










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkNascer e Crescer
Print version ISSN 0872-0754On-line version ISSN 2183-9417
Nascer e Crescer vol.27 no.3 Porto Sept. 2018
https://doi.org/10.25753/BirthGrowthMJ.v27.i3.11983
ORIGINAL ARTICLES | ARTIGOS ORIGINAIS
Assessment of asthmatic child inhalation device technique
Avaliação da Técnica Inalatória em Idade Pediátrica
Pedro Tiago PintoI; Miguel JeriI; Telma BarbosaII
I Unidade de Saúde Familiar São João do Porto. 4050-377 Porto, Portugal. gomespinto.pedro@gmail.com; miguel.jeri.med@gmail.com
II Department of Pediatrics, Centro Materno Infantil do Norte, Centro Hospitalar do Porto. 4050-371 Porto, Portugal. telmab@gmail.com
ABSTRACT
Introduction: In Portugal, asthma is a very common disease, particularly in pediatric age, and many children are treated with medications delivered by inhalation devices. It is known that child inhaler technique is often throughout the world.
Aim: The aim of this paper is to describe the performance of asthmatic child device technique in a Portuguese children hospital in the city of Porto, (Centro Materno-Infantil do Norte - CMIN).
Methods: The authors assessed inhalation device technique of children aged 6 to 18 years, according to standardized checklists, (similar to those on the Aerosol Drug Management Improvement Team (ADMIT) Website) between September and October 2016, during follow-up of pediatric pneumology consultations in CMIN.
Results: Twenty one children met the inclusion criteria and 22 inhalation devices assessments were made. The majority (86%) used dry-powder inhalers; the most common error was failure to exhale before actuation (in 61%).
Discussion/Conclusion: Our results confirm a relatively high percentage of children failing in their performance in the use of the inhalation devices. Pediatricians and primary care physicians should assess the inhalation technique of asthmatic children regularly, in order to ensure a good asthma control in the pediatric age.
Keywords: Asthma; dry powder inhalers; metered dose inhalers
RESUMO
Introdução: Em Portugal a asma é uma doença muito comum, particularmente na idade pediátrica, e muitas crianças são tratadas com fármacos sob forma de dispositivos inalatórios. Sabe-se que a técnica inalatória é frequentemente feita de forma incorreta um pouco por todo o mundo.
Objetivo: O objetivo deste estudo foi o de avaliar a técnica inalatória de crianças num hospital pediátrico na cidade do Porto (Centro Materno-Infantil do Norte - CMIN).
Métodos: Os autores avaliaram a técnica inalatória de crianças dos 6 aos 18 anos de acordo com checklists standardizadas (semelhantes às descritas em Aerosol Drug Management Improvement Team (ADMIT) Website) entre setembro e outubro de 2016 durante consultas de seguimento de crianças em consulta de pneumologia pediátrica, no CMIN.
Resultados: Vinte e uma crianças possuíam os critérios de inclusão e foram realizadas 22 avaliações de dispositivos. A maioria das crianças usava um inalador de pó seco (86%), 61% destas não exalando o volume residual, previamente à inalação, sendo este o erro mais comum.
Discussão/Conclusão: Verificou-se uma alta percentagem de crianças com erros na sua técnica inalatória, sendo esses resultados concordantes com a literatura. Os pediatras e médicos de família devem avaliar regularmente a técnica inalatória da criança asmática, a fim de garantir um correto uso do dispositivo inalatório, contribuindo deste modo para o controlo da asma em idade pediátrica.
Palavras-chave: Asma; inaladores de dose calibrada; inaladores de pó seco
INTRODUCTION AND GOALS
In Portugal, asthma in children is a very common disease with an estimated national prevalence of 12.4%.1 Even though allergen eviction (like dust mites) is important, asthmatic children are usually treated with medications delivered by inhalation devices. Younger children should use a pressurized metered-dose inhaler with a spacer to overcome hand-lung poor coordination, whereas older children, with a good inspiratory capacity, should use a dry powder inhaler device.2,3
It is well known that child inhaler technique is usually incorrectly performed throughout the world, and that different devices have different rates of optimal technique.4 Inadequate inhalation technique can result in decreased asthma control, less quality of life and high burden of costs.5 Evidence also shows that teaching children the proper use of inhalers during every consultation is an effective measure to correct technique.4
Although both caregivers and children are the mainstream of treatment, general practitioners and pediatricians should have an important role providing children assessment of their inhaler technique and correct them when errors are detected at every opportunity, which is essential for good asthma control.6-8
This paper describes the performance of asthmatic child device technique in a Portuguese children hospital.
METHODS AND MATERIALS
Inhalation device technique was assessed during September and October 2016 during follow-up of pediatric pneumology consultations.
