










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkMedicina Interna
Print version ISSN 0872-671X
Medicina Interna vol.27 no.1 Lisboa Mar. 2020
https://doi.org/10.24950/SC/361/18/1/2020
SÉRIES DE CASOS
Actinomyces and Lung: A Rare Association
Actinomyces e Pulmão: Uma Associação Rara
Bruno Cabrita1  https://orcid.org/0000-0002-7832-051X
https://orcid.org/0000-0002-7832-051X
Ana Paula Vaz1 https://orcid.org/0000-0001-9732-4754
R. Correia de Abreu2 https://orcid.org/0000-0002-0080-7571
Sofia Jordão2 https://orcid.org/0000-0002-9369-1968
Sílvia Correia1 https://orcid.org/0000-0002-2076-7925
Jorge Ferreira1 https://orcid.org/0000-0002-5003-6496
1Serviço de Pneumologia, Hospital Pedro Hispano, Matosinhos, Portugal
2Serviço de Infecciologia, Hospital Pedro Hispano, Matosinhos, Portugal
Abstract:
Introduction: Actinomycosis is a chronic bacterial infection that rarely affects the respiratory system. Lung infection usually develops after aspiration of oropharyngeal or gastrointestinal secretions. Typically, it presents with pneumonia, lung abscess or empyema, and the most common radiologic presentation is a pulmonary mass, simulating a tumour. Adequate treatment requires prolonged antibiotic therapy to prevent relapse. In this article we made a literature review on actinomycosis and analysed patients’ data from Pedro Hispano Hospital. Methods: Medical records from twelve-year data (January 2006 - December 2017) on pulmonary actinomycosis were consulted. Demographic and clinical data were retrospectively collected and analysed.
Results: Five patients were diagnosed with pulmonary actinomycosis, three males and two females. Mean age was 55 years. The most frequent microorganism was Actinomyces meyeri, identified in bronchoalveolar lavage in one case, and pleural fluid samples in other two cases. The other patients had isolation of Actinomyces odontolyticus and Actinomyces spp. All presented favourable response to treatment except for one patient, who died from empyema with septic shock. In one case, after a good therapeutic response, there was abandonment of the consultation and follow-up could not be maintained.
Conclusion: Presently, actinomycosis is a rare disease with good prognosis if diagnosed early and treated appropriately. It should always be considered as a differential diagnosis of a persistent parenchymal lung lesion.
Keywords: Actinomyces; Actinomycosis; Lung Diseases.
Resumo:
Introdução: A actinomicose é uma infeção bacteriana crónica que raramente afeta o sistema respiratório. A infeção pulmonar normalmente desenvolve-se após aspiração de secreções da orofaringe ou gastrintestinais. Tipicamente, apresenta-se como pneumonia, abcesso pulmonar ou empiema, sendo a apresentação radiológica mais comum uma massa pulmonar, simulando um tumor. O tratamento adequado requer antibioterapia prolongada para prevenir recidivas. Neste artigo fizemos uma revisão bibliográfica sobre actinomicose e analisámos dados de doentes do Hospital Pedro Hispano.
Métodos: Foram consultados registos médicos de doze anos (Janeiro 2006 - Dezembro 2017) sobre actinomicose pulmonar. Dados demográficos e clínicos foram colhidos e analisados retrospetivamente.
Resultados: Foram diagnosticados cinco doentes com actinomicose pulmonar, três do sexo masculino e dois do sexo feminino. A média de idades foi 55 anos. O microrganismo mais frequente foi o Actinomyces meyeri, identificado em amostras de lavado broncoalveolar num caso, e de líquido pleural em dois outros. Nos restantes casos, identificou-se Actinomyces odontolyticus e Actinomyces spp. Todos apresentaram evolução favorável com o tratamento excetuando um doente, que faleceu em contexto de empiema com choque séptico. Num dos casos, após melhoria inicial, houve abandono da consulta e não se conseguiu que retomasse o seguimento.
