










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPsicologia
Print version ISSN 0874-2049
Psicologia vol.17 no.1 Lisboa Jan. 2003
https://doi.org/10.17575/rpsicol.v17i1.441
The primary-service-provider model for homeland community-based services
O modelo do prestador de serviços primários aplicado aos serviços ao domicílio e à comunidade
R. A. McWilliam*
*Vanderbilt University.
ABSTRACT
Home-based services are the most common method for providing early intervention in the US, yet no sound model has been articulated to date. This article proposes a model that has applicability across continents — wherever itinerant or consultative services are offered. It focuses on "integrated" services, which are based in the concept of support to the family and which use one primary service provider (i. e., a transdisciplinary model). The model is founded on the principles that (a) professionals can have more impact on adult family members than on children, (b) daily caregivers such as family members can have a more profound impact on children than can professionals, so (c) home-based services should be directed at supporting those caregivers.1
Key-words Early intervention, service delivery, home visits, model, transdisciplinary.
RESUMO
Os serviços ao domicílio são o método mais comum de realizar intervenção precoce nos EUA. Contudo, e até à data, nenhum modelo sólido de intervenção foi proposto relativamente a este problema. Este artigo propõe um modelo que pode ser aplicado trans-continentalmente - quer se trate de serviços itinerantes, quer se trate de serviços consultivos. Este modelo centra-se nos serviços "integrados", que são baseados no conceito de suporte à família e que utilizam um prestador de serviços primários (isto é, um modelo transdisciplinar). O modelo é fundamentado pelos seguintes princípios: (a) os profissionais possuem maior impacto nos membros adultos das famílias do que nas crianças; (b) os prestadores de cuidados diários, tais como os membros das famílias, podem ter um impacto mais profundo nas crianças do que os profissionais; o que leva a que (c) os serviços ao domicílio podem ser direccionados para o suporte destes prestadores de cuidados.
Albert Einstein said, "Any intelligent fool can make things bigger, more complex, and more violent. It takes a touch of genius — and a lot of courage — to move in the opposite direction. " Ignore the reference to violence, and we have a description of what has happened in early intervention services for infants, toddlers, and families. In the United States of America, home visiting, which is the major method for delivering services to children of this age, has become bigger and more complex, and families now believe that that is better (McWilliam, Tocci, & Harbin, 1998). In this paper, the traditional multidisciplinary model of providing early intervention will be contrasted with a transdisciplinary model.
Home visits have become the essence of services to young children with disabilities and their families. Sometimes these visits are actually with the family somewhere in the community and sometimes they are with the child in child care. Other aspects of early intervention, such as assessment and program planning are important, but the core of "intervention" for children who stay home (versus going to child care) is the home visit. This article defines home visits, presents models of service delivery, and describes a concept for integrated services that seeks to replace ineffective practices with those most likely to result in family empowerment and children's successful functioning. The concept hinges on "transdisciplinary" service delivery.
Definition
The transdisciplinary approach is defined as the use of a primary service provider (PSP) to delivery early intervention services. One key aspect of this approach is that the PSP supports the family in carrying out the programs designed by other members of the team. The approach is called "transdisciplinary" because the PSP supports the family on strategies coming from different disciplines. The different models of service delivery have different assumptions about how early intervention works.
Models of service delivery
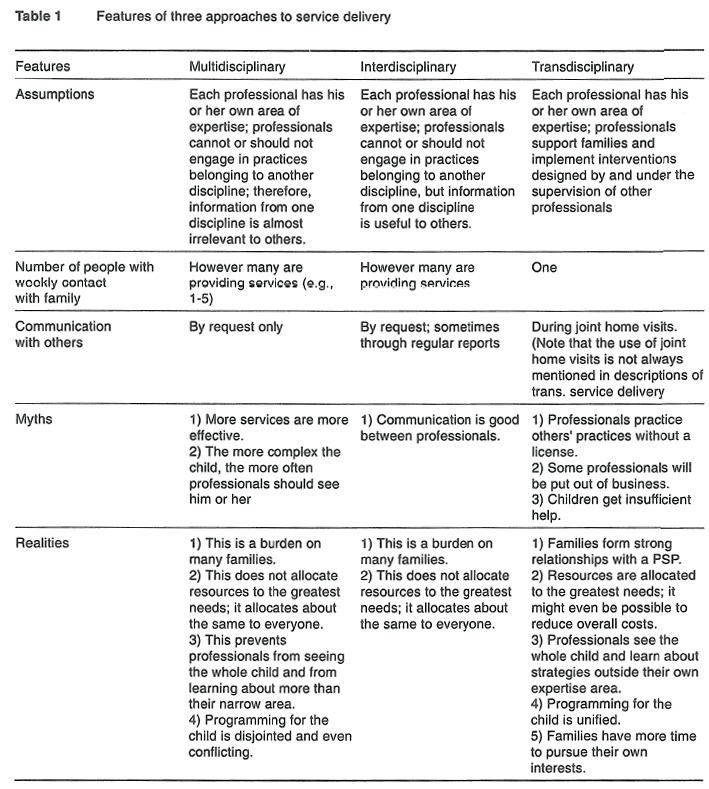
Three structures for professionals' interacting with each other have evolved in early intervention: multidisciplinary, interdisciplinary, and transdisciplinary (Chapman & Ware, 1999). In early intervention, the usual professionals are early childhood special education teachers, occupational therapists, physical therapists, speech-language pathologists, and psychologists. Table 1 shows assumptions, the number of people involved, the type of communication with others, myths, and realities for the three approaches.
