










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkMedicina Interna
Print version ISSN 0872-671X
Medicina Interna vol.27 no.2 Lisboa Apr. 2020
https://doi.org/10.24950/O/291/19/2/2020
ARTIGOS ORIGINAIS / ORIGINAL ARTICLES
São os Outcomes da Ventilação Não Invasiva na Falência Respiratória Aguda Similares nos Adultos Muito Idosos?
Are Outcomes of Non-Invasive Ventilation in Acute Respiratory Failure Similar in Very Old Adults?
Ana Rita Costa  https://orcid.org/0000-0002-1939-1043
https://orcid.org/0000-0002-1939-1043
Inês Frutado https://orcid.org/0000-0003-3985-0718
João Gonçalves https://orcid.org/0000-0002-8282-2547
Mariana Meireles https://orcid.org/0000-0002-5744-6738
João Neves https://orcid.org/0000-0003-0967-8443
Andrea Mateus https://orcid.org/0000-0002-6734-599X
Departamento de Medicina Interna, Centro Hospitalar e Universitário do Porto, Porto, Portugal.
Abstract:
Introduction: Acute respiratory failure (ARF) is one of the most prevalent causes of observation in the emergency department in an ageing population. Non-invasive positive pressure ventilation (NIPPV) has shown good results in critically ill with ARF. The evidence of NIPPV outcomes in old patients is scarce. The aim of our study is to analyse outcomes of NIPPV use in this population.
Methods: We conducted a prospective observational study in a 12-bed intermediate care unit of an university hospital. We included and consecutively compared patients aged 75 years old or more (study group) and under 65 years old (control group) submitted to NIPPV due to ARF. The primary end point was mortality (in-hospital and 30 daysafter discharge). Secondary endpoints were NIPPV settings, complications, and failure rate.
Results: A total of 109 patients were included. In-hospital mortality was significantly higher in the study group (22.2 % vs 8.1%, p< 0.01). However, mortality 30 days after discharge was not significantly different (4.1% vs 4.9%, p = 0.37). NIPPV duration of use (6.1 vs 2.2 days, p < 0.01) and hospital length of stay (14.3 vs 6.2 days, p = 0.01) were higher in the study group. NIPPV failure (22.2% vs 16.1 %, p = 0.09) and complication rate (intolerance 8% vs 6%, p = 0.31; ulcers 4% vs 3%, p = 0.28) were similar in both groups.
Conclusion: ARF carries a grim prognosis in older adults. A high mortality rate was observed in older patients despite similar severity assessments and NIPPV failure and complication rates. Notably, out of the hospital mortality is comparable between both groups.
Keywords: Aged; Aged, 80 and over; Noninvasive Ventilation; Respiratory Insufficiency; Treatment Failure.
Resumo:
Introdução: Na população envelhecida, a falência respiratória aguda (FRA) é das causas mais prevalentes de observação no serviço de urgência. A ventilação não invasiva por pressão positiva (VNiPP) mostrou bons resultados nos doentes críticos com FRA. Mas a evidência em doentes muito idosos é escassa. O objetivo do estudo é analisar os outcomes do uso de VNiPP nesta população.
Métodos: Conduzimos um estudo prospetivo observacional numa unidade de cuidados intermédios de um hospital universitário. Foram incluídos e posteriormente comparados os doentes com idade igual ou superior a 75 anos (grupo de estudo) e inferior a 65anos(grupo controlo) submetidos a VNiPP por FRA. O endpoint primário foi a mortalidade (hospitalar e 30 dias após a alta). Os endpoints secundários foram parâmetros, complicações e taxa de falência de VNPP.
Resultados: Foram incluídos um total de 109 doentes. A Mortalidade hospitalar foi significativamente maior no grupo deestudo (22,2 % vs 8,1%, p <0,01). Contudo, a mortalidade aos 30 dias após alta não foi significativamente diferente (4,1% vs 4,9%, p = 0,37). A duração de uso de VNiPP (6,1 vs2,2 dias, p < 0,01) e de internamento (14,3 vs6,2 dias, p = 0,01) foram maiores no grupo de estudo. A falência de VNiPP (22,2% vs 16,1 %, p = 0,09) e taxa de complicações (intolerância 8% vs 6%, p = 0,31; úlceras 4% vs 3%, p = 0,28) foram similares entre os grupos.
