










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMedicina Interna
versão impressa ISSN 0872-671X
Medicina Interna vol.25 no.4 Lisboa dez. 2018
https://doi.org/10.24950/rspmi/revisao/4/2018
ARTIGOS DE REVISÃO / REVIEW ARTICLES
Antiphospholipid syndrome
Síndrome antifosfolipídica
Ricard Cervera, Gerard Espinosa
Department of Autoimmune Diseases, Hospital Clínic, Barcelona, Catalonia, Spain
ABSTRACT
The antiphospholipid syndrome (APS) is defined by the development of venous and/or arterial thromboses, often multiple, and pregnancy morbidity (mainly, recurrent fetal losses), in the presence of antiphospholipid antibodies (aPL). Some estimates indicate that the incidence of the APS is around 5 new cases per 100 000 persons per year and the prevalence around 40-50 cases per 100 000 persons. The aPL are positive in approximately 13% of patients with stroke, 11% with myocardial infarction, 9.5% of patients with deep vein thrombosis and 6% of patients with pregnancy morbidity.
Currently, there is consensus in treating APS patients with thrombosis with long-term oral anticoagulation and to prevent obstetric manifestations with the use of aspirin and heparin. This review summarizes the main knowledge on the clinical and therapeutic aspects of this syndrome.
Keywords: Antibodies, Anticardiolipin; Antibodies, Antiphospholipid; Antiphospholipid Syndrome; Stroke
RESUMO
A síndrome antifosfolipídica (SAF) carateriza-se pelo desenvolvimento de tromboses venosas e/ou arteriais, muitas vezes múltiplas, e pela morbidade gestacional (por perdas fetais recorrentes), na presença de anticorpos antifosfolipídicos. As estimativas indicam que a incidência da SAF é de cerca de 5 novos casos por 100 000 pessoas por ano e a prevalência é de cerca de 40-50 casos por 100 000 pessoas. Os aPL são positivos em aproximadamente 13% dos pacientes com acidente vascular cerebral, 11% com enfarte do miocárdio, 9,5% dos pacientes com trombose venosa profunda e 6% dos pacientes com morbidade gestacional.
Atualmente, há consenso no tratamento de pacientes com SAF com trombose com anticoagulação oral de longa duração e para evitar manifestações obstétricas com o uso de aspirina e heparina. Esta revisão resume os principais conhecimentos sobre os aspectos clínicos e terapêuticos desta síndrome.
Palavras-chave: Acidente Vascular Cerebral; Anticorpos Anticardiolipina; Anticorpos Antifosfolipídeos; Síndrome Antifosfolipídica
Introduction
The antiphospholipid syndrome (APS) is characterized by the development of venous and/or arterial thromboses, often multiple, and pregnancy morbidity (mainly, recurrent fetal losses), in the presence of antiphospholipid antibodies (aPL), namely lupus anticoagulant (LA), anticardiolipin antibodies (aCL), or anti-ß2glycoprotein-I (ß2GPI) antibodies.1-4
The APS can be found in patients having neither clinical nor laboratory evidence of another definable condition (primary APS) or it may be associated with other diseases, mainly systemic lupus erythematosus (SLE), but occasionally with other autoimmune conditions,1 infections,2 drugs,1 and malignancies.3 A minority of APS patients can develop a devastating variant termed catastrophic APS.5
Epidemiology
The aPL can appear in different scenarios, such as asymptomatic aPL carrier patients, thrombotic APS with recurrent venous and/or arterial thrombosis, obstetric APS affecting otherwise healthy women with recurrent pregnancy loss, patients with non-APS classification criteria manifestations (i.e, thrombocytopenia, hemolytic anemia or livedo reticularis) or with catastrophic APS.5