Assumptions
The transdisciplinary model does not take away from professionals' having their own areas of expertise. The difference between this approach and multidisciplinary and interdisciplinary is that professionals are willing to engage in "role release" and role acceptance. Role release involves allowing other people to have information from one's own discipline and to talk to caregivers about that information. For example, a physical therapist would explain how range of motion activities work, would show someone from another discipline how to do those, and would supervise (albeit from afar) the implementation of the activities. This is how PTs work with physical therapy aides, for example. The physical therapist still conducts the assessment, designs the program, teaches caregivers and other professionals the strategies, and monitors the program.
The irony of role release. Specialists will sometimes show families what to do but will not trust other professionals with that information. For interventions to be successful, children's caregivers need to implement the activities. Specialists will, therefore, often work with families. But, if they are against multidisciplinary models, they might claim that other professionals doing the exact same thing as the families are behaving inappropriately — even unethically.
Communication
Communication among professionals is very important so families can have an integrated program for their children. The reality of everyday service delivery, however, is that professionals often do not keep each other informed, even when using an interdisciplinary model. In the transdisciplinary model, however, as I define it, specialists and the PSP make joint home visits. This allows for direct communication, without relying on written reports. The joint home visit has not been described in the literature as a critical component of transdisciplinary service delivery but it holds the most promise for effective use of this model. The assumptions behind early intervention and the importance of communication are part of the conceptual underpinnings of this model.
Conceptual framework
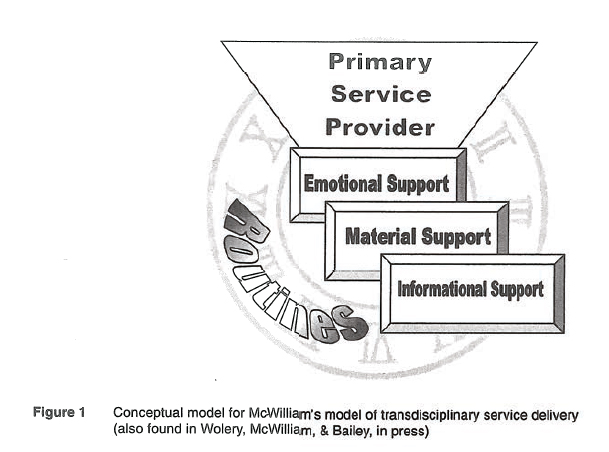
Figure 1 shows a conceptual framework for a transdisciplinary approach to home visiting and other community service provision. Such a framework is necessary to make clear the distinction between home visits as simply a location issue and home visits as a theory-based method of providing services. The first component is represented by the beveled boxes, which contain the content or "curriculum" of home and community visits. The second component is represented by the trapezoid (symbolizing a funnel), which indicates a model of service delivery. The third component is represented by the clock in the background, which symbolizes the context of the interventions — routines. In the model for community-based services described next, each of the components of the framework is explained.
A model for "integrated" services
Although much has been written about providing services in homes and communities (e.g., Bailey & Simeonsson, 1988; Coulter, 1990; Hart & Risley, 1992), about planning well with families (e.g., Johnson, McGonigel, & Kaufmann, 1989; Krauss, 1990; McWilliam, 1992), and about integrating intervention into everyday activities (e.g., McWilliam, 1995,1996; McWilliam & Sekerak, 1995), a well-formed, comprehensive model has not been described. The field has needed a model that ties together the philosophy of support, the science of early childhood learning, team functioning, and professional practice. This model is comprised of support-based services, the primary-service-provider model, and home visits themselves.
Support-based services
This three-part framework has been described as a theoretical approach to home visits (McWilliam & Scott, 2001) that recognizes (a) the potential influences of early intervention activities, (b) how children learn, and (c) the importance of what happens between visits. Some of these points are also made in the consultation chapter.
Who influences what
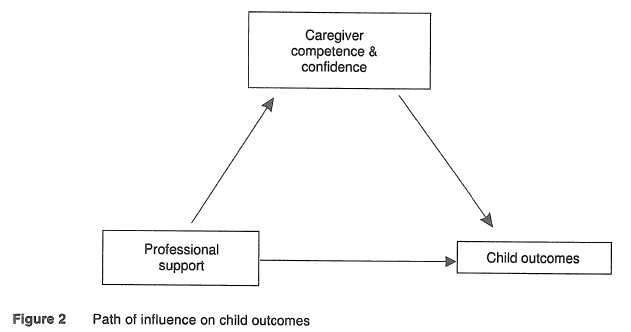
Early intervention activities with children can have only a modest effect on developmental trajectories, intelligence, motor control, and other child-level outcomes (see figure 2). These outcomes are notoriously difficult to change, and seeing a child and family for one or two sessions a week is unlikely to have too much of a direct influence on them. The family accounts for the majority of the variance in these outcomes, both through their nurturing (parenting; e.g., Steelman, Assel, Swank, Smith, & Landry, 2002) and their nature (genes). Early intervention can have considerable impact on nurturing, because the outcomes are confidence and competence. These two outcomes, unlike the child outcomes mentioned earlier, can be influenced significantly by early intervention activities. Adults' self-assurance and skill can be shaped by support from early interventionists. Those family characteristics, in turn, can have much more of an impact on children's outcomes than could weekly sessions with a child. Because of who can influence what or whom, therefore, the theoretical approach to home and community visits should consist of much attention to families' confidence and competence.
How young children learn
Young children learn through repeated interactions with their environments, dispersed over time, not through trials massed into sessions or lessons (Dunst & Bruder, 1999; Dunst, Hamby, Trivette, Raab, & Bruder, 2000; Dunst, Herter, & Shields, 2000). Each repeated practice that older children might receive in such situations adds to the child's learning. In young children, practices need to be spaced apart enough for the child to process the information. Furthermore, when the child is taught in the context of naturally occurring stimuli, the child learns to use the behavior in the relevant context. The corollary is teaching language through flash cards versus conversation. The role of the home visitor needs to reflect the reality that children learn throughout the day, whether planned or otherwise. It will emphasize support to the family to be effective teachers, rather than direct intervention with the child.