Conclusão: A FRA tem mau prognóstico nos adultos idosos. A maior taxa de mortalidade foi observada nestes doentes, apesar de similar gravidade e similares taxas de falência e complicação de VNiPP. Notavelmente, a mortalidade fora do hospital foi comparável entre os grupos.
Palavras-chave: Falha de Tratamento; Iddoso com 80 anos ou mais; Insuficiência Respiratória; Ventilação Não Invasiva.
Introdution
World population is ageing, and this phenomenon is expected to continue over time. Health professionals are increasingly facing a growing number of very old patients with chronic multimorbidity andhigher complexity.1,2 In the very old, dyspnea and acute respiratory failure (ARF) are common and are major causes of observation in the emergency department (ED) and hospital admission.3,4 They are key symptoms of the most prevalent cardiopulmonary diseases: cardiogenic pulmonary oedema (CEP), exacerbation of chronic obstructive pulmonary disease (COPD) and community-acquired pneumonia (CAP).3 Furthermore, the pathophysiological changes that occur with senescence affect both pulmonary and cardiac function and need to be taken into consideration.4
Non-invasive positive-pressure ventilation (NIPPV) use is expanding, particularly in acute settings.5-7 NIPPV has the same physiological effects of invasive mechanical ventilation (IMV) with the advantage of possibly avoiding the major, and sometimes life-threatening, risks and complications associated with the latter.5-7 It has been used for many years in a wide spectrum of diseases, including the most prevalent diseases causing ARF in the very old, with good results in terms of efficacy, survival, reduction of complications and need for intubation.5,6,8 Consequently, NIPPV became part of first line interventions in some causes of ARF.9,10
The complex and still poorly understood very old population is underrepresented in the majority of clinical trials of NIPPVuse in ARF. Therefore, evidenceis still scarce, particularly regarding long term outcomes, impact on quality of life and treatment adherence, and limited to few studies.11-13 NIPPV use can be challenging, particularly regarding timing for its initiation, patient allocation, technical settings and ethical issues. Candidates should be carefully evaluated and monitored.14 Very old patients only reinforce this challenge. With this study we aim to understand if patients presenting with ARF have the same outcomes depending if they are 75 years old or more or under 65 years old.
Patients and methods
OVERVIEW
A prospective observational study of a cohort of patients admitted to a 12-bed intermediate care unit of an university hospital was conducted. All patients with 75 years or older and under 65 years old submitted to NIPPV due to ARF admitted in this unit between September 2014 and December 2016 were included after study enrolment written consent was obtained. Patients in a weaning protocol of IMV were excluded. Patients that started NIPPV prior to intermediate care unit admission and later admitted were also included. A total of 109 patients were enrolled at our study. NIPPV was managed by the unit’s health staff. Study investigators had no influence on patient management.
DATA COLLECTION
Data was collected from patient’s clinical records. Demographic data, vital signs, blood tests, Acute Physiology and Chronic Health Evaluation (APACHE) II score and comorbidities were collected. Regarding NIPPV use, data on parameters, duration and failure of this technique (defined as death by all causes or need of invasive ventilation) were registered. Also, ARF aetiology was noted. Mortality data (in-hospital and 30 days after discharge) were also recorded.
STUDY ENDPOINTS
Patients were divided into two groups: study group (75 yo or more) and control group (under 65 yo). The 10 years gap aimed to reinforce age difference between groups. Primary endpoints were in-hospital mortality and mortality 30 days after discharge. Secondary endpoints were NIPPV settings, complications and failure. We also compared the two groups in terms of aetiology of ARF and subsequent NIPPV use at home after discharge.
STATISTICAL ANALYSIS
In the general parameters at the admission, analytic changes, ARF aetiology, NIPPV failure, NPPV complications, death, progression to VMI, do not intubate (DNI) order and readmission there was mainly used the absolute number (n) and the corresponding percentage. In the APACHE II score, vital signs, arterial blood pH, partial pressure of arterial carbon monoxide (PaCO2), partial pressure of arterial oxygen and percentage of inspired oxygen (PaO2/FiO2) ratio, EPAP and IPAP there was used the median.
