










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkJornal Português de Gastrenterologia
versão impressa ISSN 0872-8178
J Port Gastrenterol. vol.20 no.4 Lisboa jul. 2013
https://doi.org/10.1016/j.jpg.2012.10.001
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Gastroesophageal variceal bleeding secondary to neuroendocrine pancreatic tumor
Hemorragia por varizes esófago-gástricas secundária a tumor neuroendócrino pancreático
Liliana Eliseua,∗, Catarina Ruivob, José Manuel Romãozinhoc
aServiço de Gastrenterologia, Centro Hospitalar do Barlavento Algarvio, Portimão, Portugal
bServiço de Imagiologia, Centro Hospitalar Universitário de Coimbra, Coimbra, Portugal
cServiço de Gastrenterologia, Centro Hospitalar Universitário de Coimbra, Faculdade de Medicina, Universidade de Coimbra, Coimbra, Portugal
*Autor para correspondência
Case description
A 53-year-old woman was admitted to the emergency department with melena over the preceding 12 h. The patient reported previous symptoms of bloating and early satiety for about 6 months, but no past history of gastrointestinal or liver diseases was known. The physical examination evidenced a deformity in the abdominal wall, secondary to a large palpable stony mass in the epigastrium, and hepatomegaly. No other signs of liver disease were apparent and the hemodynamic parameters were normal. The initial laboratory study disclosed anemia (hemoglobin 9.5 g/dL), and a slight elevation of alkaline phosphatase (185 U/L) and gamma-glutamyltransferase (40 U/L). An emergent upper gastrointestinal endoscopy was performed, showing an active spurting bleed from a subcardial gastroesophageal varix, successfully controlled with endoscopic band ligation.
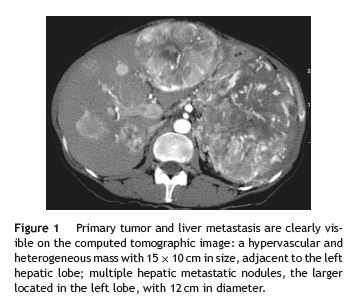
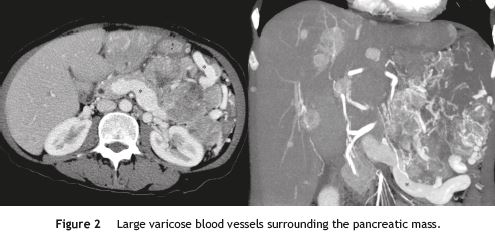
In order to clarify the nature of the abdominal mass and the etiology of the portal hypertension, the patient underwent an abdominal computed tomography (CT) scan, which revealed a large hypervascular pancreatic tumor (Fig. 1), contiguous to the left hepatic lobe, stomach and spleen, as well as multiple hepatic nodules with similar characteristics. It also showed splenic vein thrombosis and exuberant collateral blood vessels around the tumor (Fig. 2). The radiological findings were suggestive of a pancreatic neuroendocrine tumor with liver metastasis, a diagnosis subsequently confirmed by the histological and immunohistochemical studies. The investigation was completed with a chromogranin A analysis (26 nmol/L; reference upper limit 6 nmol/L) and a somatostatin-receptor scintigraphy (OctreoscanTM), which showed no additional secondary locations of the tumor.
The patients clinical course during her hospital stay was favorable, without new bleeding episodes. She was referred to the oncology department for further treatment. Neuroendocrine tumors of the pancreas represent only 1% of the new cases of pancreatic neoplasms.1 Like in the present case, these tumors are usually diagnosed at na advanced stage, with liver metastasis and at least 40% are non-functioning.1,2
The main cause of gastroesophageal varices is portal hypertension secondary to liver cirrhosis. Regional portal hypertension develops from the blockage of a branch of the portal vein. Its major causes are pancreatic tumors and chronic pancreatitis. Isolated gastric varices with no liver cirrhosis is the most typical feature, although cases of concomitant gastric and esophageal varices have been reported.3
Gastroesophageal variceal bleeding due to regional portal hypertension is a rare clinical presentation of pancreatic tumors.3,4 In our patient, the diagnosis of a neoplastic disease was suspected by the presence of an exuberante abdominal mass, which is not always the case. Another particular feature of this case was the existence of both gastric and esophageal varices.
References
1. The National Comprehensive Cancer Network. Neuroendocrine tumors. NCCN Clinical Guidelines in Oncology version1.2011;2011. [ Links ]
2. Massimo F, Plöckinger U, Kwekkeboom DJ, Manfredi R, Körner M, Kvols L, et al. Well-differentiated pancreatic nonfunctioning tumors/carcinoma. Neuroendocrinology. 2006;84:196-211. [ Links ]
3. Wang H, Bie P, Zhang L. Refractory gastroesophageal varicela bleeding secondary to neuroendocrine carcinoma in the pancreatic tail. Pancreatology. 2011;11:228-32. [ Links ]
4. Daveson J, Masson J, Cameron D, Jennings M. A case of an isolated gastric variceal bleed secondary to a pancreatic neuroendocrine tumor. European Journal of Gastroenterology and Hepatology. 2007;19:1144-8. [ Links ]
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consent. The authors must have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence must be in possession of this document.
Conflicts of interest
The authors have no conflicts of interest to declare.
*Corresponding author
E-mail address: eliseu.liliana@gmail.com (L. Eliseu).
Received 3 July 2012; accepted 5 October 2012

{kind=link}