










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.27 no.3 Porto set. 2018
https://doi.org/10.25753/BirthGrowthMJ.v27.i3.13329
QUAL O SEU DIAGNÓSTICO? | WHAT IS YOUR DIAGNOSIS?
Ophthalmology case
Caso oftalmológico
Alexandra FernandesI; Cristina MadureiraI; Fátima PintoII
I Department of Pediatrics, Centro Hospitalar Médio Ave. Unidade de Vila Nova de Famalicão. 4761-917 Vila Nova de Famalicão, Portugal. xana_ffernandes@hotmail.com; cristina_duarte9@hotmail.com
II General and Family Medicine, Unidade de Saúde Familiar Aníbal Cunha, Agrupamento de Centros de Saúde do Porto Ocidental. 4050-048 Porto, Portugal. fatymapynto@gmail.com
ABSTRACT
Brown syndrome is a rare ocular motility abnormality characterized by a restriction of the superior oblique tendon, which results in a restriction of elevation in adduction. This entity can be congenital or acquired. The cause of congenital Brown`s syndrome remains unknown but some cases with a family history have been described. Spontaneous resolution occurs between 20 to 30%. We describe a case of an eight-year-old boy with congenital Brown syndrome.
Keywords: Brown syndrome; ocular motility disorder; restriction of elevation in adduction
RESUMO
O síndrome de Brown é uma anormalidade rara da motilidade ocular caraterizada por restrição do músculo oblíquo superior, resultando em diminuição da elevação na adução. Esta entidade pode ser congénita ou adquirida. A causa do síndrome de Brown congénito permanece desconhecida, mas alguns casos de história familiar já foram descritos. A resolução espontânea ocorre entre 20 a 30%. Descrevemos o caso clínico de um rapaz de oito anos com síndrome congénito de Brown.
Palavras-chave: Distúrbio da motilidade ocular; restrição da elevação em adução; syndrome de Brown
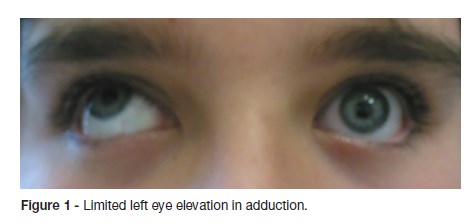
We describe a case of an eight-year-old boy presenting with limited elevation of the left eye in adduction. The parents had noticed the problem since early childhood with onset around three months of age. He had normal growth and psychomotor development. There was no history of previous traumatic events or systemic problems. His family history was unremarkable for any history of ophthalmologic diseases.
On ophthalmologic examination, the visual acuity of both eyes was 20/20 on the Snellen chart. The cover test didnt show any alteration. Examination revealed no significant refractive errors and fundal examination was normal in both eyes. Ocular motility showed an inability to elevate the left eye in adduction (Figure 1). His ocular examination was otherwise normal. A neurological evaluation, including magnetic resonance imaging of the brain was normal.
What is your diagnosis?
DIAGNOSIS
Congenital Brown syndrome of left eye
DISCUSSION
Brown syndrome is a rare ocular motility abnormality characterized by a restriction of the superior oblique tendon, which results in a restriction of elevation in adduction.1,2 The recognition of Browns syndrome can be accomplished by clinical examination and diagnosis confirmed with a positive forced duction test. When there is hypotropia ahead, the patient usually assumes an elective head position with elevation of the chin to maintain normal binocular vision.
Brown syndrome affects both males and females equally and usually only one eye.1-3 This syndrome may be present at birth or may occur as the result of another underlying disorder such as trauma or inflammation.4 In some cases it may be necessary to have an imaging examination for etiological clarification.
Congenital Brown syndrome is reported to be a restriction that is present at birth. There is no associated pain or inflammation. The cause of this disorder remains unknown but some cases with a family history have been described in literature.1-3 The limited upgaze in adduction seen in Congenital Brown syndrome is thought to be due to an abnormality of the trochlear tendon complex.
The main differential diagnoses are inferior oblique muscle hipoaction and double elevator palsy.
Spontaneous resolution occurs between 20 to 30%.4,5 This could be related to the natural growth of the child especially in those children whose eyes are normally aligned when looking straight ahead.4,5 Other cases of improvement could be related to the compensatory repetitive elevation of the eye induced by the contraction of the superior rectus muscle. Some authors advocate delaying the surgery until full orbital growth has occurred.4,5 In this case conservative management was decided because the patient did not have strabismus in the primary position or anomalous position of the head.
REFERENCES
1. Wright KW. Browns syndrome: diagnosis and management. Trans Am Ophthalmol Soc. 1999; 97:1023-109. [ Links ]
2. Attarzadeh A, Hoseinirad A, Rahat F. Brown syndrome in one pair of dizygotic twins: a case report. Cases J. 2010; 3:1 [ Links ]
3. Kenawy N, Pilz DT, Watts P. Familial unilateral Brown syndrome. Indian J Ophthalmol. 2008; 56:430-4. [ Links ]
4. Bansal S, Kumar N, Marsh I. Spontaneous resolution of congenital Brown`s Syndrome – a case report. Cases Journal. 2008;1:7 [ Links ]
5. Dawson E, Barry J, Lee J. Spontaneous resolutions in patients with congenital Brown syndrome. J AAPOS. 2012; 16:558-64. [ Links ]
CORRESPONDENCE TO
Alexandra Fernandes
Department of Pediatrics
Centro Hospitalar Médio Ave.
Unidade de Vila Nova de Famalicão
Rua Cupertino de Miranda s/n
4761-917 Vila Nova de Famalicão
Email: xana_ffernandes@hotmail.com
Received for publication: 18.10.2017
Accepted in revised form: 10.05.2018