Statistical Analysis was completed with SPSS 26.0, IBM®. The tests used were Kolmogorov-Smirnov, one sample T-test, binominal test, chi-square test and Wilcoxon-Mann-Whitney test. There were used quantitative measure scales for numeric variables and qualitative scalesin the other ones, to permit inter-group comparation. The absolute and percentual values were recorded. The mean, median and confidence interval (95%) were calculated. Statistical significance was considered for p < 0.05.
ETHICAL CONSIDERATIONS
Study protocol was approved by Local Ethics Committee. At admission, participants were informed by the investigators about study aim and protocol. Written consent was obtained for enrolled patients.
Results
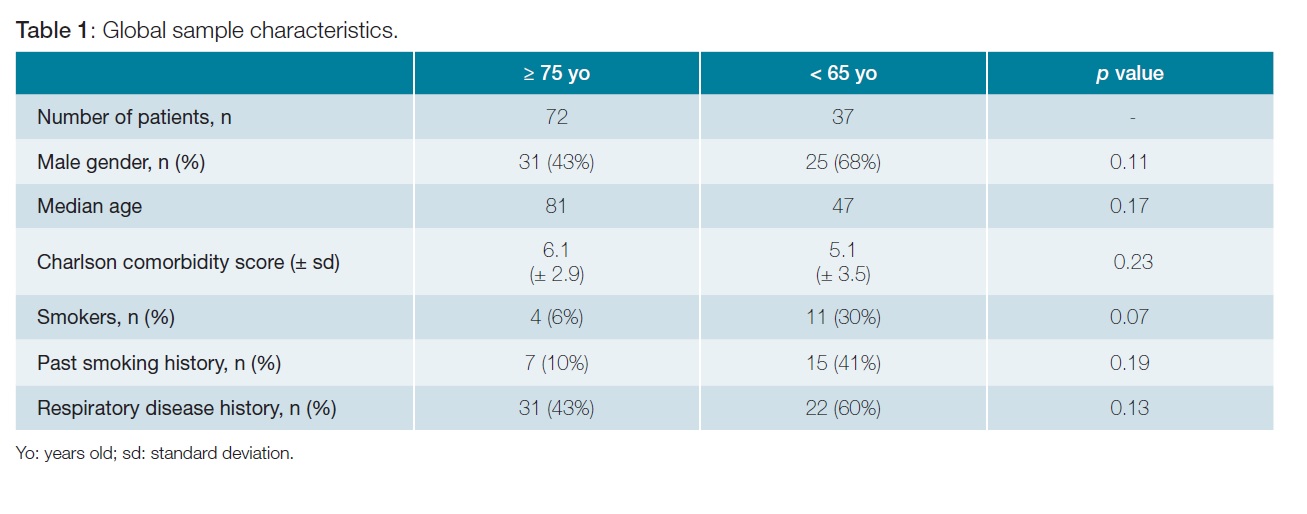
A total of 109 patients were enrolled in the study: 72 patients aged 75 or more years old (study group) and 37 under 65 years old (control group). The two groups were globally comparable. Control grouphad a male predominance without statistical significance. Comorbidity was common in both groups (Charlson comorbidity index 6.1 ± 2.9 and 5.1 ± 3.5, respectively). Smoking history (past or present) was superior in the control group, although without statistical significance. Particularly, respiratory disease history was similar in the two groups (43% instudy group and 60% inthe control group) (Table 1).
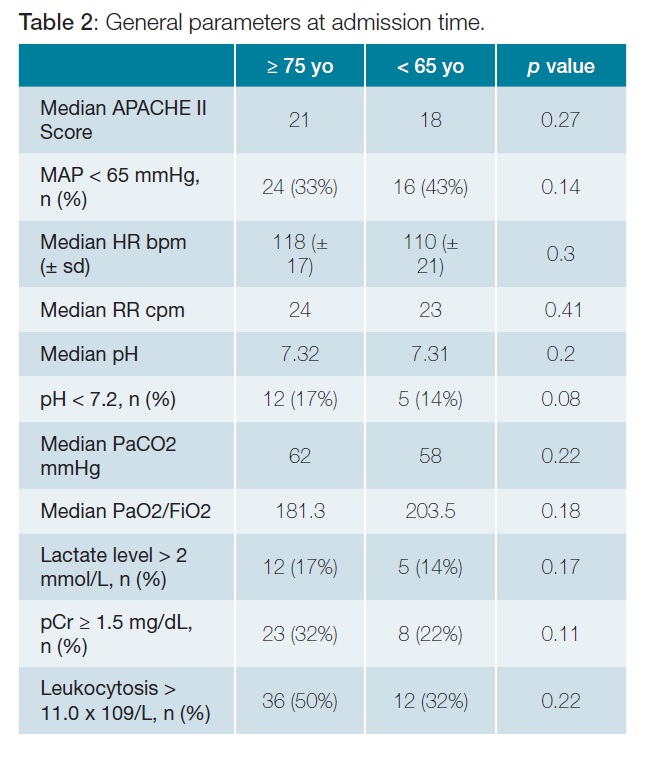
At admission groups were comparable in terms of severity of the disease (Table 2).