Conclusão: Atualmente, a actinomicose é uma patologia rara com bom prognóstico se diagnosticada precocemente e tratada de forma adequada. Deve ser sempre considerada no diagnóstico diferencial de uma lesão persistente do parênquima pulmonar.
Palavras-chave: Actinomicose; Actinomyces; Doenças do Pulmão.
Introduction
Actinomycosis is a rare infection caused by Actinomyces species, anaerobic Gram-positive bacilli, commensal from the oropharynx, gastrointestinal, skin and female genital tract. Lung disease represents 15% of all cases and usually develops after aspiration of oropharyngeal or gastrointestinal secretions.1-7 It is more common in men (fourth to fifth decades), and is associated with poor oral hygiene, dental procedures, structural lung disease and risk factors for aspiration, like alcoholism.1,2,4,6,7 Clinically, it presents with a slowly progressive pneumonia, lung abscess or empyema, with unspecific symptoms. A lung infiltrate or mass are the most common features in chest radiograph, leading to misdiagnosis with tuberculosis or cancer.1-4,7,8 Pleural involvement is present in 15% of all pulmonary cases.9 Although a rare cause of actinomycosis in humans, Actinomyces meyeri has a lung tropism and frequently disseminates, and for this reason, pulmonary forms may have worse prognosis.2,6,10 The isolation of Actinomyces spp. is essential to diagnosis, as well as the histopathological finding of characteristic yellowish sulphur granules in tissue samples.1,3,8 However, cultural tests are a difficult process because samples must be collected under strictly anaerobic conditions, and also because mixed infections are frequent.5 Invasive diagnostic techniques are often necessary.1,4,9 Treatment requires a prolonged course of antibiotics (6-12 months), and penicillin usually is the drug of choice.1,6-8 However, it must be individualized since thoracic forms frequently require longer courses, and some cases require surgical intervention.1,2,4-8,10
Actinomycosis incidence has been declining in the last four decades, although it may be underdiagnosed. It appears to have a poor correlation with the degree of immunosuppression, but more studies are required. At the present time, it is considered to have good prognosis if diagnosed early and treated appropriately, even in cases of disseminated disease.1,2,4,6,7,10
Because of the low prevalence of this disease and its usual delayed diagnosis, with a direct impact in the outcome, this study aimed to review the cases of pulmonary actinomycosis in our institution and to conclude about the relevance of considering this differential diagnosis in lung parenchymal lesions.
Methods
In a retrospective analysis of patients with pulmonary actinomycosis, between January 2006 and December 2017, in our institution, five patients were found. The diagnosis was based on microbiological findings (bronchoalveolar lavage, pleural fluid or abscess aspiration puncture samples). Demographic and clinical information (age, gender, smoking habits, risk factors for aspiration, periodontal disease, structural lung disease, symptoms, blood analysis, radiological appearance on chest radiograph and thorax computed tomography - CT, initial presumptive diagnosis, hospitalization, isolated microorganism, diagnostic procedures and treatment) were obtained from medical records and analysed for the present work.
This study has been approved by the Hospital Ethics Commission and Administrative Council.
Results
Clinical cases description
Patient 1
A 69-year-old male patient, former smoker (>100 pack-year), with high alcohol consumption, bronchiectasis and asthma-chronic obstructive pulmonary disease overlap (ACO). Admitted at the Emergency Department (ED) for dyspnea, cough, hemoptysis and weight loss (4 kg in 4 months). Thorax CT showed diffuse ground glass opacities, sparing only the left lower lobe. Due to previous antibiotics administration, he was treated empirically with piperacillin-tazobactam, considering respiratory infection. Because of clinical suspicion of pulmonary tuberculosis and scarce sputum, he was submitted to bronchofibroscopy. Actinomyces meyeri was isolated in bronchoalveolar lavage and intravenous ampicillin was initiated (total duration of 4 weeks), with good clinical response. At discharge, oral amoxicillin was prescribed for 10 months.
