










Serviços Personalizados
Journal
Artigo
 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de Enfermagem Referência
versão impressa ISSN 0874-0283versão On-line ISSN 2182-2883
Rev. Enf. Ref. vol.serV no.3 Coimbra jul. 2020
EDITORIAL
Editorial
Programas de autocuidado y rol de la enfermería para mejorar los resultados clínicos en pacientes con insuficiencia cardiaca
La insuficiencia cardiaca (IC) ha sido descrita como un problema de salud pública global, por sus altos costos de tratamiento, con un gasto de 108 billones de dólares estadounidenses anuales; el impacto social por su incremento en la población mayor, y el hecho de pertenecer al grupo de las enfermedades no transmisibles, principales causantes de muertes en el mundo, lo que genera una millonaria carga económica anual en el sector sanitario, representada en el 1-2% del presupuesto destinado a la atención médica (Lesyuk, Kriza, & Kolominsky-Rabas, 2018). Cabe señalar que la tasa de prevalencia de la enfermedad es de 124 por cada 10.000 personas, siendo 9,2 veces más frecuente en adultos mayores de 65 años; y la tasa de incidencia oscila entre 24 y 38 por cada 10.000 habitantes (Lesyuk et al., 2018). Se ha estimado que en 2016 había más de 26 millones de personas en el mundo afectadas con este síndrome crónico, de las cuales 5,7 millones correspondían a Estados Unidos. Se espera que para 2030, la cifra en este país ascienda a más de 8 millones de personas (Savarese & Lund, 2017).
La IC trae como consecuencia que disminuya la calidad de vida y se pierdan muchos años de vida productiva, pues esta enfermedad no le permite al paciente continuar con su vida cotidiana, debido a que se le dificulta más de lo normal realizar tareas básicas como alimentarse, desplazarse o actividades rutinarias dentro de su entorno familiar, laboral y social; además del componente psicológico, que puede verse afectado, llegando al punto de tener que depender de un cuidador, lo cual puede ser atendido a través de programas educativos y de seguimiento donde se fomente la adquisición de habilidades de autocuidado (Cañon-Montañez et al., 2013).
En este contexto, es importante mencionar que la educación al paciente puede ser definida como un proceso que mejora el conocimiento y las habilidades que influyen en las actitudes que el paciente requiere para mantener un comportamiento adecuado en bien de su salud. La educación dirigida a los pacientes incluye: educación sobre la terapia o el tratamiento, educación sobre aspectos clínicos y educación sobre promoción de la salud (Strömberg, 2005). La educación es una parte fundamental en el proceso de aprender a mantener el bienestar físico y emocional en los pacientes con IC, mediante el cual se puede dar a conocer los elementos más importantes relacionados para la práctica del autocuidado, entendiendo esta como toda acción positiva que realiza el paciente para mejorar sus condiciones de salud, de manera consciente y perdurable, y convirtiendo estos actos en una conducta aprendida para hacer frente a su enfermedad de manera eficaz y con el fin de llevarla de la mejor manera posible (Olivella, Bonilla, & Bastidas, 2012).
La educación a los pacientes es uno de los roles profesionales de los enfermeros. Los enfermeros tienen un gran potencial para ofrecer educación a pacientes con enfermedades crónicas, por lo que se convierten en los proveedores primarios del cuidado de la salud de las personas. La educación del paciente por el profesional de enfermería sigue dos orientaciones: una, de acción instrumental, que influye en la actitud y el comportamiento del paciente; la otra, de protección, que tiene la intención de minimizar la aprehensión del paciente con el tratamiento. El proceso de educación puede ser descrito en cinco pasos: 1) evaluación del conocimiento previo, la cognición, las actitudes, la motivación y los errores cometidos por los pacientes en su tratamiento; 2) identificar lo que se debe enseñar, considerando las potenciales barreras para el aprendizaje; 3) planificación del contenido de la educación, con participación del paciente para definir objetivos individuales y escoger las mejores intervenciones para alcanzarlos; 4) planificación del modo como la educación será brindada; 5) la evaluación crítica del proceso de educación establecida (Strömberg, 2005; Rabelo, Aliti, Domingues, Ruschel, & Brun, 2007).
