










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkNascer e Crescer
Print version ISSN 0872-0754On-line version ISSN 2183-9417
Nascer e Crescer vol.27 no.4 Porto Dec. 2018
https://doi.org/10.25753/BirthGrowthMJ.v27.i4.14236
REVIEW ARTICLES | ARTIGOS DE REVISÃO
Fever from Primary Tooth Eruption - What is the evidence?
Febre durante a erupção dentária primária - Há evidência?
Sara MatosI, Patrícia SilvaI
I General and Family Practice, Unidade de Saúde Familiar Navegantes, Agrupamento de Centros de Saúde Grande Porto IV. 4480-793 Vila do Conde, Portugal. smatos@arsnorte.min-saude.pt; pagsilva@arsnorte.min-saude.pt
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: There is no consensus on the causal relationship between primary dental eruption and both systemic and local signs and symptoms. Fever, an important sign, is often reported. Such lack of evidence hampers clinical reasoning and may contribute to delayed diagnosis of important conditions.
Objective: To review existing evidence underlying the association between primary tooth eruption and fever.
Methods: A review of the evidence on English, Portuguese and Spanish scientific publications over the last ten years was performed in the main international databases using the query “tooth eruption” and “fever” [MeSH], and in the index of Portuguese medical journals using the query “erupção dentária” and “febre” [DeCS]. SORT system of the American Family Physician was used for rating the strength of evidence.
Results: A total of 53 articles were retrieved, from which two meta-analyses and two original studies were selected, comprising a total of 5317 children. Massignan et al. (2016) meta-analysis and Memarpour et al. (2015) clinical trial found a slight temperature increase on the day of primary tooth eruption, but no fever. In Nemezio et al. (2017) meta-analysis, this association was observed in the subgroup that used the rectal method for temperature assessment. Un Lam et al. (2016) observational study reported a fever prevalence of 49.9%.
Discussion and conclusions: The present analysis had several limitations, including a significant heterogeneity amongst studies in the definition of fever, interpersonal variability during fever measurements, different fever assessment methods or absence of that information, and no exclusion of confounding factors. Given available evidence, it is not possible to establish a clear association between primary dental eruption and the occurrence of fever. A higher number of robust studies is required to confirm this hypothesis (SORT B).
Keywords: Dental eruption; Fever; Infant
RESUMO
Introdução: Não existe consenso na literatura sobre a existência de uma relação causal entre erupção dentária primária e ocorrência de sinais e sintomas sistémicos e locais. A febre, um importante sinal clínico, é frequentemente reportada por pais e profissionais de saúde. A falta de evidência dificulta o raciocínio clínico, podendo contribuir para atrasos no diagnóstico de patologias importantes associadas a este sintoma.
Objetivo: Rever a evidência disponível acerca de uma associação entre erupção dentária primária em lactentes e o aparecimento de febre.
Métodos: Foi efetuada uma pesquisa de artigos científicos em Inglês, Português e Espanhol publicados nos últimos dez anos nas principais bases de dados médicas internacionais utilizando os termos MeSH “tooth eruption” e “fever”, e no índice de revistas médicas Portuguesas utilizando os termos DeCS “erupção dentária” e “febre”. Foi utilizada a escala SORT da American Family Physician para avaliar os níveis de evidência.
Resultados: Foram identificadas 53 publicações, das quais foram selecionados duas meta-análises e dois artigos originais, abrangendo um total de 5317 crianças. Na meta-análise de Massignan et al. (2016) e no ensaio clínico de Memarpour et al. (2015), verificou-se um ligeiro aumento da temperatura no dia da erução dentária primária, mas não foi descrita a ocorrência de febre. Na meta-análise de Nemezio et al. (2017), essa associação foi encontrada no subgrupo que utilizou o método retal para medição da temperatura. O estudo observacional de Un Lam et al. (2016) encontrou uma prevalência de febre de 49,9%.
Discussão e conclusões: A presente análise tem várias limitações: uma grande heterogeneidade entre estudos na definição de febre, variabilidade interpessoal na realização das respetivas medições, utilização de diferentes métodos de medição de febre ou ausência de referência ao mesmo, e ausência de exclusão de fatores de confundimento. Perante a evidência disponível, não é possível confirmar a existência de uma associação entre erupção dentária primária e febre, sendo necessários mais estudos robustos para avaliar esta hipótese (SORT B).