Patient 2
A 52-year-old male patient, active smoker with history of alcohol and drug abuse, dental abscess and congestive heart failure. Admitted at ED with aspiration pneumonia, in the context of methadone overdose with altered mental state. He was treated with empiric amoxicillin-clavulanate, with good clinical response and hospital discharge. He was readmitted the following week, with worsening of dyspnea and respiratory failure with pleural empyema and septic shock. Chest radiograph showed a left lung veiling opacity with mediastinum right deviation, and right lung nodular opacities. He started treatment with piperacillin-tazobactam and vancomycin, non-invasive ventilation, and was submitted to thoracentesis with pleural fluid drainage. The patient had an unfavourable outcome and died of acute pulmonary oedema, refractory to all therapeutic measures. Actinomyces meyeri was later isolated in a pleural fluid sample.
Patient 3
A 64-year-old female patient was admitted at ED with chest pain, respiratory failure and elevated inflammatory parameters. Chest radiography showed irregular right lung opacity, suggesting community-acquired pneumonia (CAP). Levofloxacin was prescribed and she was discharged. Readmitted 3 days later with worsening of symptoms and a pleural effusion in the right lung, evidenced in the chest radiograph. Thoracentesis was performed, and empiric ceftriaxone and azithromycin were initiated, with a total duration of 14 and 5 days, respectively. Pleural fluid had exudate criteria with polymorphonuclear (PMN) leukocytes dominance and Actinomyces meyeri was eventually isolated. After discharge, she was lost to follow-up, so treatment could not be completed.
Patient 4
A 62-year-old male patient, former smoker of 20 pack-year. Admitted at ED with back pain, anorexia, fatigue and dyspnea with 15 days of evolution and a history of dental procedures performed 3 months prior to this condition. Thorax CT showed a left loculated pleural effusion with lung atelectasis. He was hospitalized for sepsis with empyema and started treatment with imipenem. A surgery for lysis of adhesions and pleuropulmonary decortication was performed, and Actinomyces odontolyticus was isolated in pleural fluid. After a good clinical response, he was discharged with oral clindamycin (12 months), due to ampicillin allergy. On follow-up, after the end of antibiotics, he remained asymptomatic and presented only minor fibrotic lesions on thorax CT.