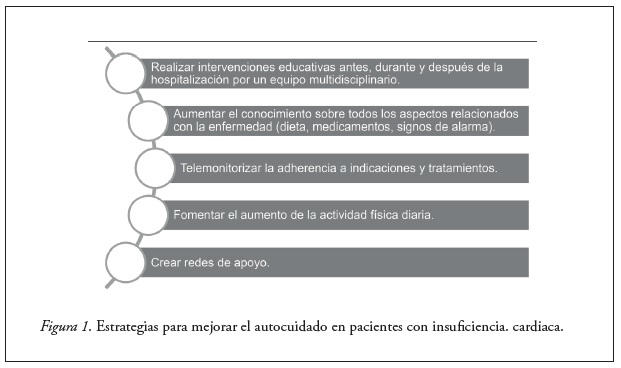
El compromiso del enfermo en el proceso educativo es un factor primordial para asegurar la adherencia al tratamiento. Cuando los pacientes entienden los factores que ayudan a su recuperación y cómo pueden ser modificados por ellos mismos en sentido favorable, es más eficaz la terapia (Cañon-Montañez et al., 2013). La instrucción básica comprende informar al enfermo y a su cuidador sobre qué es la IC, qué ha causado que su corazón falle, cómo aliviar el trabajo cardiaco controlando el peso, la ingesta de sal y los líquidos, cuáles son los signos precoces de descompensación y qué hacer cuando aparecen (Rabelo et al., 2007; Strömberg, 2005). De manera que es muy importante que la educación que se brinde al paciente se base en su capacidad de entendimiento, además de que se repita de forma reiterativa para afianzar el logro de habilidades de autocuidado (Rabelo et al., 2007), y también es crucial tener en cuenta las barreras de aprendizaje que se puedan presentar en el paciente, como edad, comorbilidades, limitaciones funcionales o cognitivas (Strömberg, 2005). Desde luego, es ideal que se realice un plan de cuidado personalizado, donde se promuevan los hábitos de vida saludable de acuerdo con su cultura, género, condición, comorbilidades y condiciones socioeconómicas, y de esta manera favorecer la adaptación a los nuevos cambios y evitar que este plan sea abandonado en el transcurso del tiempo. La figura 1 relaciona posibles estrategias para mejorar el autocuidado en pacientes con IC.
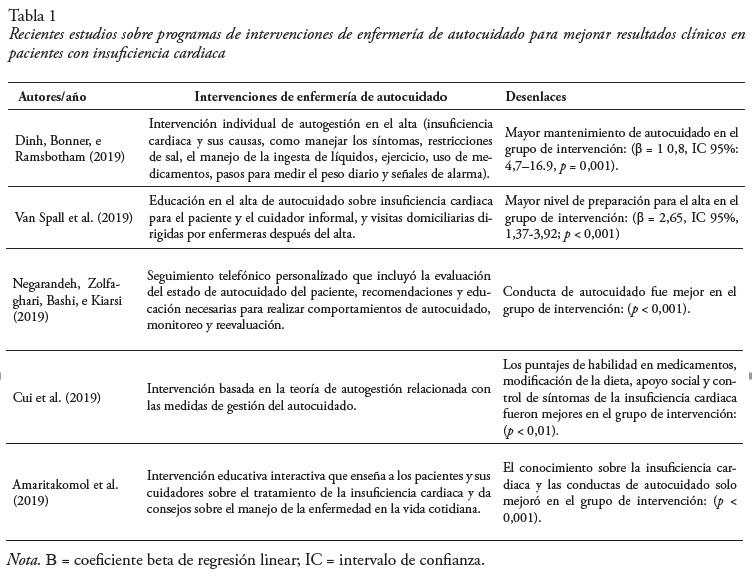
Con todo lo anterior, es fundamental recalcar que las intervenciones educativas del profesional de enfermería deben estar enfocadas a la detección temprana de signos de alarma, a la educación sobre estilos de vida saludable, a la elaboración de un plan de cuidado de acuerdo con las necesidades de cada persona, la resolución de cualquier duda que tenga el paciente o su familia con respecto a la enfermedad, el acompañamiento físico y emocional en cada etapa y, sobre todo, es vital que realice un seguimiento después del alta hospitalaria, con el fin de reducir los efectos negativos que puedan surgir al no seguir las indicaciones del equipo multidisciplinario de atención, como reingresos hospitalarios, disminución de la calidad de vida y la muerte. La tabla 1 muestra estudios de intervención recientes sobre programas de autocuidado de enfermería con resultados significativos para la mejoría de desenlaces clínicos en pacientes con IC.
