










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkJornal Português de Gastrenterologia
versão impressa ISSN 0872-8178
J Port Gastrenterol. v.17 n.3 Lisboa maio 2010
Successful Conservative Management of Emphysematous Phlegmonous Gastritis: A Case Report
Carlos Noronha Ferreira, Luís Correia, Elídio Barjas, Fátima Serejo, Miguel Carneiro de Moura
Serviço de Gastrenterologia e Hepatologia, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte
Abstract
BACKGROUND: Acute phlegmonous gastritis is a suppurative bacterial infection of the stomach first described by Curveilhier in 1820. The two variants which have been described are the emphysematous and the necrotizing variant. CASE REPORT: A 30 year old male presented with vomiting and diarrhea over 24 hours. Laboratory tests revealed leukocytosis, neutrophilia and raised C reactive Protein (CRP) levels. The abdominal CT scan showed a diffusely thickened stomach wall with intramural gas as well as in the peripheral intra-hepatic vessels. There was complete resolution of the emphysematous gastritis changes on empirical broad spectrum antibiotic therapy for 10 days with resolution of the emphysematous gastritis changes; oral diet was started. An exhaustive investigation for a possible etiological factor of emphysematous gastritis was inconclusive. The patient was discharged on the 11th day. An abdominal CT scan and upper GI endoscopy repeated after discharge were normal. CONCLUSIONS: This report describes the successful management of a patient with the emphysematous variant of phlegmonous gastritis with broad spectrum antibiotic treatment. We review the pathogenesis, clinical manifestations and management of this rare, often fatal pathology.
Keywords: phlegmonous gastritis, emphysematous gastritis.
Abordagem conservadora de um caso de gastrite fleimonosa enfisematosa
Resumo
A gastrite fleimonosa aguda é uma infecção bacteriana supurativa do estômago descrita pela primeira vez por Curveilhier em 1820. As duas variantes descritas são a variante enfisematosa e a necrotizante. CASO CLÍNICO: Trata-se de um doente de 30 anos que se apresentou com queixas de vómitos e diarreia com 24 horas de evolução. Os exames laboratoriais revelaram leucocitose, neutrofilia e aumento de proteina C reactiva (PCR). A TC abdominal confirmou achados ecográficos de espessamento difuso da parede gástrica com gás intramural e nos vasos intrahepáticos. A endoscopia digestiva alta de urgência revelou eritema geográfico da mucosa do antro e corpo com pregas espessadas, erosões superficiais e focos de necrose. Foi instituida antibioterapia empírica de largo espectro durante 10 dias com resolução das alterações enfisematosas gástricas tendo o doente tolerado dieta oral. Uma avaliação exaustiva para possíveis factores etiológicos de gastrite enfisematosa foi inconclusiva. O doente teve alta ao 11º dia de internamento. A TC abdominal e endoscopia digestiva alta após alta foram normais. CONCLUSÕES: Este caso descreve o manejo com êxito de um doente com a variante enfisematosa de gastrite fleimonosa com antibioterapia de largo espectro. Fazemos uma revisão sobre a patogénese, manifestações clínicas e manejo desta patologia rara que é frequentemente fatal.
Palavras-chave: Gastrite fleimonosa, gastrite enfisematosa.
INTRODUCTION
Acute phlegmonous gastritis is a suppurative bacterial infection of the stomach which was first described by Curveilhier in 18201. Several risk factors have been identified and these include local mucosal injury, achlorhydria, alcoholism and immunocompromised states1-3. In nearly 40% patients, no predisposing factors are identified1. There are two variants of phlegmonous gastritis: emphysematous gastritis which is due to submucosal invasion by gas producing organisms, and necrotizing or gangrenous gastritis which is characterized by extensive thrombosis of the submucosal vessels1-2.
CASE REPORT
A 30-year-old caucasian male was admitted to hospital in December 2005, with vomiting and diarrhea over 24 hours. He referred three episodes of post prandial vomiting and eight motions of yellow liquid stools without mucus or blood. He felt unwell and complained of chills with rigors. There was no documented fever or abdominal pain. Past medical history was insignificant except for a bout of diarrhea six months before, which remitted with a probiotic. He was a non smoker and did not consume alcohol.