Patient 5
A 26-year-old female patient, with type 1 diabetes mellitus, severe periodontal disease and recent right inferior lung lobe pneumonia. Admitted at ED with pleuritic thoracic pain and cough for 7 days. She was hospitalized with right inferior lobe lung abscess, evidenced in thorax CT, and started treatment with ceftriaxone and clindamycin, posteriorly escalated to piperacillin-tazobactam. After isolation of Actinomyces spp. from abscess aspiration puncture, performed in the Intensive Care Unit, intravenous ampicillin was prescribed for 4 weeks, followed by oral amoxicillin for 7 months. Control thorax CT taken 6 months later, evidenced only residual densifications.
Patients characteristics:
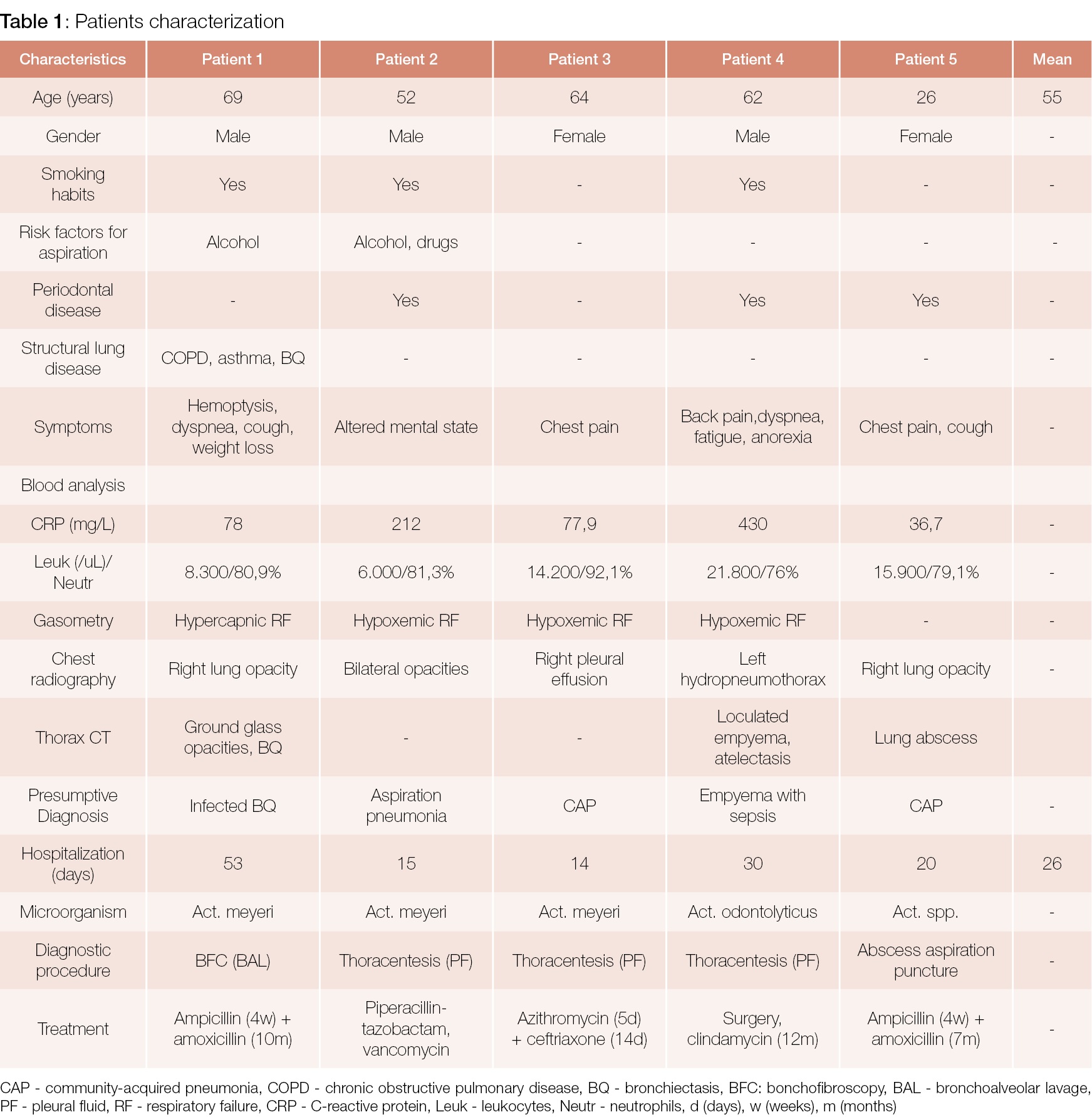
Patients characteristics are listed and summarized in Table 1.
The mean age was 55 years (26-69 years); three males and two females were included. Three patients had smoking habits, two had alcohol drinking habits, one had history of drug consumption. Three patients had history of dental procedures or periodontal disease. Only patient 1 had structural lung disease (ACO and bronchiectasis).
Clinical presentation:
The most common presenting symptoms at hospital admission were non-specific and consisted of chest pain, cough and dyspnea. Chest pain was the only symptom reported by patient 3. Only patient 1, who had structural lung disease (bronchiectasis, ACO), presented with hemoptysis. Altered mental state was the clinical presentation of patient 2, but in context of methadone abuse and aspiration pneumonia, and was not reported in any other patient. Fatigue and anorexia were other less common symptoms, reported only by patient 4. No patient presented with fever at hospital admission.
Analytic parameters evidenced elevated c-reactive protein (CRP) (36.7-430 mg/L) in all patients, and leucocytosis with neutrophilia in three of them (patients 3, 4 and 5). Patient 4 presented with the most prominent inflammatory response observed, revealing a CRP value of 430 mg/L and a leucocytosis of 21.800/μL, in the context of sepsis with empyema. On the other hand, patient 2, who also developed empyema with septic shock, had no leucocytosis at ED admission and presented a CRP of 212 mg/L. Patient 5 had lower elevation in CRP (36,7mg/L).