Between visits
What happens between home and community visits is, therefore, critical to children's learning. And what happens between home visits is the child's and family's routines. That is why assessment and intervention planning based on routines is so important for children's learning and development (Bernheimer & Keogh, 1995).
Types of support
The literature has backed the idea of early intervention as a venture focused on support (Dunst, Trivette, & Cross, 1986; Guralnick, 2001; Me William & Scott, 2001). Three types of support that encompass the majority of home visit practices are emotional, material, and informational support.
Emotional The importance of encouraging families is neither surprising nor new (Powell, 1987). Mothers provided with the opportunity to have a positive, trusting, and working relationship with a weekly home visitor as well as mother-infant groups have been found to score higher on measures of their experienced partner and family support than have mothers not having that support (Heinicke et al, 2001). Children in the intervention group scored higher on a strange-situation task, and their mothers were more responsive to their needs.
Professionals' behavior towards families has been included in a number of conceptualizations of early intervention services, including family-centered practices (e.g., Dunst, Johanson, Trivette, & Hamby, 1991; P. J. McWilliam & Winton, 1991; Turnbull, Turbiville, & Turnbull, 2000; Winton & Bailey, 1988), help-giving practices (Dunst, Trivette, Davis, & Cornwell, 1994), and stress-reduction approaches (McCubbin & Patterson, 1987). An example of the kinds of characteristics home visitors use to give emotional support was the finding from a qualitative study of family-centered service providers (McWilliam, Tocci, & Harbin, 1998). The five characteristics they found do not encompass all emotionally supportive practices, but they do constitute a useful framework for organizing this aspect of home and community visiting. They were positiveness, responsiveness, orientation to the whole family, and sensitivity.
Material The second type of support home visitors should be prepared to provide is material support, which is defined as ensuring families have access to the resources they need to accomplish their goals. Resources include equipment, supplies, and financial resources. Some children benefit from equipment so they can be engaged, independent, or social. Home visitors need to make sure families have such equipment. Some families need basic supplies, such as food, shelter, and clothing. They will be unlikely to take advantage of learning opportunities if they are wondering where the next meal is coming from (Maslow, 1943). Home visitors need to make sure families have access to such supplies. Some families will need financial resources from the government, which, in the U. S., are available for temporary assistance to needy families (TANF); social security income (SSI); nutrition for Women, Children, and Infants (WIC); and so on. Home visitors will need to make sure families eligible for such assistance can gain access to it.
Teachers or therapists providing home and community visits might think this material support is far outside their area of expertise. They would probably be right, which is why they should develop skills in using human resources, such social workers and other "case workers. " In the same way that a social worker might need to call a speech-language pathologist to help with a particularly thorny problem the child was having with language, the speech-language pathologist might need to call a social worker to help the family get governmental financial assistance.
Informational The third type of support Is providing information to families. In almost every study asking families what more they want from early intervention than they are currently getting, they list information (D'Amato & Yoshida, 1991; Fewell, 1986; Gowen, Christy & Sparling, 1993). There are four topics on which families often want information: the child's condition or disability, child development (including what the child should be doing at this developmental age and what will come next), resources (including services now and in the future), and what to do with the child. That last topic, hidden away in the list, actually encompasses the majority of what home visitors do. It also is the real meaning of "therapy" and "special instruction" in home and community visits.
When therapy and special instruction are viewed as informational support, professionals might be more likely to deliver the service in a way that is consistent with how children learn. For billing and other purposes, providing this information should count as reimbursable therapy or special instruction. When working with infants and preschoolers through home visits, this is how those services should be provided. For practitioners and families who fear that "just providing information" is not what early intervention is about, they can be reassured that it still involves much handling of the child. The three reasons for putting hands on a child are assessment, demonstration, and to show affection. Consequently, the home visitor might still spend most of each home and community visit handling the child.
When home visitors provide emotional support, material support, and informational support, they address many of the purposes of home-based early intervention. Who is providing this support? The integrated model features the concept of a primary service provider.
Primary-service-provider model
In addition to support-based services, the use of a primary service provider is likely to result in an efficient, family-centered service that focuses on functional needs (McCormick & Goldman, 1979; Raver, 1991). This model is controversial, mostly because of misunderstanding about how it works. To help, explanations of various terms are presented here, and concerns with implementing the model are addressed.
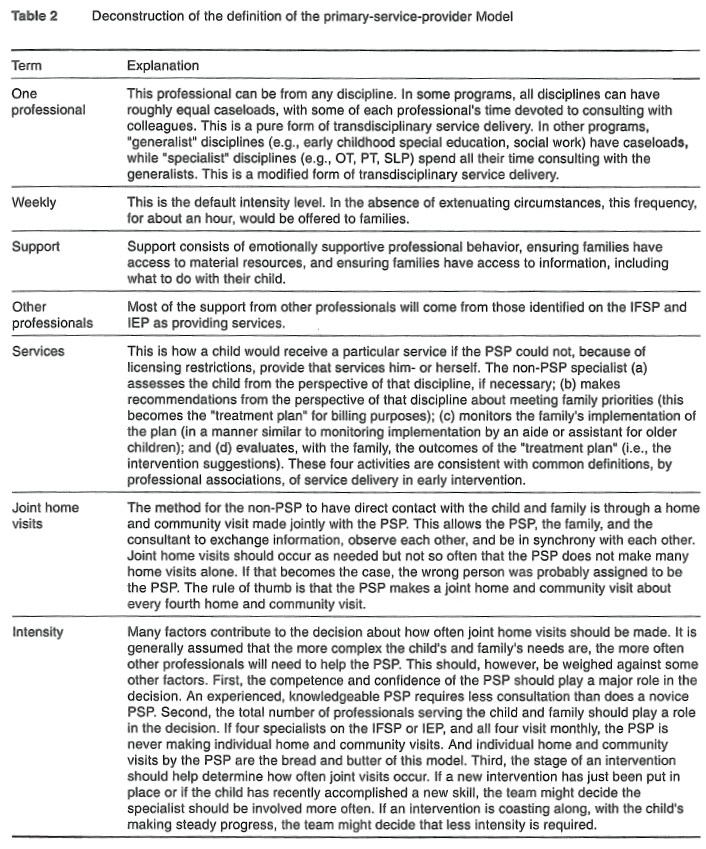
The primary-service-provider (PCP) model is defined as one professional providing weekly support to the family, backed up by a team of other professionals who provide services to the child and family through joint home visits with the primary service provider. The intensity of joint home and community visits depends on child, family, and PSP needs. table 1 deconstructs this definition. Table 2 has encapsulated the main points about the PSP also known as transdisciplinary model. Concerns about the model are as follows.