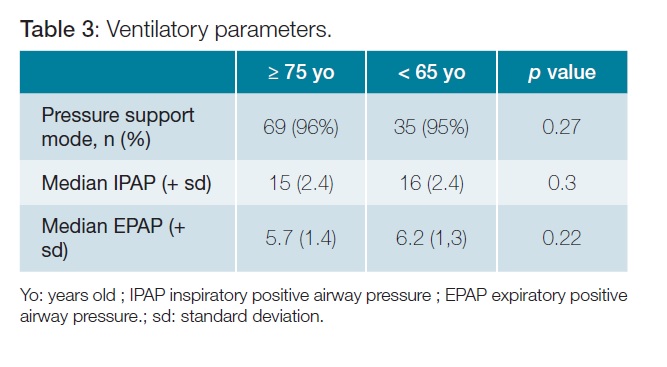
The preferred mode of NIVPP was pressure support ventilation (PSV), with similar average IPAP/EPAP (Table 3).
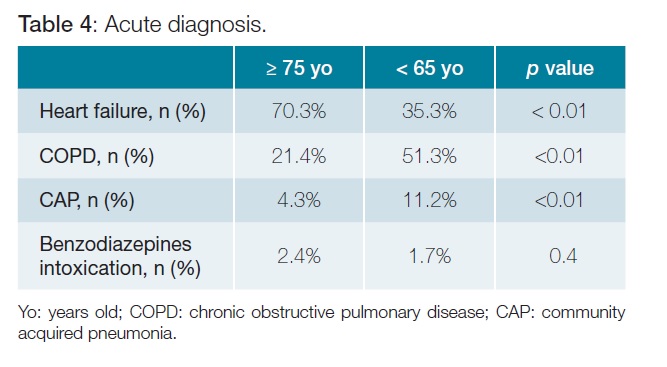
Heart failure (HF) as ARF aetiology was more prevalent in the study group (70.3% vs 35.3%, p < 0.01). Chronic obstructive pulmonary disease (COPD) exacerbation and CAP were more common in control group, although the latter was present only in a minority of patients (Table 4).
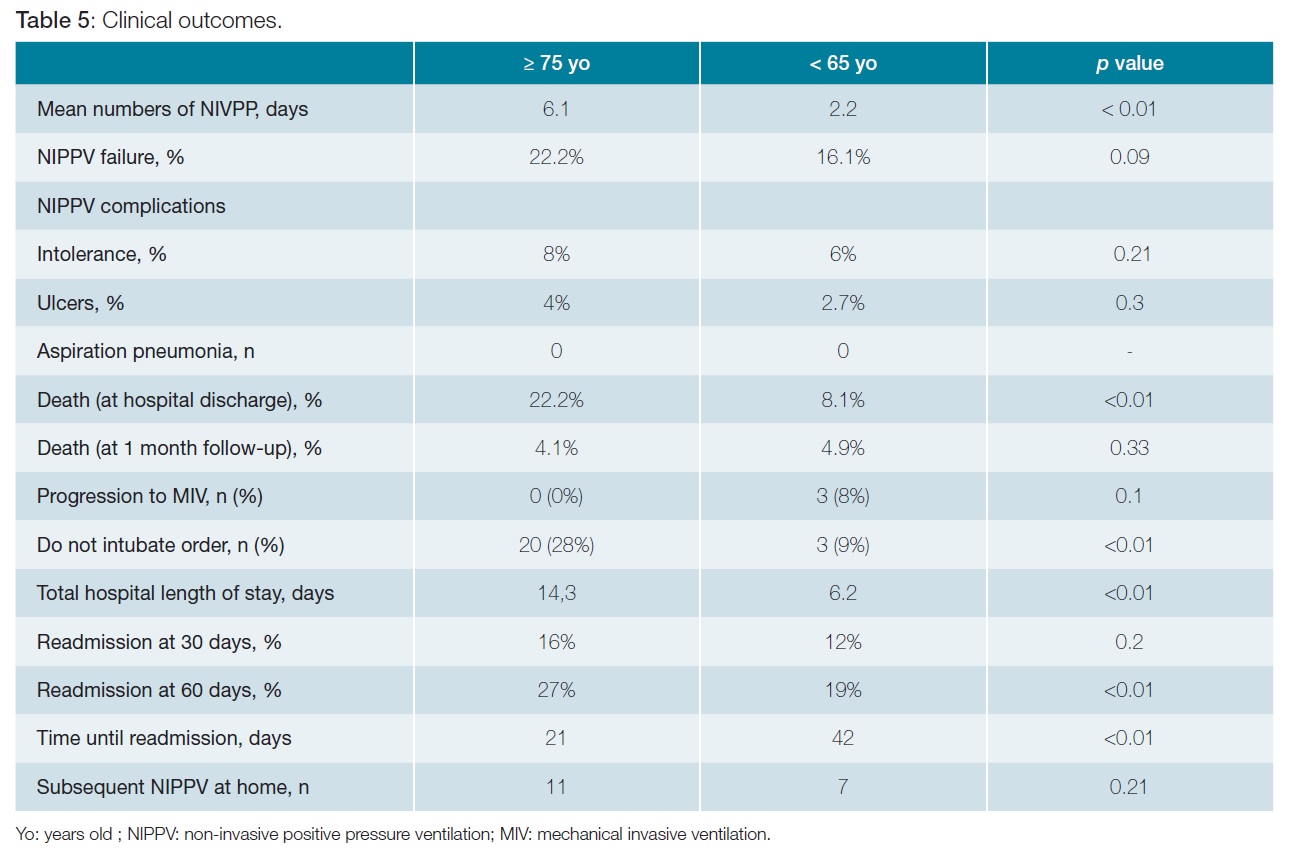
NIVPP duration and hospitalization were both longer in the study group (6.1 vs 2.2 days; p < 0.01) and 14.3 vs 6.2 days(p < 0.01), respectively. NIPPV failure was similar (22.2% vs 16.1% p = 0.09). A significatively higher proportion of patients in the study group had a do not intubate order (DNI) (28% vs 9%, p < 0.01). Hospital mortality rate was greater in the study group(22.2% vs8.1%, p< 0.01). No difference was found between the groups in terms of readmission at 60 days (27% vs 19%, p < 0.001) and time until readmission (21 days vs 42 days, p < 0.01). Survival at one-month post hospital discharge was not statistically different (4.1% and 4.9%, respectively p > 0.2) (Table 5).
Discussion
The number of very old patients enrolled in the study clearly surpasses the number of under 65 years old patients.
We believe this to be a clear reflection of our hospital daily clinical practice and not a selection bias. Actually, previous work at our institution focused in emergency room NIPPV practice already highlighted this point.15
Surprisingly, our control group had a Charlson Comorbidity score similarto thevery old patients. Disease burden in this younger population is higher than previously reported and should challengecommon beliefs that very old patients are necessarily sicker.16 Also, as we previously reported, Charlson Comorbidity Index is a poor discriminator of NIPPV outcomes.17
Although not statistically significant, current tobacco use was more prevalent in the control group and may explain the higher proportion of COPD exacerbation as cause of ARF in this group. Moreover, we may have a survival bias as COPD patients with history of ARF and NIPPV may have died at younger ages.
Regarding ARF severity assessment, we found no difference between the two groups despite the comprehensive data collected. Particularly, looking at median APACHE II score, the 3 points difference could be attributed to age exclusively (patients with or over 75 years old score 6 points and those under 65 score 3 points) (Table 5). Our study population can be underpowered to find such differences, although statistical difference was found for other data, namely for primary endpoints.
Age did not determine NIPPV mode or parameters selection, as shownby the absence of differences between both groups. This reflects an age unbiased practice in our intermediate care unit. NIPPV complications rates were similar between groups and fairly residual.
