2007) highlighted the possibility of false negatives using the AES-S particularly for patients who have a lack of insight into their problems or apathy, which could be present because of the moderate (and not high) correlation between AES-C and AES-S.
Table 7
Descriptions of healthy participants included in the English, Chinese, German and Portuguese studies of the AES-C and AES-S. Internal consistency and cut-off point of each version.
In the Clarke et al. (2008) publication, older patients with dementia (n=121; age mean=73.7, SD=9.4 years old) were apathetic if they scored above 40.5 points for the AES-C, and 36.5 points for the AES-S, which are lower than the cut-off point in our sample of patients with dementia.
We also studied the metric properties of a new 10-item short version of the AES clinical rate and of a self-rated scale, the AES-C-10 and the AES-S-10, to be used in acute hospital settings. The analysis of AES-C-10 (Cronbach a=.70; Split-half=.76) and the AES-S-10 (Cronbach a=.65; Split-half=.57) showed good construct validity and internal consistency. The cut-off point of AES-C-10 was 18 points and the cut-off point of AES-C-10 was 22 points.
Lueken et al. (2007) also developed a short version of the AES-C, which is different from our short version of the AES-C. We chose and validated 10 items suitable for an acute setting, while Lueken et al. chose 10 items and validated a 10-item scale appropriate for demented nursing home residents and not an acute hospital setting. Sagen et al (2010) also performed a study of the metric properties of a second 10-item version of the AES, in stroke, subarachnoid haemorrhage and in psychiatric patients, 4 months after disease onset. Once again, we think that this proposal was not suitable for acute hospital settings. A common feature is that both were validated in patients and not in healthy participants as we did.
Our study had some limitations. We did not evaluate a sample of patients diagnosed as apathetic by DSM-IV-TR clinical criteria of Personality Disturbances Secondary to a Medical Condition on clinical groups of patients. We also did not compare the performance on AES with a different validated apathy scale. We should note that there is no other validated scale to assess apathy in the Portuguese language. We did not analyze test-retest and inter-rater reliability.
If not detected, silently apathy interferes with individuals mental health decreasing well being and psychosocial involvement (Lamers, Westerhof, Bohlmeijer, ten Klooster, & Keyes, 2011), which is the main reason for giving special attention.
In conclusion, the AES-C and the AES-S were proved to be useful to assess apathy in the normal Portuguese-speaking population. The shorter versions of these two scales (AES-C-10 and AES-S-10) would be of value for use in a hospital setting and in such a setting it can be used instead of the long-versions. Clearly, the four versions of the AES differentiated healthy common people from clinical samples.
REFERENCES
American Psychological Association (2007). A.P.A. Dictionary of Psychology. Washington DC: American Psychological Association. [ Links ]
American Psychiatric Association (APA) (2002). Mood Disorders. In: APA (ed), Diagnostic and Statistical Manual of Mental Disorders, (4th ed. Revised, pp345-428). . Washington DC: American Psychological Association. [ Links ]
Biancosino, B., Picardi, A., Marmai, L., Biondi, M., & Grassi, L. (2010). Factor structure of the Brief Psychiatric Rating Scale in unipolar depression. Journal of Affective Disorders, 124, 329-334. http://dx.doi.org/10.1016/j.jad.2009.11.019 [ Links ]
Clarke, D.E., Ko, J.Y., Lyketsos, C., Rebok, G.W., & Eaton, W.W. (2010). Apathy and cognitive and functional decline in community-dwelling older adults: Results from the Baltimore ECA longitudinal study. International Psychogeriatrics, 22, 819–829. http://dx.doi.org/10.1017/S1041610209991402 [ Links ]
Clarke, D.E., van Reekum, R., Simard, M., Streiner, D.L., Conn, D., Cohen, T., & Freedman, M. (2008). Apathy in dementia: clinical and sociodemographic correlates. Journal of Neuropsychiatry and Clinical Neurosciences, 20, 337-347. http://dx.doi.org/10.1176/appi.neuropsych.20.3.337 [ Links ]
Clarke, D.E., van Reekum, R., Patel, J., Simard, M., Gomez, E., & Streiner, D.L. (2007). An appraisal of the psychometric properties of the Clinician version of the Apathy Evaluation Scale (AES-C). International Journal of Methods in Psychiatric Research, 16, 97–110. http://dx.doi.org/10.1002/mpr.207 [ Links ]