The subjects eligible for this study were asthmatic children aged 6 to 18 years, on daily inhaling medication.
Informed consent was obtained from all included children and their parents.
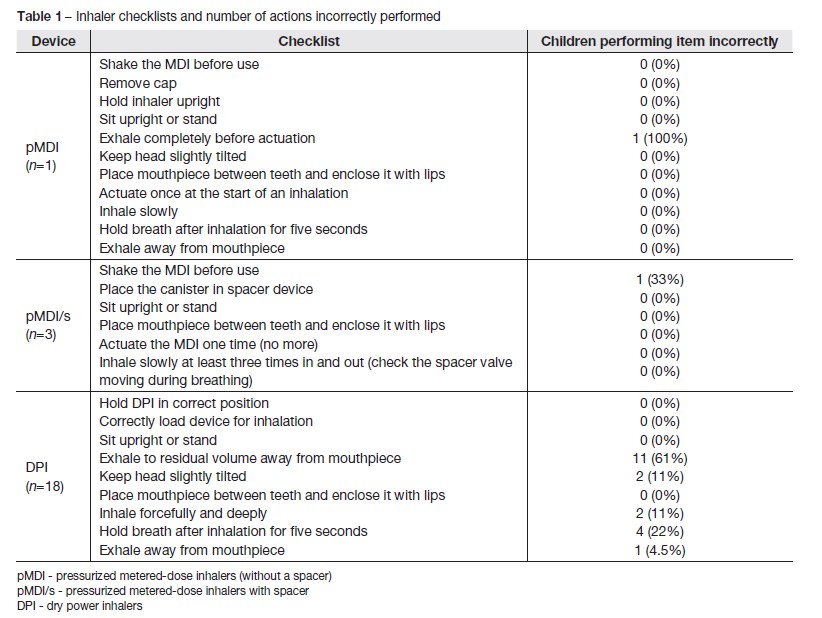
Inhalation technique was evaluated once using standardized checklists similar to those on the Aerosol Drug Management Improvement Team (ADMIT) Website (Table 1).9
The study was observational; no instructions were given prior to the assessment.
Asthma control was evaluated according to Global Initiative for Asthma (GINA) 2015 Guidelines (In the past four weeks, the patient had: 1- Daytime symptoms more than twice/week? Yes/No; 2- Any night waking due to asthma? Yes/No; 3- Reliever needed more than twice/week? Yes/No; 4-Any activity limitation due to asthma? Yes/No. If none of these: well controlled; If 1-2 of these: partly controlled; If 3-4 of these: uncontrolled).10
The authors considered three categories of inhalers: dry powder inhalers (DPI) and pressurized metered-dose inhalers with and without a spacer device (pMDI/s and pMDI, respectively).
It was considered that a correct technique had all steps performed with no errors, and an incorrect technique had at least one incorrect step.
In univariate analysis, the authors related inhalation technique to age, gender duration of asthma, asthma control, read-information about asthma, existence of a written plan and supervision of a caregiver.
Data-analysis was performed with SPSS for Windows (v 12.2) (SPSS, Inc.).
RESULTS
Twenty-one children met the inclusion criteria (43% female; mean age 12.2 years) and twenty-two devices were assessed according to the checklists (Table 1). Devices used were:
- DPI: Turbuhaler (n=13), Novolizer (n=3), Diskus (n=2)
- pMDI/s (n=3)
- pMDI (n=1)
The patient using pMDI was 16 years old.
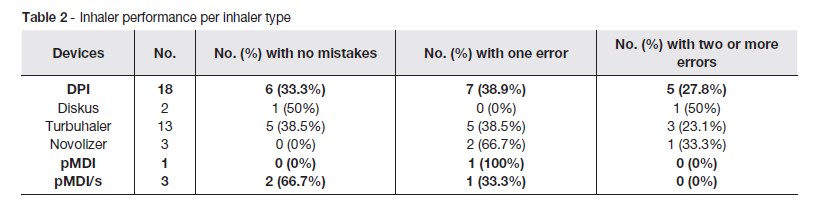
Of the 22 device assessments, only 36% (n=8) had no errors in the performance. The most common error in the DPI devices was not exhaling to residual volume before inhaling the asthma medication (61%). Four of the patients 18 (22%) forgot to hold breath after inhalation for five seconds.
Of the four pMDI assessments, three (75%) used it with a spacer device with a mask; only those had a family surveillance during technique. In one of these cases, the shaking prior to use was forgotten by the caregiver (Table 2).