Concern 1: the model involves practicing without a license
The PSP is not practicing anything other than what he or she is qualified to practice. Supporting a family to carry out a licensed or registered specialist's program does not require a license. It is what a neighbor might do. If a PT Is the PSP, then much of his or her work would constitute practicing PT. In a modified-transdisciplinary model, however, where a generalist is the PSP, he or she is emphatically not practicing outside the area of individual expertise.
Concern 2: it is unethical for practitioners to see children so infrequently
There is no rubric for calculating the appropriate intensity of services, so there are no ethical guidelines. If someone on the team thinks a family is being seen too infrequently, that person should call1 a team meeting to resolve the issue. If a specialist insists that, ethically, he or she needs to see a family much more frequently than the rest of the team agrees upon, this might reflect this person's discomfort with the model. If he or she has a real concern about intensity, the team needs to provide an opportunity for the case to be made.
Concern 3: it is unethical for practitioners to turn over the monitoring of the program to someone else
Again, this concern usually reflects a practitioner's discomfort with the transdisciplinary approach. The monitoring of the program is still the specialist's responsibility What the PSP is doing is supporting the family in carrying out the interventions, which is different from monitoring the "treatment program, " as defined by national and state guidelines. Again, the analogy is how aides or assistants are used. Although they have frequent contact with the recipient of services (usually to provide therapy), the responsibility for monitoring the program rests with the licensed professional.
Concern 4: PSPs are unqualified to support families in carrying out specialized programs
This concern hinges on the definition of support. In this context, PSPs support families by reminding them what the specialist said, encouraging them in their implementation of the interventions, and listening to their concerns and triumphs. Experienced PSPs might suggest different ways to make the implementation of the program easier for the family, which is a sign of true partnership. Inexperienced PSPs might not be confident about any change to what the specialist has recommended. For all concerned, the more the PSP can contribute, the better.
Concern 5: one cannot be reimbursed for this model
This model is reimbursable because it is the therapists' contact time with families that third-party payers will pay for. The work of the PSP might or might not be reimbursable under any specific plan. Medicaid, for example, might cover some of those activities under "targeted case management. " Rules for reimbursement of the PSP vary enormously. Clearly, however, someone pays for home visits by generalists. In pure-transdisciplinary situations, where a therapist functions as the PSP, most of every visit can be reimbursed as therapy time. In some systems, the PSP has to bill for the time spent "providing therapy" and for the time spent in "targeted case management" separately. In general, services using the model are reimbursable.
Concern 6: families want more specialists, not fewer
It is true that families believe that more is better, when it comes to services, especially therapies (McWilliam, Young, & Harville, 1996). The critical question is why families believe this (McWilliam et al., 1998). First, professionals might teach this notion, by suggesting during planning meetings that separate needs require separate services. Second, families might think that it is the direct time that professionals spend with the child that causes positive change. In other words, they might believe that intervention for the child occurs during the home and community visit more than between it. When families are introduced to the more-is-better idea early, it is not surprising that they would endorse it. But when families are introduced to the PSP model, their expectations are different.
These concerns about the PSP model reflect the fact that it is innovative and a challenge to tradition, especially traditions so closely tied to the "therapy culture." The controversy around the service delivery model is accompanied by another controversy in early intervention generally, but one that is most often affected in home visits.
Additional questions. Two other issues need to be addressed in community-based services: the controversy of parent education and the question of whether aides are necessary. A recent clarion call for returning to the notion of parent education in early intervention (Mahoney et al., 1999) has been met with much protest (Dunst, 1999; Winton, Sloop, & Rodriguez, 1999). The main arguments have been that (a) early intervention was founded on the idea of teaching parents what to do with their children, (b) parents' interactions with their children are predictive of later functioning, and professionals can teach parents the most effect interaction styles, and (c) the field has wandered too far and that a focus on parent education will achieve the most impact.
In some parts of the country, aides are used to provide home and community visits, often because of shortages of licensed professionals. Such aides might be licensed physical therapy aides, certified occupational therapy aides, speech-language aides, or education aides. It is possible that they are used because the team believes that direct contact by a noncaregiver, even just weekly, can make a difference (which is unlikely). Although there are bound to be situations where an aide is useful, in home visits this is not likely to be true. The PSP should be a well-qualified individual, usually someone with the highest professional qualifications in his or her discipline, and the specialists are obviously licensed, registered, or certified.
Home and community visiting models can have varying conceptual bases. Although they all take place in homes and other "natural environments," they can differ considerably in their philosophical underpinnings and therefore their strategies. For heuristic purposes, the practices described here are those that place a heavy emphasis on supporting families and on efficient service delivery. Home visits themselves are the crucible in which early intervention is delivered.