NIPPV duration was longer in very old patients, in spite of most of them (70.3%) having heart failure as ARF aetiology. We did not expect the control group to have shorter NIPPV duration. Usually, comparably to COPD exacerbations, acute pulmonary oedema is associated with shorter ventilation time. Moreover, ARF severity, as previously discussed, cannot explain these differences. Age is related to diminished functional reserve of several organs and system, particularly on respiratory function. Time to recovery may be longer in these very old patients.18 We hypothesize that terminal heart failure in our very old patients may partially explain not only longer NIPPV times, but also the higher hospital mortality in this group. Unfortunately, data about left ventricular function was not collected to support this hypothesis. Although the rational to set a DNI order was not evaluated, the greater number of DNI patients in the study group is certainly a consequence of the identification of poorer functional status or advanced organic disease. We should also reflect whether prolonged NIPPV use in the group with higher mortality could be a surrogate to lack of recognition of irreversible conditions. Patient selection is of paramount importance, both at initiation and prolongation of NIPPV. The mortality of patients with ARF is high, particularly in old people. Studies in older patients with ARF have reported hospital mortality rates between 16%- 40%.3,12 This is in concordance with our study, that found a mortality rate at hospital discharge of 22.2% in patients aged 75 yo or more. This was significantly higher than in patients aged less than 65 yo (8.1%, p < 0.01), despite comparable characteristics, similar severity of the disease at the admission, NIPPV settings, complications and failure. In opposition to Schortgen et al12 in our study the mortality at 30 days after discharge was only 4.1% and not significantly different from the control group (4.1 % vs 4.9%, p = 0.33). Very old patient 30-day survival after discharge may result of survivor bias of the functionally less compromised patients. The percentage of patients readmitted at 60 days (27% vs 19%, p < 0.01) and time until readmission (21 days vs 42 days, p < 0.01) was also not significantly different between the two groups. This may add a potential benefit for this subset of very old patients who survive to hospital discharge, by being able to avoid or delay further hospital admissions. Recognition of this subset of very old patients is of uttermost importance for selection of the best candidates to NIPPV.
Conclusion
ARF is a common cause of intermediate care unit ad- mission and NIPPV use in very old patients. Under the same NIPPV practice, same level of comorbidity and ARF severity, this seems a safe therapy in very old patients. Our results sug- gestthat thereis a subset of this very old patients that will benefit the most from NIPPV in ARF. Large RCTs are needed to further establish and broadcast the efficacy and safety of NIPPV in older people presenting with ARF and to identify this subset of patients.
Acknowledgments
The authors thank the medical team of the Intermediate
Care Unit of Centro Hospitalar Universitário do Porto.
All the authors of this paper have no possible conflicts of interest to disclose and no other financial relationships that may influence the writing of the manuscript.
All authors have been implicated in the process until the final version of the manuscript. ARC, JG, IF and MM were involved in data collection. ARC, IF and JN were responsible for the draft of the article and gave critical revision of the manuscript for important intellectual content. All the authors revised the manuscript for final version approval.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
1. Rechel B, Grundy E, Robine JM, Cylus J, Mackenbach JP, Knai C, et al. Ageing in the European Union. Lancet. 2013;381:1312-22. [ Links ]
2. Ferrucci L, Giallauria F, Guralnik JM. Epidemiology of aging. Radiologic clinics of North America. 2008;46:643-52, v. [ Links ]
3. Ray P, Birolleau S, Lefort Y, Becquemin MH, Beigelman C, Isnard R, et al. Acute respiratory failure in the elderly: etiology, emergency diagnosis and prognosis. Critical Care. 2006;10:R82. [ Links ]
4. Delerme S, Ray P. Acute respiratory failure in the elderly: diagnosis and prognosis. Age and ageing. 2008;37:251-7. [ Links ]