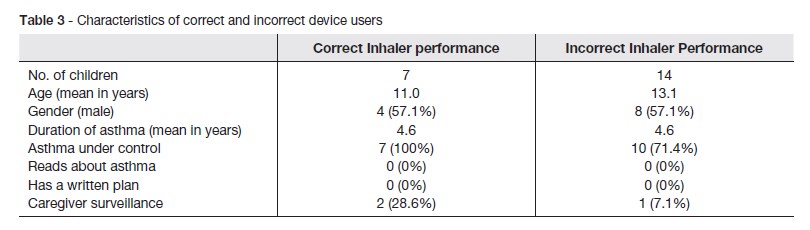
In Table 3 the authors compared the correct (all steps correct) and incorrect (at least one step incorrect) performances with some features of children whose technique was assessed.
According to these results, the mean age of an incorrect inhaler performance is higher than those who perform with no mistakes. Although we couldnt find statistical significance (p=0.145, Mann-Whitney U test), the results point a higher probability of an incorrect inhaler technique among older children.
According to gender and asthma duration, there are no differences in the percentage of children who performed the technique correct or incorrectly.
In the assessments made, all children who didnt have their asthma under control (uncontrolled (n=2) or partially controlled (n=2)) had incorrect performances.
None of the children usually read asthma information neither follow a written plan for inhaler performance.
Only three children had adult supervision, all of them using pMDI/s.
DISCUSSION/CONCLUSION
The authors assessed the inhalation technique of asthmatic children aged between 6-18 years. There was a relative high percentage of children failing in their performance, findings similar to what scientific evidence reports.4,10 Results support the idea that health providers should assess childrens inhalation technique on every consultation. Although the results are in compliance with literature, they differ regarding duration of asthma: Have et al. found that children with asthma diagnosis for a longer time had more errors in the performance.10
A limitation of this study is the small number of assessments, due to the short period of data collection imposed by mandatory schedule issues. Another limitation is the fact that inhalation technique performance during the assessment might not mimic the performance at home. However it is doubtful that they can do it better at home, because it isnt expected that they pay as much attention to their performance as in the assessment.
Although they were given a plan with instructions on how to use the inhaler at the time of the prescription, most of them didnt follow it.
Pediatricians and primary care physicians should assess the inhalation technique of all asthmatic children who were prescribed an inhaler in order to guarantee its correct use, which is essential for a good asthma control in the pediatric age.
Furthermore, caregivers should also be able to manage the device and supervise the children technique in every consultation and not only in the beginning of treatment. This strategy will, no doubt improve the efficacy of the drug administration.
REFERENCES
1. Sá-Sousa A, Azevedo LF, Carvalho R, Jacinto T, Todo-Bom A, Loureiro C, et al. Prevalence of asthma in Portugal - The Portuguese National Asthma Survey. Clin Transl Allergy. 2012; 2:15. [ Links ]
2. Devadason SG. Recent advances in aerossol therapy for children with asthma. J Aerosol Med. 2006; 19:61-6. [ Links ]
3. Bindels PJ, vand der Wouden JC, Ponsioen BP, Brand PL, Salome PL, Van Hensbergen W, et al. NHG-Standaard Astma Bij Kinderen. Juisarts Wet 2006; 49:557-72. [ Links ]
4. Gillete C, Rockich-Winston N, Kuhn JA, Flesher S, Shepherd M. INhaler Technique in Children with Asthma: A Systematic Review. Acad Pediatr. 2016; 16:605-15. [ Links ]
5. Kwok PCL, Chan HK. Delivery of inhalation drugs to children for asthma and other respiratory disease. Adv Drug Deliv Ver. 2014; 83: 83-8. [ Links ]
6. National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma. National Institutes of Health. August, 2007. (Accessed November 5, 2016). Available at: http://www.nhlbi.nih.gov/files/docs/guidelines/asthgdln.pdf. [ Links ]
7. Sleath B, Ayala G, Gillette C, Williams D, Davis S, Tudor G, et al, Provider Demonstration and Assessment of Child Device Technique During Pediatric Asthma Visits, Pediatrics. 2011; 127:642-8. [ Links ]
8. ADMIT Website (http://www.admit-online.info/en/). [ Links ]
9. Global Initiative for Asthma. Pocket guide for Asthma management and prevention (for Adults and Children older than 5 years). 2015. Available at: https://ginasthma.org/archived-reports/. [ Links ]
10. Have W, Berg N, Bindels P, Aalderen W, Palen J. Assessment of Inhalation Technique in Children in General Practice: Increased Risk of Incorrect Performance with New Device. Journal of Asthma. 2008; 45:67-71. [ Links ]
CORRESPONDENCE TO
Pedro Tiago Pinto
Unidade de Saúde Familiar
São João do Porto
Rua Miguel Bombarda, 234
4050-377 Porto
Email: gomespinto.pedro@gmail.com
Received for publication: 08.05.2017
Accepted in revised form: 13.07.2018


{kind=link}
{kind=link}
{kind=link}