Prevalence of the aPL in the general population ranges between 1% - 5%. However, only a minout together all the published case reports as well as the new diagnosed cases from all over the world, an international registry of patients with catastrophic APS ("CAPS Registry") was crerity of these individuals develop the APS. Some estimates indicate that the incidence of the APS is around 5 new cases per 100 000 persons per year and the prevalence around 40-50 cases per 100 000 persons.6 Specifically, aPL are positive in approximately 13% of patients with stroke, 11% with myocardial infarction (MI), 9.5% of patients with deep vein thrombosis (DVT) and 6% of patients with pregnancy morbidity.7
The prevalence of the catastrophic APS is scarce (less than 1% of all cases of APS).5,8,9 In order to pated in 2000 by the European Forum on Antiphospholipid Antibodies. Currently, it documents the entire clinical, laboratory and therapeutic data of more than 500 patients.5
Pathogenesis
Autoantibodies associated with APS are directed against a number of proteins of the plasma or expressed on, or bound to, the surface of vascular endothelial cells or platelets. The involvement of aPL in clinically important normal procoagulant and anticoagulant reactions and on certain cells altering the expression and secretion of various molecules are the basis for possible mechanisms by which aPL may develop thrombotic events in patients with APS. In depth reviews of these mechanisms can be found elsewhere.10,11
Clinical Manifestations
The clinical picture of the APS is characterized by venous and arterial thromboses, pregnancy morbidity (mainly, fetal losses) and moderate thrombocytopenia. Single vessel involvement or multiple vascular occlusions may give rise to a wide variety of presentations. Any combination of vascular occlusive events may occur in the same individual and the time interval between them also varies considerably from weeks to months or even years.12-14 The prevalence of the main manifestations in a cohort of 1000 patients with APS (“Euro-Phospholipid Project”) are collected in Table 1.12
Several attempts have been made in order to identify the individual risk of thrombosis in aPL positive patients.15,16 A study of pregnant women with APS reported that patients with triple aPL positivity (ie, positivity for LA, aCL, and anti-ß2GPI) and/or previous thromboembolism had an increased likelihood of poor neonatal outcomes than patients with double or single aPL positivity and no thrombosis history.15 More recently, a global APS score (GAPSS) was developed in a cohort of 211 SLE from a single centre after the combination of several independent risk factors for both thrombosis and pregnancy loss. The final score includes 6 factors with different weights: IgG/IgM aCL (5 points), IgG/IgM anti-ß2GPI antibodies (4 points), LA (4 points), IgG/ IgM anti-phosphatidylserine–prothrombin complex antibodies (3 points), hyperlipidemia (3 points) and arterial hypertension (1 point). A GAPSS cut-off value higher than 10 points appears to have the best prognostic yield.16
Classification Criteria
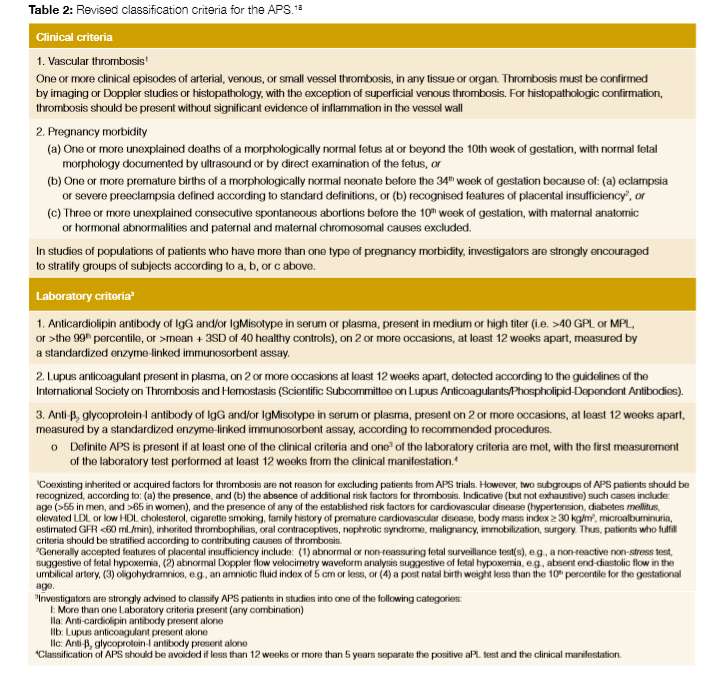
A preliminary classification set of criteria was established after an expert workshop held in Sapporo, Japan, in 1999.17 These classification criteria were updated in another workshop was held in Sydney, Australia, in 2006 in which the experts proposed the inclusion of anti-ß2GPI antibodies. Although no new clinical criteria were added, some particular features were remarked on, such as associated APS features, including cardiac valve involvement, livedo reticularis, thrombocytopenia, APS nephropathy, and non-thrombotic central nervous system manifestations (i.e. cognitive dysfunction)18 (Table 2).