Three patients presented with hypoxemic respiratory failure (patients 2, 3, 4), one patient with hypercapnic respiratory failure (patient 1, who had structural lung disease) and one patient with no significant arterial blood gases changes.
Radiological presentation:
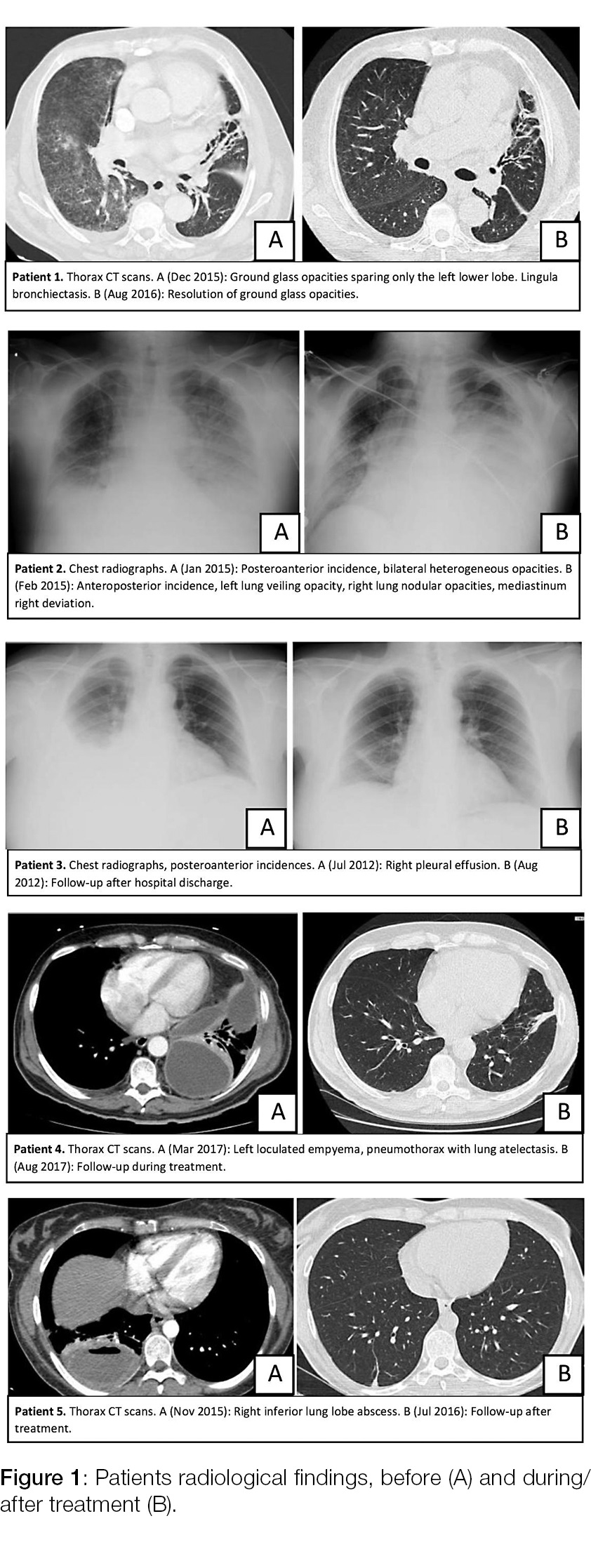
Chest radiographs were performed, and the most common finding was a chest opacity (irregular and poorly defined in patients 1, 2 and 5; well delimited in patients 3 and 4, suggesting a pleural effusion). Three patients performed thorax CT: patient 1 evidenced bilateral ground glass opacities and bronchiectasis, patient 4 evidenced a loculated pleural effusion (empyema) with lung atelectasis, and patient 5 a lung abscess (Fig. 1).
Diagnosis:
None of the patients had suspected pulmonary actinomycosis at presentation. The most common presumptive diagnosis at hospital admission was CAP.