Guerreiro, M., Silva, A.P., Botelho, M.A., Leitão, O., Castro-Caldas, A., & Garcia, C. (1994). Adaptação à população portuguesa e tradução do Mini Mental State Examination (MMSE). Revista Portuguesa Neurologia, Supplement 1, 9. [ Links ]
Iancu, I, Tschernihovsky, E., Bodner, E., Piconne, A.S., & Lowengrub, K. (2010). Escitalopram in the treatment of negative symptoms in patients with chronic schizophrenia: A randomized double-blind placebo-controlled trial. Psychiatry Research, 179, 19-23. http://dx.doi.org/10.1016/j.psychres.2010.04.035 [ Links ]
Lamers, S. M., Westerhof, G. J., Bohlmeijer, E. T., ten Klooster, P. M., & Keyes, C. L. (2011). Evaluating the psychometric properties of the mental health Continuum-Short Form (MHC-SF). Journal of Clinical Psychology, 67, 99–110. http://dx.doi.org/10.1002/jclp.20741 [ Links ]
Lane-Brown, A.T., & Tate, R.L. (2009). Measuring apathy after traumatic brain injury: Psychometric properties of the Apathy Evaluation Scale and the Frontal Systems Behaviour Scale. Brain Injury, 23, 999-1007. http://dx.doi.org/10.3109/02699050903379347 [ Links ]
Lee, S.H., Wen, M.C., Chao, C.C., Chen, Y.J., & Yen, C.F. (2008). Apathy in late-life depression among Taiwanese patients. International Psychogeriatrics, 20, 328-337. http://dx.doi.org/10.1017/S1041610207005698 [ Links ]
Lueken, U., Seidl, U., Schwarz, M., Völker, L., Naumann, D., Mattes, K., .... & Schweiger, E. (2006). Psychometric properties of a German version of the Apathy Evaluation Scale. Fortschritte der Neurologie-Psychiatrie, 74, 714-722. [ Links ]
Lueken, U., Seidl, U., Schwarz, M., Völker, L., Schweiger, E., & Schröder, J. (2007). Development of a short version of the Apathy Evaluation Scale specifically adapted for demented nursing home residents. American Journal of Geriatric Psychiatry, 15, 376-385. http://dx.doi.org/10.1097/JGP.0b013e3180437db3 [ Links ]
Marin, R.S. (1991). Apathy: A neuropsychiatric syndrome. Journal Neuropsychiatry Clinical Neurosciences, 3, 243-254. [ Links ]
Marin, R.S., Biedrzycki, R.C., & Firinciogullari, S. (1991). Reliability and validity of the apathy evaluation scale. Psychiatry Research, 38, 143-162. http://dx.doi.org/10.1016/0165-1781(91)90040-V [ Links ]
Marin RS (1990). Differential diagnosis and classification of apathy. American Journal Psychiatry, 147, 22-30. [ Links ]
Mehta, M., Whyte, E., Lenze, E., Hardy, S., Roumani, Y., Subashan, P., .. & Studenski, S. (2008). Depressive symptoms in late life: associations with apathy, resilience and disability vary between young-old and old-old. International Journal of Geriatric Psychiatry, 23, 238–243.http://dx.doi.org/10.1002/gps.1868 [ Links ]
Montgomery, S.A., & Asberg, M. (1979). A new depression scale designed to be sensitive to change. British Journal of Psychiatry, 134, 382-389. http://dx.doi.org/10.1192/bjp.134.4.382 [ Links ]
Resnick, B., Zimmerman, S.I., & Adelman, A. (1998). Use of the apathy evaluation scale as a measure of motivation in elderly people. Rehabilitation Nursing, 23, 141–147.http://dx.doi.org/10.1002/j.2048-7940.1998.tb01766.x [ Links ]
Reyes, S., Viswanathan, A., Godin, O., Dufouil, C., Benisty, S., Hernandez, K., . & Chabriat, H. (2009). Apathy: a major symptom in CADASIL. Neurology, 72, 905-910. http://dx.doi.org/10.1212/01.wnl.0000344166.03470.f8 [ Links ]
Sadock, B.J.S., & Sadock, V.A.S. (2003). Synopsis of psychiatry. Behavioural sciences/Clinical psychiatry. New York: Lippincott Williams Wilkins, [ Links ].
Sagen, U., Faerden, A., Haug, T., Melle, I., Finset, A., & Dammen, T. (2010). Are there common core features of apathy in different neuropsychiatric samples as assessed by the Apathy Evaluation Scale? Nordic Journal of Psychiatry, 64, 49-57. http://dx.doi.org/10.3109/08039480903274415 [ Links ]
Streiner, D.L., & Norman, G.R. (2003). Health measurement scales. Oxford: Medical Publications. [ Links ]
Recebido em 26 de janeiro de 2012 / Aceite em 15 de Outubro de 2012
ACKNOWLEDGEMENTS
This research was partly supported by the Fundação para a Ciência e a Tecnologia, from the PhD scholarship (ref.: SFRH/BD/22282/2005) attributed to Lara Caeiro.
The authors would like to express their gratitude to Prof. Ana Verdelho (Neurologist, Neurologic Outpatient Clinic, Hospital Santa Maria, Lisbon), and also to Dr. Daniel Barrocas, Dr. João Miguel Pereira, Dra. Manuela Silva and Dr. Diogo Guerreiro (Psychiatrists, Psychiatric Outpatient Clinic, Hospital Santa Maria, Lisbon) for their contribution, and to their patients for their voluntary contribution and participation in this study.
The authors would like to express their gratitude to Vera Caeiro and Marco Machado who translated the Apathy Evaluation Scale English version into Portuguese and retroversion of the Portuguese version into English.