Palavras-chave: Criança; Erupção dentária; Febre
Introduction
Eruption of an infant’s first tooth is often considered one of the most significant landmarks in the child’s development.1 Primary tooth eruption (PTE) usually begins between the forth and tenth months of age, taking place during an eight-day window period including the four days prior to tooth eruption, the day of eruption, and the three days afterwards.2,3 PTE is a physiological process consisting in the movement of teeth from their initial position within the alveolar bone of the jaw towards the gingiva, emerging in the oral cavity. The driving force that promotes PTE is not well established to date.4
Some authors have associated PTE with the development of several local or systemic signs and symptoms, including fever, general irritability, sleep disturbances, crying, rhinorrhea, facial flushing, diarrhea, loss of appetite, increased salivation, inflammation, and gingival hyperemia.1,2,4-7
Many parents and health care professionals strongly believe that PTE is the cause of such local and systemic manifestations.4 However, there is no consensus to date on the causal relationship between such factors, and those symptoms are often attributed to popular beliefs instead of supported by scientific evidence. In fact, it remains unclear whether such manifestations are triggered by PTE or simply coincident with the eruption of the first teeth.8 Expression of local and systemic symptoms during teeth eruption is a frequent driver for parents to seek medical or dental advice and, sometimes, even to administer over-the-counter drugs to relieve the child’s discomfort.5,8
Fever, an important symptom associated with several childhood diseases, is one of the most frequently reported by parents and health professionals.6,9 Several medical decisions, both investigational and therapeutic, are based on body temperature assessment.9 The lack of scientific evidence hinders diagnostic reasoning and may contribute to delayed diagnosis and treatment of major diseases.8
As a subject still requiring clarification, this review aimed to investigate existing evidence regarding the association between PTE and the onset of fever in infants.
Methods
A literature survey was performed in the main medical international databases for meta-analyses (MAs), systematic reviews (SRs), randomized controlled trials, observational studies, and clinical guidelines using the MeSH terms “tooth eruption” and “fever”. Portuguese medical journals’ indexes were also scanned using the search terms (DeCS) “ erupção dentária “ and “febre”.
English, Portuguese, and Spanish articles published between February 2008 and February 2018 were included. Articles were selected if meeting the following criteria: a) population: children within the age range of primary dental eruption; b) exposure: primary dental eruption; c) comparison: body temperature during a time period not associated with dental eruption; and d) outcome: fever in absence of systemic disease.
Studies were excluded if not meeting inclusion criteria, diverging from the study purpose, representing duplicates, or having been included in the MA or SR. The American Family Physician’s Strength of Recommendation Taxonomy (SORT) scale was used for rating the strength of the evidence retrieved.
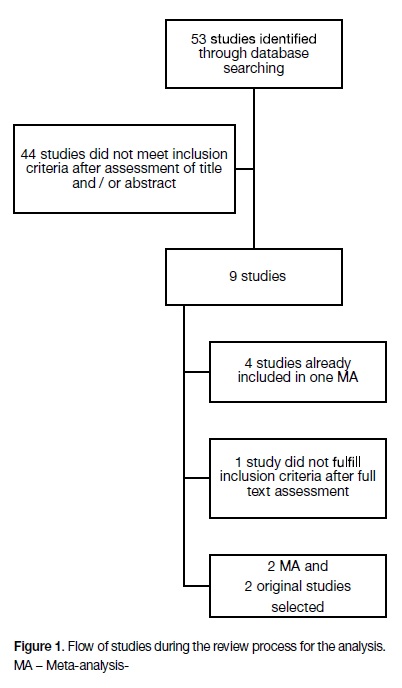
Results
The search strategy retrieved 53 articles, 49 of which were excluded from the analysis. Article selection process is depicted in Figure 1. Articles included consisted of two meta-analyses and two original studies, accounting for 5317 children in total (Tables 1 and 2).