To achieve a correct diagnosis with Actinomyces isolation, microbiological analysis of pleural fluid obtained by thoracentesis proved to be the most useful complementary test. Patient 1 was diagnosed with bronchoalveolar lavage analysis and patient 5 with lung abscess aspiration puncture, due to low probability of obtaining uncontaminated specimens with other diagnostic methods.
Hospitalization:
All patients were hospitalized. Total mean time of hospitalization was 26 days.
Patient 2 and 4 were admitted with complicated forms of pulmonary actinomycosis, developing a sepsis from empyema. Patient 3 developed an empyema, too. Patient 5 was admitted with a lung abscess, a possible finding at presentation. Patient 1 presented with hemoptysis.
Treatment:
All patients began empiric intravenous antibiotic treatment at hospital admission regarding the most probable diagnosis at the ED (CAP or other). After the correct diagnosis of pulmonary actinomycosis, initial intravenous antibiotic of choice was ampicillin with a mean treatment duration of 30 days. At hospital discharge, oral antibiotic was prescribed, and amoxicillin was the preferred treatment. Duration of oral antibiotic therapy varied; patient 5 completed 7 months of amoxicillin, patient 1 was treated with 10 months of amoxicillin, and patient 4 completed 12 months of clindamycin, due to allergic reaction to ampicillin.
Only one patient was submitted to surgical treatment (patient 4) for lysis of adhesions and pleuropulmonary decortication due to a loculated empyema. Excluding patient 2 (who died of septic shock) and patient 3 (who was lost to follow-up), all patients showed good therapeutic response after the correct diagnosis and specific antibiotic treatment.
Discussion
In the present study, medical records from twelve-year data on pulmonary actinomycosis from Pedro Hispano Hospital were analysed. Only five cases were identified, or had medical records available, and none of them had this condition as differential diagnosis at hospital admission. This reflects the fact that pulmonary actinomycosis is a rare and possibly underdiagnosed condition, that presents with unspecific symptoms, also seen in more frequent diseases like CAP.
Actinomyces meyeri was the most isolated microorganism, which is not surprising since it is the most often responsible agent for lung infection. Although cultural identification of the species is a difficult process, since it requires strictly anaerobic conditions, none of the patients required lung biopsy, which is often essential for definitive diagnosis. In one patient there was isolation with abscess puncture technique.
We found three cases of actinomycosis with pleural involvement, manifesting with pleural effusions or empyema. Two cases had identification of A. meyeri, and one case A. odontolyticus (patient 4) that caused only pleural disease with no significant parenchymal affection, a very rare manifestation of this species.9
According to literature, actinomycosis is usually a benign condition if diagnosed and treated appropriately. However, in this series one patient had an unfavourable evolution, refractory to treatment, and died.
Treatment with antibiotics is usually long (up to 12 months), as seen in the patients with hospital discharge. Only one patient was treated with a short course of antibiotics (14 days), initially misdiagnosed with CAP, and then lost to follow-up without possibility to begin adequate treatment.
A major limitation of this study is its small number of clinical cases, probably due to a relatively short period of time to analyse this rare disease, considering it may be underdiagnosed.
Conclusion
As described in our study, the diagnosis of pulmonary actinomycosis is challenging and requires a combination of compatible clinical and imagological findings, microbiological isolation of the specimen, histological evidence of sulphuric granules, and a good response to therapy. The prognosis is usually good, if diagnosed early and treated appropriately. Thus, it should always be considered as a differential diagnosis of a persistent parenchymal lesion, especially when underlying conditions are favourable to the infection.