This revised APS classification criteria19 provide a more uniform basis for selecting patients for APS research by emphasising risk stratification. They strongly recommend investigating coexisting inherited and acquired thrombosis risk factors in patients with APS, especially in those who are included in clinical trials. An assessment of these 2006 revised APS classification criteria has shown that only 59% of the patients meeting the 1999 APS Sapporo classification criteria met the revised criteria.19
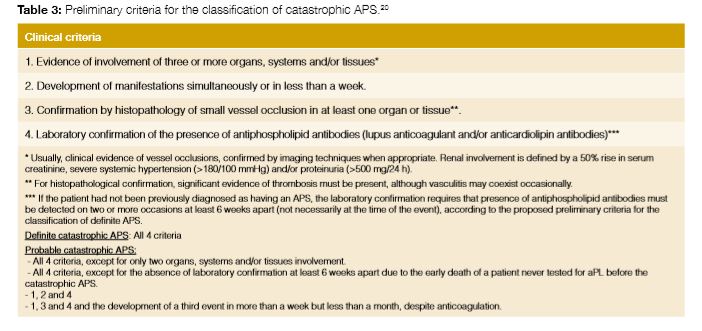
The preliminary classification criteria for catastrophic APS were formulated at a workshop in Taormina, Italy, in 2002, during the 10th International Congress on aPL (Table 3).20 A validation study showed that they have a sensitivity of 90.3%, a specificity of 99.4%, a positive predictive value of 99.4% and a negative predictive value of 91.1%.21 A recent evidence-based set of guidelines for the diagnosis and management of catastrophic APS has formulated the recommendation that these classification criteria can be also used as diagnostic criteria.22
Treatment
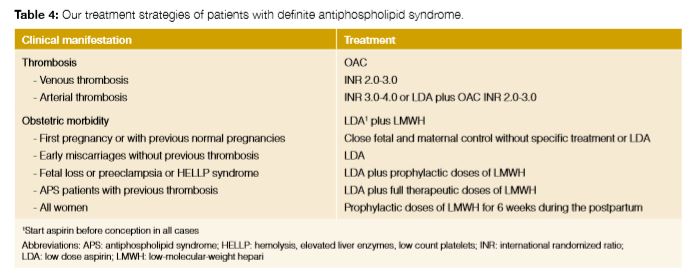
Treatment of thrombosis in APS patients is based on long-term oral anticoagulation and treatment of obstetric manifestations on the use of aspirin and heparin.23 These recommendations are based on randomized controlled trials and observational studies (Table 4). In detail, patients with definite APS with first venous thrombosis have to be treated with prolonged oral anticoagulation at a target international normalized ratio (INR) of 2.0-3.0. Anticoagulation at INR of 3.0-4.0, isolated antiaggregation, anticoagulation at INR 2.0-3.0 or anticoagulation at INR 2.0-3.0 plus antiaggregation have been proposed for definite APS patients with arterial thrombosis. Regarding obstetric APS, although combined therapy with low-dose aspirin and low-molecular-weight heparin is the mainstay of treatment in women with obstetric APS, the strength of evidence of its efficacy is under discussion.24
Otherwise, in the field of APS there are grey areas where the evidence is scarce and where the management of certain patients is difficult. Some examples are patients with “seronegative” APS, those who do not display formal (clinical or laboratory) classification criteria for APS, those with refractory APS despite optimal treatment (recurrent thrombotic events despite optimal anticoagulation or recurrent fetal losses despite the combination of aspirin and low molecular