Home visits themselves
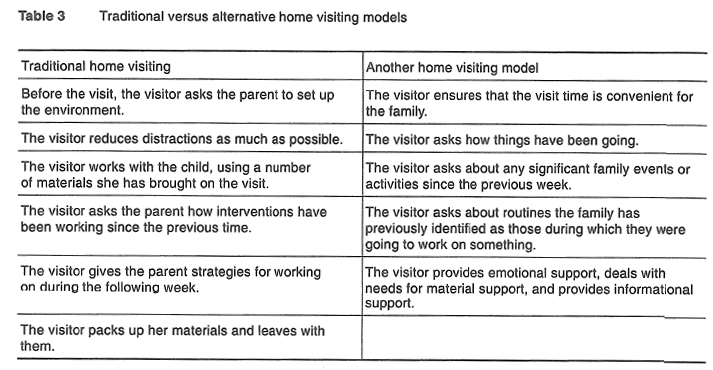
For the purposes of this article, home visiting is defined as a professional's meeting the family at a place where the family would naturally be if the child were not receiving services, such as the home or a community setting. Many home visitors see children in child care settings, which is described in the consultation chapter. Traditional home visiting will be contrasted with a support-based model here, to explain how this form of service delivery can be driven by theory Table 3 shows two approaches.
The traditional approach (a) is similar to a clinic-based approach dumped on the living room floor, (b) is based on an assumption that the home visit is the time when the child is really learning, and (c) uses an expert model of consultation (see consultation chapter). In contrast, the other approach (a) is respectful and encouraging of families, (b) ensures that families' basic needs are attended to, and (c) deals with what to do with the child. These characteristics are not necessarily mutually exclusive. Practitioners of traditional home visits can, for example, encourage families. Similarly, practitioners of support-based home visits can "work with" the child, as will be described later. Nevertheless, the traditional approach (so called because it is old and popular) is professionally driven, therapeutically oriented, and paternalistic. The alternative model is family-driven, support oriented, and family-centered. The remainder of the chapter will discuss (a) the five types of home visits, (b) support-based home visits, and (c) home visiting concerns.
Five types of home visits?
Not all home visits serve the same purpose, are aimed at the same kinds of families, or are provided by the same kinds of professionals. Five types of home visits are described.
PSP alone. In a transdisciplinary model, the PSP makes a visit by him- or herself, addressing multiple domains or areas of development. One quite-different variation on this has been visits by paraprofessionals or "lay visitors ", which has led to some confusion about the purpose and effectiveness of home visiting. Many programs using lay visitors have resulted in poor efficacy data for this model of service delivery {e.g., Schuler, Nair, & Black, 2002). Most studies decrying the effectiveness of home visits were conducted with disadvantaged children, and the home visitors were lay people (e.g., Goodson et al., 2000), public health nurses (e.g., Zahr, 2000), or others who are different from today's early intervention home visitors.
Joint home visits. Joint home visits, in which two professionals go to the home together, are used with a transdisciplinary model but could also be used as supplements to the traditional model. In a transdisciplinary model, a specialist accompanies the PSP. The purpose of the joint home visit is the exchange of information among the family, the PSP, and the specialist. The specialist is a consultant in the context.
Discipline-specific visits (without PSP). Discipline-specific visits occur all the time in multidisciplinary models and might occur occasionally in other models. On these visits, one specialist visits the family on his or her own, and the topic is limited to the area of training, licensure, expertise, or comfort of the professional. Because of this restrictiveness, it is not unusual to find that families receive multiple visits like these per week.
Visit by classroom teacher. Another type of home visit is when the classroom teacher makes a home visit (e.g., Conduct Problems Prevention Research Group, 2000). These visits typically occur very few times a year, although in some combination placements, children might be served both in a classroom and at home. Ordinarily, though, the purpose of the visit is for the professional to get to know the family and to convey information to them.
Service coordination alone. Sometimes, families have a service coordinator, whose main role is to navigate the family through the process of getting Into intervention, the process of developing an intervention plan, and securing and coordinating resources to meet the goals on the plan. The last type of home visit is that of the service coordinator's visiting, when the service coordinator is not also a PSP That is, he or she is a "designated" service coordinator, meaning he or she exclusively does service coordination, without providing other services. These visits also typically occur very few times a year and are limited to decision making and sometimes to securing resources for the family.
Each type of home visit has its distinct purpose, so what happens during the visits differs by type. The most common home visits are those by one person. Many home visitors consider an important reason for visiting families is to model for them.
Modeling
How successful is modeling for the parent? Once it is understood how young children learn, the home visitor’ might have to renegotiate existing schema about home visits. The traditional home visitor might have treated the "session" as a time to intervene intensely with the child, but, because of the way young children learn, such an approach might have been misguided. Modeling requires the 'learner" to be interested, watching, and, if possible, practicing with feedback. Simply going through activities with the child on a home visit does not necessarily constitute modeling for the family. If the family is not paying attention, perhaps not even in the room, the modeling will be to no avail. Families who are interested in having the home visitor show them how to do something will pay attention. In a study of modeling to change maternal behaviors, undergraduate nursery education students make home visits for 10 weeks to demonstrate three types of behavior while working with preschoolers: information processing, positive reinforcement, and positive control (Goodman, 1975). Modeling rapidly increased the mothers' performance of information-processing acts.
One element of a successful home visit, therefore, is the salience of the activities the home visitor proposes. Not only does the activity have to be interesting to the child — perhaps more importantly it has to be interesting to the adults who will carry out the interventions. Understanding how children learn leads to understanding the need to support families in their intervention roles.
How often does the family need modeling from a specialist? Because some specialists justify weekly home visits on the basis of the need to model, it begs the question, how often does the family need modeling form a specialist? Unfortunately, the research on modeling is very sparse. If (a) the intervention is quite complex, (b) the specialist is still assessing the child, or (c) the interventionist is inexperienced or lacks knowledge, it is possible that frequent visits are necessary. If visits are very frequent, it suggests that the PSP should be that specialist who Is needed often. It should be rare, however, for multiple professionals to need to model interventions week in and week out.