REFERÊNCIAS
1. Kim S, Jung L, Oh I, Kim Y, Shin K, Lee M, et al. Pulmonary actinomycosis during the first decade of 21st century: cases of 94 patients. BMC Infect Dis. 2013;13:216. doi: 10.1186/1471-2334-13-216. [ Links ]
2. Mabeza G, Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003;21:545-51. [ Links ]
3. Kobashi Y, Yoshida K, Miyashita N, Niki Y, Matsushima T. Thoracic actinomycosis with mainly pleural involvement. J Infect Chemother. 2004;10:172-7. [ Links ]
4. Yildiz O, Doganay M. Actinomycosis and nocardia pulmonary infections. Curr Opin Pulm Med. 2006;12:228-34. [ Links ]
5. Higashi Y, Nakamura S, Ashizawa N, Oshima K, Tanaka A, Miyazaki T, et al. Pulmonary actinomycosis mimicking pulmonary aspergilloma and a brief review of the literature Intern Med 2017;56:449-53. doi: 10.2169/internalmedicine.56.7620. [ Links ]
6. Fazili T, Blair D, Riddell S, Kiska D, Nagra S. Actinomyces meyeri infection: Case report and review of the literature. Case Rep Infect Dis. 2015;2015:291838. doi: 10.1155/2015/291838. [ Links ]
7. Sullivan D, Chapman S. Bacteria that masquerade as fungi: actinomycosis/nocardia. Proc Am Thorac Soc. 2010;7:216-21. doi: 10.1513/pats.200907-077AL. [ Links ]
8. Qiu L, Lan L, Feng Y, Huang Z, Chen Y. Pulmonary actinomycosis imitating lung cancer on F-FDG PET/CT: a case report and literature review. Korean J Radiol. 2015;16:1262-5. doi: 10.3348/kjr.2015.16.6.1262. [ Links ]
9. Malik R, Keshwani N, Beegle S. First case of Actinomyces Odontolyticus pleural effusion Chest 2016;150:590A. [ Links ]
10. Park H, Park K, Kim S, Sung H, Choi S, Kim Y, et al. A case of disseminated infection due to Actinomyces meyeri Involving lung and brain. Infect Chemother. 2014;46:269-73. doi: 10.3947/ic.2014.46.4.269. [ Links ]
Acknowledgements
We would like to thank the following colleagues for their valuable contribution for this article:
Eduarda Pena1, Marília Silva2, Sofia Correia2, Cristina Rodrigues3
1Medical Intern of Infectious Diseases Department, at Pedro Hispano Hospital, Matosinhos, Portugal
2Medical Intern of Internal Medicine Department, at Pedro Hispano Hospital, Matosinhos, Portugal
3Physician of Internal Medicine Department, at Pedro Hispano Hospital, Matosinhos, Portugal.
Responsabilidades Éticas
Conflitos de Interesse: Os autores declaram a inexistência de conflitos de interesse na realização do presente trabalho.
Fontes de Financiamento: Não existiram fontes externas de financiamento para a realização deste artigo.
Confidencialidade dos Dados: Os autores declaram ter seguido os protocolos da sua instituição acerca da publicação dos dados de doentes.
Proteção de Pessoas e Animais: Os autores declaram que os procedimentos seguidos estavam de acordo com os regulamentos estabelecidos pelos responsáveis da Comissão de Investigação Clínica e Ética e de acordo com a Declaração de Helsínquia da Associação Médica Mundial.
Proveniência e Revisão por Pares: Não comissionado; revisão externa por pares.
Ethical Disclosures
Conflicts of interest: The authors have no conflicts of interest to declare.
Financing Support: This work has not received any contribution, grant or scholarship.
Confidentiality of Data: The authors declare that they have followed the protocols of their work center on the publication of data from patients.
Protection of Human and Animal Subjects: The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Provenance and Peer Review: Not commissioned; externally peer reviewed.
© Autor (es) (ou seu (s) empregador (es)) 2019. Reutilização permitida de acordo com CC BY-NC. Nenhuma reutilização comercial.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use.
Correspondence / Correspondência:
Bruno Cabrita – bmcabrita@gmail.com
Serviço de Pneumologia, Hospital Pedro Hispano, Matosinhos, Portugal
Morada: Rua Dr. Eduardo Torres / 4464-513 Senhora da Hora
Received / Recebido: 29/01/2019
Accepted / Aceite: 06/06/2019
Publicado / Published: 17 de Março de 2020


{kind=link}
{kind=link}