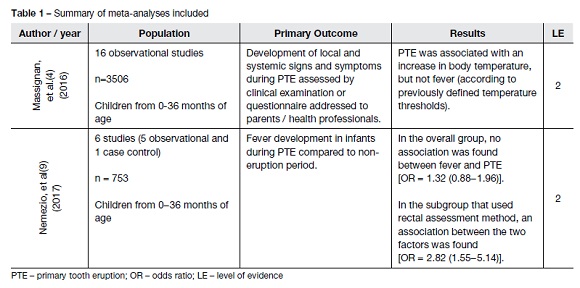
The meta-analysis by Massignan et al., published in 2016, aimed to evaluate the occurrence of local and systemic signs and symptoms during PTE in children from 0 to 36 months of age.4 This was achieved through clinical examination or through a questionnaire directed to parents or health professionals.
The analysis included 16 studies and a total of 3506 children, with several studies reporting a positive association between the two factors:
- One study found a mean rectal temperature of 37.6°C on the day of tooth eruption (DE) and ranging between 36.9−37.1ºC on days not associated with tooth eruption (DNAE);
- one study revealed only a minor temperature difference (36.18°C of tympanic temperature on DNAE and 36.21°C on DE);
- the other two studies (both with a moderate risk of bias) did not report mean DNAE or DE temperature, only mentioning a rectal temperature threshold of 37.7ºC and 37.5°C, respectively.
In fact, none of these studies reported temperature values higher than those previously defined as fever. In contrast, two other studies included in the meta-analysis (one being the most robust study included in the analysis) did not show an association between PTE and body temperature rise. The authors concluded that, although it is acceptable that PTE may be associated with an increase in body temperature, such cannot be characterized as fever. They also pointed out several limitations of studies included, such as the fact that many did not exclude for confounding factors (such as concomitant diseases), others were based on parental reporting of symptoms (memory bias), there was inconsistency in the definition of DE, and there was no clear description of diagnostic methods employed.
The 2017 meta-analysis by Nemezio et al. included six studies and 753 children and compared the onset of fever during PTE and during a time period not associated with dental eruption.9 Results from the total population revealed no association between fever and PTE. However, fever was more common during PTE in the subgroups where axillary, tympanic and, particularly, rectal assessment methods were used for temperature evaluation. In studies that did not report the assessment method used, no association was observed. Again, studies had a considerable heterogeneity regarding assessment measurement methods and who performed the assessments, and a clear risk of bias, with some studies not fully reporting inclusion and exclusion criteria.
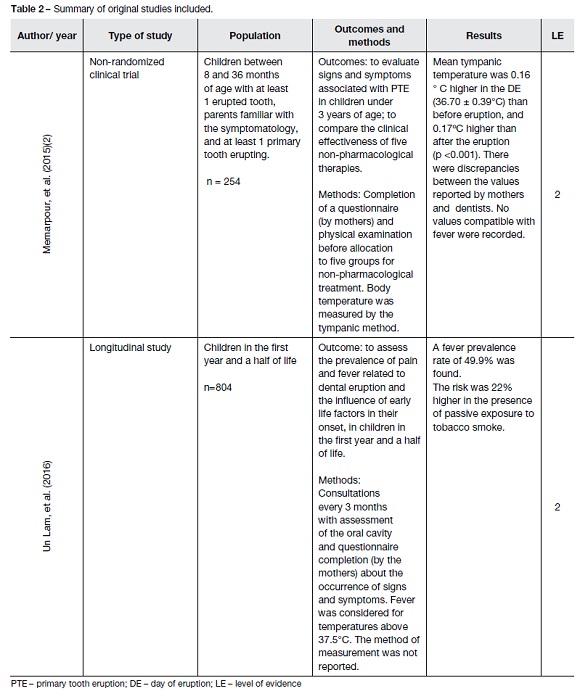
The clinical trial by Memarpour et al., from 2015, initially included 270 children aged 8 to 36 months, only 254 of whom completed the study. Children were selected and divided into groups and observed during an eight-day period during PTE. At each visit, data was retrieved through a questionnaire, an oral exam, and tympanic temperature assessment. The study found slight increases in body temperature only on DE (36.70 ± 0.39°C) compared with both previous and subsequent day of eruption (p<0.001 for both). There was no correlation between temperature values reported by mothers and researchers.