Deciding on service intensity
Once the outcomes or goals have been identified, services and resources need to be decided upon. (Note that often services are erroneously Identified on the basis of diagnosis — what a child is eligible for — not on the basis of need; Giangreco, Edelman, Luiselli, & MacFarland, 1997). Most practitioners are familiar with the idea of making these decisions on the basis of child characteristics — such as diagnosis and severity of the child's disability, but few are familiar with the making decisions on the basis of the needs of the caregiver and the PSP. If the caregiver (i. e., parents or child care providers) is confident and understands what to do with the child, specialists do not have to keep visiting week after week. If, on the other hand, the PSP is having difficulty helping the family, specialists might be needed to develop alternative programs. Perhaps the most critical issue for deciding on intensity is the confidence and competence of the PSP. Weekly home visitors who are experienced and knowledgeable will be able to understand the specialists' programs and help the family carry them out. Home visitors with little experience in this type of work, with a particular disability, or with a particular type of intervention might need more frequent visits than would the experienced PSPs. It is rare for IFSP or IEP teams to consider the home visitor's skills, but this should occur. In fact, teams usually avoid the question by simply having multiple specialists visit every week.
Implementation therefore can involve both the adoption of the PSP model and then decisions based on that person's competence and confidence. In this model, once the PSP has been identified, most specialist visits occur jointly with the PSP. The dangers of separate visits by individual specialists are (a) they tend to escalate (more and more reasons for such visits become manufactured), (b) they undermine the PSP, (c) they reinforce the notion that the visit itself is more important than what happens between visits, and (d) they underline the notion that different problems require different services (when, in fact, some do and some don't). The decisions about intensity and the policies for how the team will provide services should, therefore, be made early in the process.
Addressing concerns
The support-based home visit challenges some home visitors who are used to a more didactic, hands-on philosophy. Five concerns are addressed here: the irrelevance of the toy bag; the apparent diminishment of child-level intervention; problems with modeling; home environments; and different adult family members. How to abandon the toy bag. What's wrong with the toy bag?
— it gives the impression that the home visitor thinks the existing toys and other materials are inadequate;
— it reflects an assumption that the home visit is when learning occurs, instead of between home visits; and
— it involves assumed intervention with objects the child does not have.
Because home visitors should be affirming families, including what the child has to play with, they should use existing toys and materials. In any case, the child needs to learn to play with what is in the environment, not what Is brought in from an early intervention program. If the family and interventionist decide that a child could benefit from something the child does not have, and if such a discussion would not undermine a family's confidence, the interventionist could bring a toy for the child to try out or even keep.
Traditionally, toy bags have often constituted the home visit agenda. The home visitor goes through the different activities with the child. Adult family members have either watched or participated. Another option some families have chosen is to attend to other things while the home visitor is "working with the child. " Ironically, those home visitors are likely to say that such parents are not "involved. " In the support based model, (a) the home visitor is visiting the adult family members, (b) talks through interventions with the family, and (c) demonstrates interventions with the child. Consequently, such families do not wander off or stop paying attention.
A conversation about routines and other matters replaces the toy bag as the agenda for home visits. The following kinds of questions are appropriate:
— how have things been going?
— what about breakfast, getting people out of the house, the hours from Hell, etc. ?
— what did you do last weekend?
— did you have any appointments? Any coming up?
— is there a time of day that's not going well for you?
— in the past week, what time of day has been going well (with or without the child!)
— do you have enough to do with your child? Too much?
This kind of conversation might seem too simple, but the skilled home visitor asks appropriate follow-up questions and the answers lead to all kinds of activities. They lead to the home visitor's talking, showing, and reviewing.
What about child-level intervention? Professionals who are used to "teaching" or "providing therapy" on home visits might be concerned about the role of child-level intervention. Actually, the most effective child-level intervention on home visits is carried out through and by the adult family members. The difference between the old and new models is that in the new model the home visitor is not responsible for the actual implementation of the interventions, just helping to design them with the family.
Frequently, the home visitor ends up demonstrating for the family, but demonstration should be used judiciously. When it becomes apparent that a child isn't doing something as desired, and the parent wants help, the home visitor makes suggestions. If the parent wants to be shown what to do, or the home visitor can't clearly describe what to do, the home visitor can model.
What are the three reasons for putting your hands on a child? Modeling for the family is one of three reasons for handling children on home visits. The other two are to assess the child and to be affectionate with the child. Assessing the child while physically interacting with him or her would be as part of functional or dynamic assessment rather than as part of formal, standardized testing. Showing affection is important when working with small children and when establishing positive relationships with families.
When do you need a specialist to consult with a family about a problem? Child-level interventions are happening all the time, whether we like it or not, because families are interacting with their children. The children are learning from those interactions. The regular home visitor {e.g., the PSP) should have enough expertise to guide families about interactions and interventions that cut across diagnostic types, across ages, and across families. They should know about normal development, about analyzing behavior, and about the basics of most disabilities. When a question outside these parameters arises, home visitors should obtain consultation from specialists. If specialists on the team are concerned that the home visitor might now know when to call them for consultation, they should advocate for periodic check-ins with the family through joint home visits with the PSP. In general, therefore, child-level intervention is still a central part of home visits. It is simply that a professional's direct intervention with the child is not as important as the professional's intervention with the caregivers who spend enough time with the child to make a difference.