La mayoría de las intervenciones fueron realizadas en escenarios de programas multidisciplinarios (clínicas de insuficiencia cardiaca) con estrategias de visita domiciliaria y/o educación prealta en el hospital. Los programas educativos fueron centrados en conocimiento, desarrollo de habilidades y conductas de autocuidado (Amaritakomol et al., 2019; Cui et al., 2019; Dinh et al., 2019; Negarandeh et al., 2019; Van Spall et al., 2019).
Se puede concluir que es importante conocer las intervenciones de seguimiento, cuidado y educación que se están realizando en torno al cuidado de los pacientes con IC, que buscan alcanzar oportunidades de mejora y, de esta manera, aumentar la calidad de vida de esta población. Sin embargo, aún hay poca evidencia que evalúe el efecto combinado de las intervenciones educativas centradas en programas de autocuidado. La realización de una síntesis actualizada de la evidencia podría contribuir a comprender mejor el impacto de estos estudios para mejorar los resultados clínicos de los pacientes con IC.
Referencias
Amaritakomol, A., Kanjanavanit, R., Suwankruhasn, N., Topaiboon, P., Leemasawat, K., Chanchai, R., . . . Phrommintikul, A. (2019). Enhancing knowledge and self-care behavior of heart failure patients by interactive educational board game. Games for Health Journal, 8(3), 177-186. doi:10.1089/g4h.2018.0043 [ Links ]
Cañon-Montañez, W., & Oróstegui Arenas, M. (2013). Intervenciones educativas de enfermería en pacientes ambulatorios con falla cardiaca. Enfermería Global, 12(3), 52-67. doi:10.6018/eglobal.12.3.160411 [ Links ]
Cui, X., Zhou, X., Ma, L.-l., Sun, T.-W., Bishop, L., Gardiner, F. W., & Wang, L. (2019). A nurse-led structured education program improves self-management skills and reduces hospital readmissions in patients with chronic heart failure: A randomized and controlled trial in China. Rural and Remote Health, 19(2), 5270. doi:10.22605/RRH5270 [ Links ]
Dinh, H. T., Bonner, A., Ramsbotham, J., & Clark, R. (2019). Cluster randomized controlled trial testing the effectiveness of a self-management intervention using the teach-back method for people with heart failure. Nursing & Health Sciences, 21(4), 436-444. doi:10.1111/nhs.12616 [ Links ]
Lesyuk, W., Kriza, C., & Kolominsky-Rabas, P. (2018). Cost-of-illness studies in heart failure: A systematic review 2004–2016. BMC Cardiovascular Disorders, 18(1), 74. doi:10.1186/s12872-018-0815-3 [ Links ]
Negarandeh, R., Zolfaghari, M., Bashi, N., & Kiarsi, M. (2019). Evaluating the effect of monitoring through telephone (tele-monitoring) on self-care behaviors and readmission of patients with heart failure after discharge. Applied Clinical Informatics, 10(2), 261-268. doi:10.1055/s-0039-1685167 [ Links ]
Olivella, M., Bonilla, C. P., & Bastidas, C. V. (2012). Fomento del autocuidado en la insuficiencia cardiaca. Enfermería Global, 11(25), 282-286. doi:10.4321/S1695-61412012000100017 [ Links ]
Rabelo, E. R., Aliti, G. B., Domingues, F. B., Ruschel, K. B., & Brun, A. O. (2007). What to teach to patients with heart failure and why: The role of nurses in heart failure clinics. Revista Latino-Americana de Enfermagem, 15(1), 165-170. doi:10.1590/S0104-11692007000100024 [ Links ]
Savarese, G., & Lund, L. H. (2017). Global public health burden of heart failure. Cardiac Failure Review, 3(1), 7-11. doi:10.15420/cfr.2016:25:2 [ Links ]
Strömberg, A. (2005). The crucial role of patient education in heart failure. European Journal of Heart Failure, 7(3), 363-369. doi:10.1016/j.ejheart.2005.01.002 [ Links ]
Van Spall, H. G., Lee, S. F., Xie, F., Oz, U. E., Perez, R., Mitoff, P. R., … Connolly, S. J. (2019). Effect of patient-centered transitional care services on clinical outcomes in patients hospitalized for heart failure: The PACT-HF randomized clinical trial. Journal of the American Medical Association, 321(8), 753-761. doi:10.1001/jama.2019.0710
Wilson Cañon-Montañez
Facultad de Enfermería
Universidad de Antioquia
Medellín, Colombia
E-mail: wilson.canon@udea.edu.co
Mónica López de Ávila
Facultad de Enfermería
Universidad de Antioquia
Medellín, Colombia
Alba Luz Rodríguez-Acelas,
Facultad de Enfermería
Universidad de Antioquia
Medellín, Colombia
Self-care programs and the role of nursing in improving clinical outcomes in patients with heart failure
Heart failure (HF) has been described as a global public health problem due to its high treatment costs, with an annual expenditure of $108 billion, the social impact due to the increase in population aging, and the fact that it is a non-communicable disease, the main cause of death in the world, thus generating a millionaire annual economic burden in the health sector, represented by 1-2% of the budget allocated to medical care (Lesyuk, Kriza, & Kolominsky-Rabas, 2018). It should be noted that the prevalence rate of this disease is 124 per 10,000 people, being 9.2 times more frequent in older adults over 65. The incidence rate varies between 24 and 38 per 10,000 inhabitants (Lesyuk et al., 2018). It has been estimated that, in 2016, more than 26 million people in the world suffered from this chronic syndrome, of which 5.7 million were located in the United States. It is expected that, by 2030, the figure in this country will be more than 8 million people (Savarese & Lund, 2017).