The study published by Um Lam et al. in 2016 assessed the prevalence of dental eruption-associated pain and fever and the influence of early life factors on their onset in children in their first year and a half of life. The study included 1033 children, but only 804 mother/children pairs were considered in the multivariable analysis. Children from three weeks to 1.5 years of age were observed every three months. During the medical appointment, an oral cavity examination was performed, and the presence of pain and fever was registered through questionnaires completed by mothers after proper training on how to make the observations. Body temperature above 37.5°C was considered as fever, but the temperature assessment method was not indicated. A fever prevalence rate of 49.9% was reported and the risk of fever was found to be 22% higher with passive exposure to maternal tobacco smoke. Mean temperature values were not reported.
Conclusions
Given limited available evidences and their inconsistent results, it is not possible to conclude the existence of an association between primary dental eruption and fever (SORT B). However, several studies have shown a slight increase in body temperature on the day of dental eruption.
The present review has several limitations, the most important being the lack of studies about the subject under investigation. Heterogeneity between available studies should also be taken into account, particularly regarding the temperature considered as defining fever, the temperature assessment method, and interpersonal variability in measurements. In some studies, assessment of body temperature was performed by health professionals, while in others it was carried out by the mother following completion of a questionnaire. Some studies have a significant risk of bias, since no clear definition of inclusion and exclusion criteria were used and some key information was missing, as the method used for temperature assessment - which necessarily impairs their external validity.
In conclusion, more studies are required to withdraw conclusions on this subject. These should include standard temperature limits for inferring fever, information on average temperature values retrieved, and, when applicable, a comparison of body temperature assessment methods and their accuracy.
Legends
DE day of the eruption
DeCS Descritores em Ciências da Saúde DNAE days not associated with eruption
LE Level of Evidence
MA Meta-analysis
MeSH Medical Subject Headings
PTE primary tooth eruption
RCTs randomized controlled trials
SORT Strength of Recommendation Taxonomy SR systematic reviews
REFERENCES
1. Olabu BO, Okoro DO, Thigiti JM, Oramisi VA. Impact of socio-cultural practice of infant/young child gum lancing during teething. J Clin Pediatr Dent. 2013; 37:355-9. [ Links ]
2. Memarpour M, Soltanimehr E, Eskandarian T. Signs and symptoms associated with primary tooth eruption: a clinical trial of nonpharmacological remedies. BMC Oral Health. 2015;15:88. [ Links ]
3. Haznedaroglu E, Mentes A. The Internet versus pediatricians as a source of infant teething information for parents in Turkey. Clinics. 2016. p. 430-4. [ Links ]
4. Massignan C, Cardoso M, Porporatti AL, Aydinoz S, Canto GDL, Mezzomo LAM, et al. Signs and Symptoms of Primary Tooth Eruption: A Meta-analysis. Pediatrics. 2016; 137:e20153501. [ Links ]
5. Kiran K, Swati T, Kamala BK, Jaiswal D. Prevalence of systemic and local disturbances in infants during primary teeth eruption: a clinical study. Eur J Paediatr Dent. 2011; 12:249-52. [ Links ]
6. Un Lam C, Hsu C-YS, Yee R, Koh D, Lee YS, Chong MF-F, et al. Early-life factors affect risk of pain and fever in infants during teething periods. Clin Oral Investig. 2016; 20:1861-70. [ Links ]
7. Ramos-Jorge J, Pordeus IA, Ramos-Jorge ML, Paiva SM. Prospective Longitudinal Study of Signs and Symptoms Associated With Primary Tooth Eruption. Pediatrics. 2011; 128:471-6. [ Links ]
8. Feldens CA, Faraco IMJ, Ottoni AB, Feldens EG, Vítolo MR. Teething symptoms in the first year of life and associated factors: a cohort study. J Clin Pediatr Dent. 2010; 34:201-6. [ Links ]
9. Nemezio MA, Oliveira KM De, Romualdo PC, Queiroz AM, Paula-e-Silva FW, Silva RA, et al. Association between Fever and Primary Tooth Eruption: A Systematic Review and Meta-analysis. Marwah N, editor. Int J Clin Pediatr Dent. 2017; 10:293-8. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Sara Matos
General and Family Practice,
Unidade de Saúde Familiar Navegantes
Avenida D. Manuel I, 360
4480-793 Vila do Conde
Email: smatos@arsnorte.min-saude.pt
Received for publication: 28.04.2018
Accepted in revised form: 08.10.2018