The patient had a good general condition, was afebrile and hemodynamically stable. The abdomen was soft on palpation, without organomegaly or palpable masses. The bowel sounds were normal. No other significant abnormality was detected on physical examination. Laboratory tests revealed normal hemoglobin level (Hb 15g/dL), leukocytosis 14.000/μL (N: 4-11.000/μL) (neutrophils: 82%, lymphocytes 10% monocytes 8%), low serum potassium 3.2mEq/L (N: 3.5-5mEq/L) and raised CRP 5.2mg/dL (N: < 0.5mg/dL). Serum AST, ALT, total bilirubin, alkaline phosphatase, lactate dehydrogenase and amylase were normal. Abdominal X ray was normal. An abdominal ultrasonography (USG) and CT scan showed diffuse thickening of the stomach wall with an irregular mucosal pattern and intramural air. There was evidence of air in the peripheral intrahepatic vessels. No air was noted in the extrahepatic portal or splenic vessels or in the peritoneum (Fig. 1). These findings were highly suggestive of emphysematous gastritis. The surgery consultancy ruled out urgent laparotomy in view of the good clinical condition and the absence of sepsis. Upper gastrointestinal endoscopy revealed thickened, edematous and soft mucosal folds with multiple superficial erosions and necrosis (Fig. 2). The gastric antral mucosa had an intense geographic pattern of erythema (Fig. 3). Gastric mucosal biopsies performed revealed mucosal infiltration by neutrophils, extensive hemorrhage in the lamina propria with atrophy and loss of the mucosal crypts and glands due to mucosal ischemia. Helicobacter pylori (Hp) was not detected.
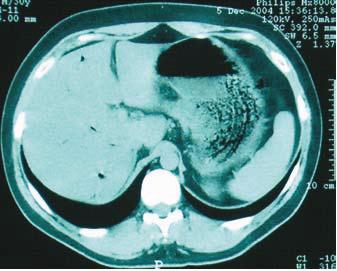
Fig. 1. Abdominal CT scan showing thickened stomach wall with intra-mural air and air in the peripheral intra-hepatic veins.
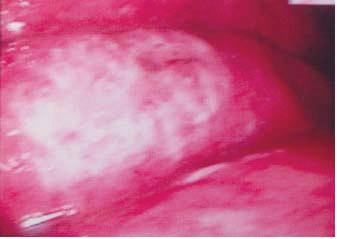
Fig. 2. Thickened gastric folds with hyperemia, superificial erosions and necrosis seen in upper gastrointestinal endoscopy.

Fig. 3. Upper gastrointestinal endoscopy showing intense hyperemia with geographic pattern of the antral mucosa.
Empirical broad spectrum antibiotic therapy with piperacilin/tazobactam and vancomicin was started. Investigations done to rule out a possible predisposing or etiologic condition, including blood bacterial cultures and serum markers for human immunodeficiency virus (HIV) 1 and 2 were negative. The patient had an uneventful recovery and was discharged after 10 days of intravenous antibiotics.
An abdominal CT scan 3 weeks after discharge was normal (Fig. 4). Upper GI endoscopy 12 weeks after discharge, revealed a few gastric antral erosions. Mucosal biopsies revealed non active and non atrophic chronic gastritis without Hp. The patient remains asymptomatic to date.

Fig. 4. Normal follow-up abdominal CT scan 3 weeks after discharge.
DISCUSSION
Phlegmonous gastritis occurs due to local or hematogenous bacterial infection of the gastric wall. It may be localized, often involving the gastric antrum, or diffuse involving the entire stomach1,3-6. Extension into the other segments of the gastrointestinal tract is rare and may be more common with the necrotizing variant1,2,6.
The exact pathogenetic mechanism of phlegmonous gastritis is unknown1,4,5. Risk factors can be identified in nearly 60% of patient and they include local mucosal injury, achlorhydria, alcoholism, malignancy, connective tissue disorders, infection and immunocompromised states1-6. The alpha-hemolytic Streptococcus is the most frequent causative organism and is isolated from the blood or gastric wall in 75% of the cases of phlegmonous gastritis1-4. Other etiologic organisms in decreasing order of frequency are Staphylococcus spp, Escherichia coli, Haemophilus influenzae, Proteus and Clostridia1,3-5. Mixed bacterial infections are documented in 30% cases1-4. Emphysematous gastritis is caused by Clostridium welchii and other gas-forming aerobic colonic bacilli which include Escherichia coli, Streptococcus, Bacillus subtilis and Bacillus proteus1,2,7. In our patient, the blood cultures were negative.
Histologically, it is characterized by gastric submucosal infiltration by neutrophils and plasma cells with intramural hemorrhage, necrosis and thrombosis of submucosal blood vessels1,2,4-6.
Patients typically present with abdominal pain, nausea, vomiting, fever, chills and hematemeses1,3-5. Deninger´s sign is characterized by localized abdominal pain in the epigastric region which is relieved by sitting up1-3,6. Our patient presented with diarrhea and chills without fever or abdominal pain.