weight heparin), and the treatment of clinical manifestations not included in the classification criteria such as hematologic manifestations (thrombocytopenia and haemolytic anemia), neurologic manifestations (chorea, myelitis or multiple sclerosis-like lesions), nephropathy and heart valve disease associated with antiphospholipid antibodies. In these cases, the recommendations are based on the common sense since the published evidence is scarce or it does not exist.23
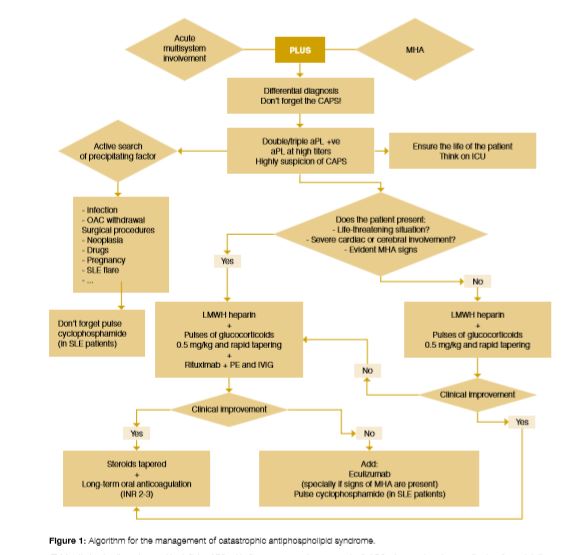
In cases of catastrophic APS, an aggressive treatment is required (Fig 1). Therefore, early diagnosis is very important to start adequate therapy and decrease the high mortality rate of these patients. Once the diagnosis is made or suspected, searching and treating the precipitating factor, mainly infection, is the first step of treatment. The specific therapy of catastrophic APS is the combination of anticoagulation with heparin, and corticosteroids as first line of treatment. Additionally adding intravenous immunoglobulins and/or plasma exchange have to be considered in life-threatening cases. In patients with associated SLE, intravenous cyclophosphamide has demonstrated be beneficial. In refractory cases, rituximab or eculizumab should be added.22,25
Outcome and Organ Damage
Given that APS affect predominantly young patients, assesment of organ damage is crucial but evidence in that field is limited. A retrospective analysis was published that focused in morbidity, mortality, and organ damage in 135 APS patients (89 primary APS and 46 with secondary APS).26 Patients were clustered according to the initial event: arterial thrombosis, DVT or pregnancy morbidity. One-fourth of the patients progressed to organ damage in a mean time of 10 years from disease onset. The highest morbidity was attributed to neurologic damage, which was more common among patients with arterial thrombosis as an initial manifestation.
During the follow-up study period of the “Euro-Phospholipid Project”, a 10-year survival rate of 91% was reported.14 During this follow-up period, 93 (9.3%) patients died. The main causes of death were thrombosis (36.5%) and infections (26.9%).
Patients with APS still develop significant morbidity and mortality despite current treatment (mainly oral anticoagulants and/ or antiaggregant agents); therefore, it is imperative to increase the effort in determining optimal prognostic markers and therapeutic measures to prevent these important complications of the APS.