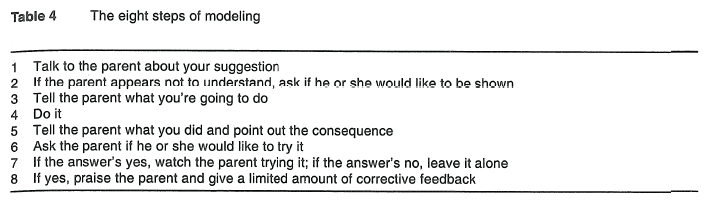
The eight steps of modeling: avoiding the model-&-pray approach. Consultation with families on home visits often involves modeling, but how effective those models are is questionable. Home visitors often sense that the models they have provided the week before have not been imitated. Many home visitors have used the model-and-pray approach, where they "modeled" and prayed that the family would spontaneously imitate the modeled intervention. A more effective approach would be to use modeling methodically. Table 4 shows eight simple steps that should be followed in a naturalistic and easy way.
These eight steps (a) ensure that the family is really interested in the intervention; (b) give the family two input modes, visual and auditory; and (c) give the family the opportunity to practice.
The inherent challenges of home visits. Home visits come with challenges. Some homes are very chaotic and some are very dirty. Sometimes, people the home visitor does not know are present. Sometimes, despite the home visitor's best practices, the parent will be distracted. And sometimes, pets, other children, and other adults will become involved.
Families themselves. Any time professionals are working with families, they need to be prepared for all sorts of situations. Because early intervention occurs at a time in a family's development that is intense and unfamiliar, home visitors encounter many reactions to them and to home visits. Families can be happy, distrustful, upset (sad, worried), angry, intense, and uninterested. By and large, however, families enjoy their home visits and love their home visitors. Home visitors, therefore, have a considerable responsibility to return that trust and affection.
Home visits can thus be centered around the provision of emotional, material, and informational support. This can be done by integrating specialized services in the PSP model, which is based on the recognition that intervention is what the child receives from the people who spend significant amounts of time with him or her. With the realization that this is the most common form of service delivery for infants and toddlers with disabilities and their families, it is important to carry it out with competence, knowledge of child development and family functioning, and common sense.
References
Bailey, D. B., & Simeonsson, R. J. (1988). Home-based early interventions. In S. L. Odom & M. B. Karnes (Eds.), Early intervention for infants and children with handicaps (pp. 199-216). Baltimore: Paul H. Brookes. [ Links ]
Bernheimer, L. P., & Keogh, B. K. (1995). Weaving interventions into the fabric of everyday life: An approach to family assessment. Topics in Early Childhood Special Education, 15,415-533. [ Links ]
Chapman, L., & Ware, J. (1999). Challenging traditional roles and perceptions: Using a transdisciplinary approach in an inclusive mainstream school. Support for Learning, 14,104-109. [ Links ]
Conduct Problems Prevention Research Group (2000). Initial impact of the fast track prevention trial for conduct problems: I — The high-risk sample. Journal of Consulting and Clinical Psychology, 67, 631-647. [ Links ]
Coulter, D. (1990). Home is the place: Quality of life for young children with developmental disabilities. In R. Schalock & M. J. Bogale (Eds.), Quality of life: Perspectives and issues (pp. 61-70). Washington, DC: American Association of Mental Retardation.
D'Amato, E., & Yoshida, R. K. (1991). Parental needs: An educational life cycle perspective. Journal of Early Intervention, 15, 246-254. [ Links ]
Dunst, C. J. (1999). Placing parent education in conceptual and empirical context. Topics in Early Childhood Special Education, 19,141-147. [ Links ]
Dunst, C. J., & Bruder, M. B. (1999). Increasing children's learning opportunities in the context of family and community life. Children's Learning Opportunities Report, 1, http://www.puckett.org/childleam/L.O._Newsletter_Vol.1,1.htm. [ Links ]
Dunst, C. J., Hamby, D., Trivette, C. M., Raab, M., & Binder, M. B. (2000). Everyday family and community life and children's naturally occurring learning opportunities. Journal of Early Intervention, 23,151-164. [ Links ]
Dunst, C. J., Herter, S., & Shields, H. (2000). Interest-based natural learning opportunities. In S. Sandall & M. Ostrosky (Eds.), Young exceptional children monograph series no. 2: Natural environments and inclusion (pp. 37-48). Denver, CO: The Division for Early Childhood of the Council for Exceptional Children.
Dunst, C. J., Johanson, C., Trivette, C. M., & Hamby, D. W. (1991). Family-oriented early intervention policies and practices: Family-centered or not? Exceptional Children, 58,115-126. [ Links ]
Dunst, C. J., Trivette, C. M., & Cross, A. H. (1986). Mediating influences of social support: Personal, family, and child outcomes. American Journal of Mental Deficiency, 90, 403-417. [ Links ]
Dunst, C. J., Trivette, C. M., Davis, M., & Cornwell, J. C. (1994). Characteristics of effective help-giving practices. In C. J. Dunst, C. M. Trivette, & A. G. Deal (Eds.), Supporting and strengthening families, Vol. 1: Methods, strategies and practices (pp. 171-186). Cambridge, MA: Brookline Books.
Fewell, R. R. (1986). Supports from religious organizations and personal beliefs. In R. R. Fewell & P. R Vadasy (Eds.), Families of handicapped children: Needs and supports across the life span (pp. 297-316). Austin, TX: Pro-Ed.
Giangreco, M. F., Edelman, S. W., Luiselli, T. E., MacFarland, S. Z. C. (1996). Support service decision making for students with multiple service needs: Evaluative data. Journal of the Association for Persons with Severe Handicaps, 21,135-144, [ Links ]
Goodman, E. O. (1975). Modeling: A method of parent education. Family Coordinator, 24, 7-11. [ Links ]
Goodson, B. D., Layzer, J. L, St Pierre, R. G., Bernstein, L. S., & Lopez, M. (2000). Effectiveness of a comprehensive, five-year family support program for low-income children and their families: Findings from the comprehensive child development program. Early Childhood Research Quarterly, 15,5-39. [ Links ]
Gowen, J. W., Christy, D. S., & Sparling, J. (1993). Informational needs of parents of young children with special needs. Journal of Early Intervention, 17,194-210. [ Links ]
Guralnick, M. J. (2001). A framework for change in early childhood inclusion. In M. J.