There are no specific laboratory findings diagnostic of phlegmonous gastritis though presence of leukocytosis and normal serum / urinary amylase in the clinical context supports the diagnosis2,6. Plain abdominal X-rays are abnormal in 50% cases and findings include paralytic ileus, edematous gastric folds, elevation of the left hemi diaphragm and free gas under the diaphragm2,6. In our patient, the abdominal X-ray was normal. Abdominal USG detects thickening of the gastric wall. Abdominal CT scan demonstrates thickened hypodense gastric wall with intramural gas, and gas in vessels draining the stomach1. In our patient, the thickening of the gastric wall and intramural gas were very suggestive of emphysematous gastritis. Endoscopic examination of the upper gastrointestinal tract reveals thickened edematous, reddened mucosal folds with fibrinopurulent exudates1,5,8. Due to submucosal involvement, snare biopsy specimens are preferred to standard forceps2,4,5. Culture of the exudates may identify the causative organism1,4,6. This was not performed in our patient. Endoscopic ultrasound (EUS) is superior to CT scan for assessment of gastric wall thickening and the extent of inflammation1,4,6,8. Although phlegmonous gastritis primarily involves the submucosa, it may extend to involve all the gastric wall layers5,8,9. EUS detects diffuse thickening of the gastric wall with a hypoechoic submucosal layer in phlegmonous gastritis and a linear band of air in the submucosal layer in emphysematous gastritis7. The two radiological patterns of gastric intramural air include; linear lucency pattern associated with gastric emphysema, and the cystic mottled pattern is usually associated with the more serious emphysematous gastritis7.
The decision for conservative management depends on the clinical condition and the findings on imaging. Phlegmonous gastritis is a very rare pathology. Due to delay in diagnosis and rapid progression to peritonitis, it is associated with high mortality2,6,8. In patients managed conservatively with medical treatment, the mortality varies between 10 to 17% in those with localized phlegmonous gastritis; and is around 60% for those with diffuse disease and the emphysematous type of phlegmonous gastritis1. There is no correlation of mortality risk with the age, gender and clinical presentation1. Conservative medical treatment can be considered in early and localized disease2,6,8. Broad spectrum antibiotic therapy is recommended as 30% of the patients have polymicrobial infection1,2,5,6. Surgical resection of the stomach may be required. The combination of medical and surgical treatment is associated with better survival (50%) than medical treatment alone (20%)1,5.
In conclusion, this patient presented with the rare and potentially fatal emphysematous variant of phlegmonous gastritis. No predisposing agent was identified. He was successfully managed conservatively with broad spectrum antibiotics with an excellent outcome.
REFERÊNCIAS
1. Kim GY, Ward John, Henessey B, et al. Phlegmonous gastritis: case report and review. Gastrointest Endosc 2005;61:168-174. [ Links ]
2. Stein LB, Greenberg RE, Ilardi CF, et al. Acute necrotizing gastritis in a patient with peptic ulcer disease. Am J of Gastroenterol 1989;84:1552-1554.
3. Schultz MJ, van der Hulst RWM, Tytgat GNJ. Acute phlegmonous gastritis. Gastroint Endosc 1996;44:80-83.
4. Hu DC, McGrath KM, Jowell PS, et al. Phlegmonous gastritis: successful treatment with antibiotics and resolution documented by EUS. Gastrointest Endosc 2000;52:793-795.
5. Aviles JF, Fernandez-Seara J, Barcena R, et al. Localized phlegmonous gastritis: Endoscopic view. Endoscopy 1988;20:38-39.
6. Hsu CY, Liu JS, Chen DF, et al. Acute diffuse phlegmonous esophago-gastritis: Report of a survived case. Hepatogastroenterology 1996;43:1347-1352.
7. Soon MS, Yen HH, Soon A, et al. Endoscopic ultrasonographic appearance of gastric emphysema. World J of Gastroenterol 2005;11:1719-1721.
8. Yuji I, Kabemura T, Daisuke Y, et al. A case of acute phlegmonous gastritis successfuly treated with antibiotics. J Clin Gastroenterol 1999;28:175-177.
9. Wakayama T, Watanabe H, Ishizaki Y, et al. A case of phlegmonous esophagitis associated with diffuse phlegmonous gastritis. Am J Gastroenterol 1994;89:804-806.
Correspondência: Carlos Noronha Ferreira; E-mail: carlosnferreira@hotmail.com.
Recebido para publicação: 01/12/2008 e Aceite para publicação: 20/04/2009.