5. Nava S, Hill N. Non-invasive ventilation in acute respiratory failure. Lancet. 2009;374:250-9. [ Links ]
6. Scala R, Pisani L. Non invasive ventilation in acute respiratory failure: which recipe for success? Eur Respir Rev. 2018;27:180029. doi: 10.1183/16000617.0029-2018. [ Links ]
7. Mas A, Masip J. Noninvasive ventilation in acute respiratory failure. Curr Heart Fail Rep. 2019;16:89-97. doi: 10.1007/s11897-019-00429-y. [ Links ]
8. Liu YJ, Zhao J, Tang H. Non-invasive ventilation in acute respiratory failure: a meta-analysis. Clin Med. 2016;16:514-23. [ Links ]
9. Rochwerg B, Brochard L, Elliott MW, Hess D, Hill NS, Nava S, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017;50:1602426. doi: 10.1183/13993003.02426-2016. [ Links ]
10. British Thoracic Society Standards of Care C. Non-invasive ventilation in acute respiratory failure. Thorax. 2002;57:192-211. [ Links ]
11. Nava S, Grassi M, Fanfulla F, Domenighetti G, Carlucci A, Perren A, et al. Non-invasive ventilation in elderly patients with acute hypercapnic respira- tory failure: a randomised controlled trial. Age Ageing. 2011;40:444-50. [ Links ]
12. Schortgen F, Follin A, Piccari L, Roche-Campo F, Carteaux G, Taillandier-Heriche E, et al. Results of noninvasive ventilation in very old patients. Ann Intensive Care . 2012;2:5. doi: 10.1186/2110-5820-2-5. [ Links ]
13. Philippart F, Vesin A, Bruel C, Kpodji A, Durand-Gasselin B, Garcon P, et al. The ETHICA study (part I): elderly´s thoughts about intensive care unit admission for life-sustaining treatments. Intensive Care Med . 2013;39:1565-73. doi: 10.1007/s00134-013-2976-y. [ Links ]
14. Scala R. Challenges on non-invasive ventilation to treat acute respiratory failure in the elderly. BMC Pulm Med. 2016;16:150. doi: 10.1186/s12890-016-0310-5. [ Links ]
15. Vilaça M, Aragão I, Cardoso T, Dias C, Cabral-Campello G. The Role of Noninvasive Ventilation in Patients with "Do Not Intubate" Order in the Emergency Setting. PLoS One. 2016;11:e0149649. doi: 10.1371/journal.pone.0149649. [ Links ]
16. Morland M, Haagensen R, Dahl FA, Berdal JE. Epidemiology and prognoses in a medical intermediate care unit. Tidsskr Nor Laegeforen . 2018;138. doi: 10.4045/tidsskr.17.0496. [ Links ]
17. Meireles M, Machado A, Lopes J, Abreu S, Furtado I, Goncalves J, et al. Age-adjusted Charlson Comorbidity Index Does Not Predict Outcomes in Patients Submitted to Noninvasive Ventilation. Arch Bronconeumol. 2018;54:503-9. [ Links ]
18. van Oostrom SH, Engelfriet PM, Verschuren WM, Schipper M, Wouters IM, Boezen M, et al. Aging-related trajectories of lung function in the general population-The Doetinchem Cohort Study. PloS One. 2018;13:e0197250. doi: 10.1371/journal.pone.0197250. [ Links ]
Responsabilidades Éticas
Conflitos de Interesse: Os autores declaram a inexistência de conflitos de interesse na realização do presente trabalho.
Fontes de Financiamento: Não existiram fontes externas de financiamento para a realização deste artigo.
Confidencialidade dos Dados: Os autores declaram ter seguido os protocolos da sua instituição acerca da publicação dos dados de doentes.
Proteção de Pessoas e Animais: Os autores declaram que os procedimentos seguidos estavam de acordo com os regulamentos estabelecidos pelos responsáveis da Comissão de Investigação Clínica e Ética e de acordo com a Declaração de Helsínquia da Associação Médica Mundial.
Proveniência e Revisão por Pares: Não comissionado; revisão externa por pares.
Ethical Disclosures
Conflicts of interest: The authors have no conflicts of interest to declare.
Financing Support: This work has not received any contribution, grant or scholarship
Confidentiality of Data: The authors declare that they have followed the pro- tocols of their work center on the publication of data from patients.
Protection of Human and Animal Subjects: The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Provenance and Peer Review: Not commissioned; externally peer reviewed.
© Autor (es) (ou seu (s) empregador (es)) 2019. Reutilização permitida de acordo com CC BY-NC. Nenhuma reutilização comercial.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use.
Correspondence / Correspondência:
Ana Rita Costa – arcosta89@gmail.com
Largo Prof. Abel Salazar - 4099-001 PORTO
Received / Recebido: 15/01/2020
Accepted / Aceite: 28/04/2020
Publicado / Published: 27 de Junho de 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}