Guralnick (Ed.), Early childhood inclusion: Focus on change (pp. 3-38). Baltimore, MD: Paul H. Brookes Publishing Co.
Hart, B., & Risley, T. (1992). American parenting of language-learning children: Persisting differences in family-child interactions observed in natural home environments. Developmental Psychology, 28 (6), 1096-1105. [ Links ]
Heinicke, C. M., Reinman, N. R., Ponce, V. A., & Guthrie, D. (2001). Relation-based intervention with at-risk mothers: Outcome in the second year of life. Infant Mental Health Journal, 22,431-462. [ Links ]
Johnson, B. H., McGonigel, M. J., & Kaufmann, R. K. (1989). Guidelines and recommended practices for the individualized family service plan. Chapel Hill, NC, & Washington, DC: NEC*TAS and ACCH. [ Links ]
Krauss, M. W. (1990). New precedent in family policy: Individualized family service plan. Exceptional Children, 56,388-395. [ Links ]
Mahoney, G., Kaiser, A., Girolametto, L., MacDonald, J., Robinson, C, Safford, R, & Spiker, D. (1999). Parent education in early intervention: A call for a renewed focus. Topics in Early Childhood Special Education, 19,131-140. [ Links ]
Maslow, A. H. (1943). A theory of human motivation. Psychological Review, 50, 370-396. [ Links ]
McCormick, L., & Goldman, R. (1979). The transdisciplinary model: Implications for service delivery and personnel preparation for the severely and profoundly handicapped. AAESPH Review, 4,152-161. [ Links ]
McCubbin, H. L, & Patterson, J. M. (1987). Family inventory of life events and changes. In H. M. McCubbin & A. I. Thompson (Eds.), Family assessment inventories for research and practice (pp. 79-98). Madison: University of Wisconsin-Madison. [ Links ]
McWilliam, P. J., & Winton, P. J. (1991). Brass tacks. Unpublished instrument. Frank Porter Graham Child Development Center, University of North Carolina, Chapel Hill, [ Links ] NC.
McWilliam, R. A. (1992). Family-centered intervention planning: A routines-based approach. Tucson, AZ: Communication Skill Builders.
McWilliam, R. A. (1995). Integration of therapy and consultative special education: A continuum in early intervention. Infants and Young Children, 7 (4), 29-38. [ Links ]
McWilliam, R. A. (1996). A program of research on integrated versus isolated treatment in early intervention. In R. A. McWilliam (Ed.), Rethinking pull-out services in early intervention: A professional resource (pp. 49-70). Baltimore, MD: Paul H. Brookes.
McWilliam, R. A., & Scott, S. (2001). A support approach to early intervention: A three-part framework. Infants & Young Children, 13 (4), 55-66. [ Links ]
McWilliam, R. A., & Sekerak, D. (1995). Integrated practices in center-based early intervention: Perceptions of physical therapists. Pediatric Physical Therapy, 7, 51-58. [ Links ]
McWilliam, R. A., Tocci, L., & Harbin, G. L. (1998). Family-centered services: Service providers' discourse and behavior. Topics in Early Childhood Special Education, 18,206-221. [ Links ]
McWilliam, R. A., Young, H. J., & Harville, K. (1996). Therapy services in early intervention: Current status, barriers, and recommendations. Topics in Early Childhood Special Education, 16, 348-374. [ Links ]
Powell, D. R. (1987). Life in a parent support program: Research perspectives. Family Resource Coalition Report, 6 (3), 4-5,18. [ Links ]
Raver, S. A. (1991). Strategies for teaching at-risk and handicapped infants and toddlers: A transdisciplinary approach. Nova lorque: Macmillan. [ Links ]
Schuler, M. E., Nair, R, & Black, M. M. (2002). Ongoing maternal drug use, parenting attitudes, and home intervention: Effects on mother-child interaction at 18 months. Journal of Development and Behavioral Pediatrics, 23, 87-94. [ Links ]
Steelman, L. M., Assel, M. A., Swank, P. R., Smith, K. E., & Landry, S. H. (2002). Early maternal warm responsiveness as a predictor of child social skills: Direct and indirect paths of influence over time. Journal of Applied Developmental Psychology, 23,135-156. [ Links ]
Stone, W. L., & Yoder, P. J. (2001). Predicting spoken language level in children with autism spectrum disorders. Autism, 5,341-361. [ Links ]
Turnbull, A. R, Turbiville, V., & Turnbull, H. R. (2000). Evolution of family-professional models: Empowerment as the model for the early 21st century. In S. J. Meisels, & J. P. Shonkoff (Eds.), Handbook of early intervention (pp. 630-650). Cambridge, MA: Cambridge University Press.
Winton, P. J., & Bailey, D. B. (1988). The family-focused interview: A collaborative mechanism for family assessment and goal-setting. Journal of the Division for Early Childhood, 12,195-207. [ Links ]
Winton, R J., Sloop, S., & Rodriguez, P. (1999). Parent education: A term whose time is past. Topics in Early Childhood Special Education, 19,157-161. [ Links ]
Zahr, L. K. (2000). Home-based intervention after discharge for Latino families of low-birth-weight infants. Infant Mental Health Journal, 21,448-463. [ Links ]
Notes
1Much of the material in this article is taken from a chapter by the author to appear in M. Wolery, R. A. McWilliam, & D. B. Bailey, Jr. (Eds.), Teaching infants and preschoolers with disabilities. Columbus, OH: Merrill.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}