HF results in a decrease in quality of life and the loss of many years of productive life. This disease does not allow the patient to continue with his/her daily life because carrying out basic tasks becomes more difficult, such as feeding, moving, or routine activities within the family, work and social context. Besides, the psychological component may be affected, possibly leading to dependence on a caregiver, a need which can be met through educational and monitoring programs that encourage the acquisition of self-care skills (Cañon-Montañez et al., 2013).
Within this scope, it should be noted that patient education can be defined as a process that improves the necessary knowledge and skills for the patient to maintain an appropriate behaviour to his/her health. Patient education focuses on therapy or treatment, clinical aspects, and health promotion (Strömberg, 2005). Education is a key part of the process of learning how to maintain the physical and emotional well-being of patients with HF, providing information on the most important elements related to self-care. Self-care is considered as any positive action that the patient carries out to improve his/her health conditions, consciously and lastingly, converting these acts into a learned behaviour to deal with his/her illness effectively and to manage it in the best possible way (Olivella, Bonilla, & Bastidas, 2012).
Patient education is one of the responsibilities of the nursing profession. Nurses are well-placed to provide education to patients with chronic diseases as they become the health professionals that provide primary care to people. Nurse-led patient education follows two guidelines: one of effective action, which influences the patient’s attitude and behaviour; the other of protection, aiming to minimize the patient’s apprehension about treatment. The educational process can be described in five steps: 1) assessment of prior knowledge, cognition, attitudes, motivation, and mistakes made by patients in their treatment; 2) identification of what should be taught, considering the potential barriers to learning; 3) planning of educational content, with the participation of the patient to define individual goals and choose the best interventions to achieve them; 4) planning how the education will be provided; 5) critical evaluation of the established educational process (Strömberg, 2005; Rabelo, Aliti, Domingues, Ruschel, & Brun, 2007).
The patient’s commitment to the educational process is essential to ensure adherence to treatment. When patients understand the factors that help their recovery and how they can change them in their favor, therapy is more effective (Cañon-Montañez et al., 2013). Basic education includes informing the patient and his/her caregiver about what HF is, what has caused his/her heart to fail, how to relieve the cardiac workload with weight control, salt restrictions, and fluid intake management, what the early signs of decompensation are, and what to do when they appear (Rabelo et al., 2007; Strömberg, 2005). Therefore, patient education should take into account his/her capacity to understand and be reinforced and continuous to promote the acquisition of self-care skills (Rabelo et al., 2007). It is also crucial to consider the learning barriers that the patient may face, such as age, comorbidities, functional or cognitive limitations (Strömberg, 2005). Indeed, developing a personalized care plan is paramount so that healthy living habits are promoted according to the patient’s culture, gender, health status, comorbidities, and socioeconomic conditions, favouring adaptation to new changes and preventing abandonment of the care plan over time. Figure 1 shows possible strategies for improving self-care in patients with HF.
Therefore, it should be noted that nurses’ education should focus on early detection of warning signs, education about healthy lifestyles, development of a care plan according to the needs of each person, solving the patient’s and family’s doubts relating to the disease, physical and emotional monitoring at each stage. Above all, it is vital that the patient post-discharge follow-up care to reduce the negative effects that may result from disregarding the indications of the multidisciplinary care team, such as hospital readmissions, reduced quality of life, and death. Table 1 shows recent intervention studies on nursing self-care programs with significant results for the improvement of clinical outcomes in patients with HF.