Referências
1. Cervera R, Espinosa, Khamashta MA. Antiphospholipid syndrome in systemic autoimmune diseases. 2nd ed. Amsterdam: Elsevier; 2016. [ Links ]
2. Cervera R, Asherson RA, Acevedo ML, Gomez-Puerta JA, Espinosa G, De La Red G, et al. Antiphospholipid syndrome associated with infections: clinical and microbiological characteristics of 100 patients. Ann Rheum Dis. 2004;63:1312-7. [ Links ]
3. Gómez-Puerta JA, Cervera R, Espinosa G, Aguiló S, Bucciarelli S, Ramos-Casals M, et al. Antiphospholipid antibodies associated with malignancies: clinical and pathological characteristics of 120 patients. Semin Arthritis Rheum. 2006;35:322-32. [ Links ]
4. Gómez-Puerta JA, Martin H, Amigo MC, Aguirre MA, Camps MT, Cuadrado MJ, et al. Long-term follow-up in 128 patients with primary antiphospholipid syndrome: do they develop lupus? Medicine. 2005;84:225-30. [ Links ]
5. Rodríguez-Pintó I, Moitinho M, Santacreu I, Shoenfeld Y, Erkan D, Espinosa G, et al. Catastrophic antiphospholipid syndrome (CAPS): Descriptive analysis of 500 patients from the International CAPS Registry.Autoimmun Rev. 2016;15:1120-4. doi: 10.1016/j.autrev.2016.09.010. [ Links ]
6. Durcan L, Petri M. Epidemiology of the Antiphospholipid Syndrome. In: Cervera R, Espinosa, Khamashta MA, editors. Antiphospholipid syndrome in systemic autoimmune diseases. 2nd ed. Amsterdam: Elsevier; 2016.p. 17-30. [ Links ]
7. Andreoli L, Chighizola CB, Banzato A, Pons-Estel GJ, Ramire de Jesus G, Erkan D. Estimated frequency of antiphospholipid antibodies in patients with pregnancy morbidity, stroke, myocardial infarction, and deep vein thrombosis: a critical review of the literature.Arthritis Care Res. 2013; 65: 1869-73. doi: 10.1002/acr.22066. [ Links ]
8. Cervera R, Espinosa G, Bucciarelli S, Gomez-Puerta JA, Font J. Lessons from the catastrophic antiphospholipid syndrome (CAPS) registry. Autoimmun Rev. 2006;6:81-4. [ Links ]
9. Cervera R, Bucciarelli S, Plasin MA, Gomez-Puerta JA, Plaza J, Pons-Estel G, et al. Catastrophic antiphospholipid syndrome (CAPS): descriptive analysis of a series of 280 patients from the "CAPS Registry". J Autoimmun. 2009;32:2405. doi: 10.1016/j.jaut.2009.02.008. [ Links ]
10. Espinosa G, Cervera R. Antiphospholipid syndrome: frequency, main causes and risk factors of mortality. Nat Rev Rheumatol. 2010; 6: 296-300. doi: 10.1038/nrrheum.2010.47. [ Links ]
11. Giannakopoulos B, Krilis SA. The pathogenesis of the antiphospholipid syndrome. N Engl J Med. 2013;368:1033-44. doi: 10.1056/NEJMra1112830. [ Links ]
12. Cervera R, Piette JC, Font J, Khamashta MA, Shoenfeld Y, Camps MT, et al. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheumatol. 2002;46:1019-27. [ Links ]
13. Cervera R, Khamashta MA, Shoenfeld Y, Camps MT, Jacobsen S, Kiss E, et al. Morbidity and mortality in the antiphospholipid syndrome during a 5-year period: a multicentre prospective study of 1000 patients. Ann Rheum Dis. 2009;68:1428-32. doi: 10.1136/ard.2008.093179. [ Links ]
14. Cervera R, Serrano R, Pons-Estel GJ, Ceberio-Hualde L, Shoenfeld Y, de Ramón E, et al. Morbidity and mortality in the antiphospholipid syndrome during a 10-year period: a multicentre prospective study of 1000 patients. Ann Rheum Dis. 2015; 74: 1011-8. doi: 10.1136/annrheumdis-2013-204838. [ Links ]
15. Ruffatti A, Calligaro A, Hoxha A, Trevisanuto D, Ruffatti AT, Gervasi MT, et al. Laboratory and clinical features of pregnant women with antiphospholipid syndrome and neonatal outcome. Arthritis Care Res. 2010;62:302-7. doi: 10.1002/acr.20098. [ Links ]
16. Sciascia S, Sanna G, Murru V, Roccatello D, Khamashta MA, Bertolaccini ML. GAPSS: the Global Anti-Phospholipid Syndrome Score. Rheumatology. 2013;52:1397-403. doi: 10.1093/rheumatology/kes388. [ Links ]
17. Wilson WA, Gharavi AE, Koike T, Lockshin MD, Branch DW, Piette JC, et al. International consensus statement on preliminary classification criteria for definite antiphospholipid syndrome: report of an international workshop. Arthritis Rheumatol. 1999;42:1309-11. [ Links ]
18. Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4:295306. [ Links ]
19. Kaul M, Erkan D, Sammaritano L, Lockshin MD. Assessment of the 2006 revised antiphospholipid syndrome classification criteria. Ann Rheum Dis. 2007;66:927-30. [ Links ]
20. Asherson RA, Cervera R, de Groot PG, Erkan D, Boffa MC, Piette JC, et al. Catastrophic antiphospholipid syndrome: International consensus statement on classification criteria and treatment guidelines. Lupus. 2003;12:530-4. [ Links ]
21. Cervera R, Font J, Gomez-Puerta JA, Espinosa G, Cucho M, Bucciarelli S, et al. Validation of the preliminary criteria for the classification of catastrophic antiphospholipid syndrome. Ann Rheum Dis. 2005;64:1205-9. [ Links ]
22. Legault K, Schunemann H, Hillis C, Yeung C, Akl EA, Carrier M, et al. McMaster RARE-Bestpractices clinical practice guideline on diagnosis and management of the catastrophic antiphospholipid syndrome. J Thromb Haemost. 2018 (in press). doi: 10.1111/jth.14192. [ Links ]
23. Espinosa G, Cervera R. Current treatment of antiphospholipid syndrome: lights and shadows. Nat Rev Rheumatol. 2015;11:586-96. doi: 10.1038/nrrheum.2015.88. [ Links ]
24. Chighizola CB, Andreoli L, Gerosa M, Tincani A, Ruffatti A, Meroni PL. The treatment of anti-phospholipid syndrome: A comprehensive clinical approach. J Autoimmun. 2018;90:1-27. doi: 10.1016/j.jaut.2018.02.003. [ Links ]
25. Cervera R, Rodríguez-Pintó I, Espinosa G. The diagnosis and clinical management of the catastrophic antiphospholipid syndrome: A comprehensive review. J Autoimmun. 2018;92:1-11. doi: 10.1016/j.jaut.2018.05.007. [ Links ]
26. Grika EP, Ziakas PD, Zintzaras E, Moutsopoulos HM, Vlachoyiannopoulos PG. Morbidity, mortality, and organ damage in patients with antiphospholipid syndrome. J Rheumatol. 2012;39:516-23. doi: 10.3899/jrheum.110800. [ Links ]
Correspondência:Marta Vaz Batista martafilipavaz@gmail.com
Serviço de Medicina 1, Hospital Professor Doutor Fernando Fonseca, Amadora, Portugal
IC 19 - 2720-276 Amadora
Conflitos de Interesse: Os autores declaram a inexistência de conflitos de interesse na realização do presente trabalho.
Fontes de Financiamento: Não existiram fontes externas de financiamento para a realização deste artigo.
Conflicts of interest: The authors have no conflicts of interest to declare.
Financing Support: This work has not received any contribution, grant or scholarship.
Recebido: 09/09/2018
Aceite:30/09/2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}