Most interventions were conducted in multidisciplinary program settings (heart failure clinics) with home visiting strategies and/or pre-discharge education. The educational programs focused on knowledge, skill development, and self-care behaviours (Amaritakomol et al., 2019; Cui et al., 2019; Dinh et al., 2019; Negarandeh et al., 2019; Van Spall et al., 2019).
In conclusion, it is important to know which follow-up, care, and educational interventions are being carried out regarding the care to patients with HF, with a view to promoting opportunities for improvement and thus increasing the quality of life of this population. However, there is still little evidence that allows assessing the combined effect of educational interventions focused on self-care programs. An updated synthesis of the evidence could contribute to a better understanding of the impact of these studies so as to improve the clinical outcomes of patients with HF.
References
Amaritakomol, A., Kanjanavanit, R., Suwankruhasn, N., Topaiboon, P., Leemasawat, K., Chanchai, R., . . . Phrommintikul, A. (2019). Enhancing knowledge and self-care behavior of heart failure patients by interactive educational board game. Games for Health Journal, 8(3), 177-186. doi:10.1089/g4h.2018.0043
Cañon-Montañez, W., & Oróstegui Arenas, M. (2013). Intervenciones educativas de enfermería en pacientes ambulatorios con falla cardiaca. Enfermería Global, 12(3), 52-67. doi:10.6018/eglobal.12.3.160411
Cui, X., Zhou, X., Ma, L.-l., Sun, T.-W., Bishop, L., Gardiner, F. W., & Wang, L. (2019). A nurse-led structured education program improves self-management skills and reduces hospital readmissions in patients with chronic heart failure: A randomized and controlled trial in China. Rural and Remote Health, 19(2), 5270. doi:10.22605/RRH5270
Dinh, H. T., Bonner, A., Ramsbotham, J., & Clark, R. (2019). Cluster randomized controlled trial testing the effectiveness of a self-management intervention using the teach-back method for people with heart failure. Nursing & Health Sciences, 21(4), 436-444. doi:10.1111/nhs.12616
Lesyuk, W., Kriza, C., & Kolominsky-Rabas, P. (2018). Cost-of-illness studies in heart failure: A systematic review 2004–2016. BMC Cardiovascular Disorders, 18(1), 74. doi:10.1186/s12872-018-0815-3
Negarandeh, R., Zolfaghari, M., Bashi, N., & Kiarsi, M. (2019). Evaluating the effect of monitoring through telephone (tele-monitoring) on self-care behaviors and readmission of patients with heart failure after discharge. Applied Clinical Informatics, 10(2), 261-268. doi:10.1055/s-0039-1685167
Olivella, M., Bonilla, C. P., & Bastidas, C. V. (2012). Fomento del autocuidado en la insuficiencia cardiaca. Enfermería Global, 11(25), 282-286. doi:10.4321/S1695-61412012000100017
Rabelo, E. R., Aliti, G. B., Domingues, F. B., Ruschel, K. B., & Brun, A. O. (2007). What to teach to patients with heart failure and why: The role of nurses in heart failure clinics. Revista Latino-Americana de Enfermagem, 15(1), 165-170. doi:10.1590/S0104-11692007000100024
Savarese, G., & Lund, L. H. (2017). Global public health burden of heart failure. Cardiac Failure Review, 3(1), 7-11. doi:10.15420/cfr.2016:25:2
Strömberg, A. (2005). The crucial role of patient education in heart failure. European Journal of Heart Failure, 7(3), 363-369. doi:10.1016/j.ejheart.2005.01.002
Van Spall, H. G., Lee, S. F., Xie, F., Oz, U. E., Perez, R., Mitoff, P. R., … Connolly, S. J. (2019). Effect of patient-centered transitional care services on clinical outcomes in patients hospitalized for heart failure: The PACT-HF randomized clinical trial. Journal of the American Medical Association, 321(8), 753-761. doi:10.1001/jama.2019.0710
Wilson Cañon-Montañez
Faculty of Nursing
University of Antioquia
Medellín, Colombia
E-mail: wilson.canon@udea.edu.co
Mónica López de Ávila
Faculty of Nursing
University of Antioquia
Medellín, Colombia
Alba Luz Rodríguez-Acelas,
Faculty of Nursing
University of Antioquia
Medellín, Colombia


{kind=link}
{kind=link}