










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkNascer e Crescer
Print version ISSN 0872-0754On-line version ISSN 2183-9417
Nascer e Crescer vol.27 no.2 Porto June 2018
ARTIGOS ORIGINAIS | ORIGINAL ARTICLES
Self-Concept and Disturbed Eating Behavior in a Clinical Population of Adolescents with Eating Disorders
Autoconceito e Comportamento Alimentar Perturbado numa População Clínica de Adolescentes com Perturbação do Comportamento Alimentar
David MoreiraI; Joana SaraivaI
I Department of Child and Adolescent Psychiatry, Centro Hospitalar do Porto. 4099-001 Porto, Portugal. dnomoreira@hotmail.com; joana.saraiva@chporto.min-saude.pt
ABSTRACT
Introduction: Changes in self-concept have been considered to play a crucial role in the etiology of eating disorders. In this study, we evaluate the levels of self-concept and severity of the disturbed eating behavior in a clinical population of adolescents with Eating Disorders (ED) and study their correlations.
Method: A sample of 50 patients of an Adolescent Psychiatric Service completed two validated self-report scales: the Piers-Harris Childrens Self-concept Scale (PHCSCS) and the Eating Disorder Examination - Questionnaire (EDE-Q). Anthropometric data were also collected.
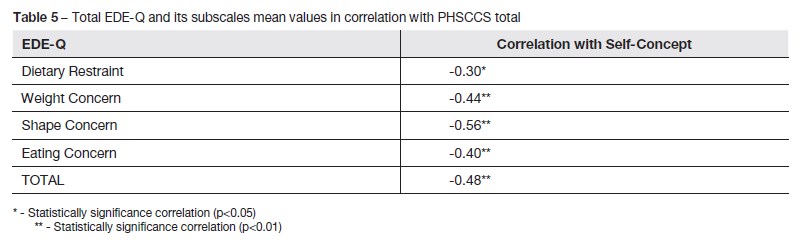
Results: Total self-concept had a negative correlation with disease severity [total EDE-Q (rs= -0.48)], as well as with four subscales of the EDE-Q [Dietary Restraint (rs =-0.30); Weight Concern (rs=-0.44); Shape Concern (rs=-0.56); and Eating Concern (rs=-0.40)]. Four of the PHCSCS subscales showed a negative correlation with the severity of the disease [Behavioral Adjustment (rs=-0.39); Freedom from Anxiety (rs=-0.56); Popularity (PO) (rs=-0.43) and Happiness and Satisfactions (HS) (rs=-0.39)]. Then the sample was divided into two groups: Compulsive / Purgative [5 Bulimia Nervosa (BN) + 3 Unspecified Feeding and Eating Disorder (UFED) with insufficient criteria for BN] and Restrictive (38 Anorexia Nervosa + 4 UFED with insufficient criteria for AN). The Compulsive / Purgative group had lower Self-concept than the Restrictive group (p <0.05). This first group also presented lower values than the Restrictive group in all subscales of the PHCSCS, but with statistical significance only in the Intellectual and School Status and HS. It also presented higher disease severity (p <0.05), with higher values in all four EDE-Q subscales, but with statistical significance only in Weight Concern (p <0.05).
Conclusions: These results are in agreement with the literature that the Self-concept is altered in ED. In our study, we report an inverse correlation between self-concept and dysfunctional eating behaviors. The Compulsive/Purgative group reported a lower self-concept and greater severity of the eating behavior pathology, but there were no clinical differences between the two groups. This finding may be explained by the lower morbidity awareness of the Restrictive group.
Keywords: Adolescents; Anorexia Nervosa; Bulimia Nervosa; Self-concept
RESUMO
Introdução: Alterações no autoconceito têm sido consideradas como tendo um papel crucial na etiologia das perturbações do comportamento alimentar (PCA). Neste estudo, avaliámos os níveis de autoconceito e severidade do comportamento alimentar perturbado numa população clínica de adolescentes com perturbações do comportamento alimentar e estudamos suas correlações.
Métodos: Uma amostra (n = 50) de pacientes dum Serviço de Psiquiatria da Adolescência preencheu duas escalas de auto-relato validadas: a Piers-Harris Children´s Self-concept Scale (PHCSCS) e o Eating Disorder Examination – Questionnaire (EDE-Q). Os dados antropométricos também foram recolhidos.
Resultados: O autoconceito total teve uma correlação negativa com a gravidade da doença [EDE-Q total (rs= -0,48)], bem como com as quatro subescalas da EDE-Q [Restrição (rs= -0,30); Preocupação com o Peso (rs= -0,44); Preocupação com a forma (rs= -0,56); e Preocupação com a Comida (rs= -0,40)]. Quatro das subescalas PHCSCS mostraram correlação negativa com a gravidade da doença [Aspeto Comportamental (rs= -0,39); Ansiedade (rs= -0,56); Popularidade (rs= -0,43) e Satisfação e Felicidade (SF) (rs= -0,39)]. Em seguida, a amostra foi dividida em dois grupos: Compulsivo / Purgativo [5 Bulimia Nervosa (BN) + 3 Perturbação da Alimentação e da Ingestão Não Especificada (PAINE) com critérios insuficientes para BN] e Restritivo (38 Anorexia Nervosa + 4 PAINE com critérios insuficientes para AN). O grupo Compulsivo / Purgativo apresentou menor Autoconceito do que o grupo Restritivo (p <0,05). Este primeiro grupo apresentou também valores mais baixos do que o grupo Restritivo em todas as subescalas do PHCSCS, mas com significância estatística somente no Estatuto Intelectual e SF. Também apresentou maior gravidade da doença (p <0,05), com valores mais altos nas quatro subescalas do EDE-Q, mas com significância estatística somente em Preocupação com o Peso (p <0,05).
Conclusões: Estes resultados estão de acordo com a literatura de que o autoconceito está alterado na PCA. No nosso estudo, relatamos uma relação inversa entre o autoconceito e os comportamentos alimentares disfuncionais. O grupo Compulsivo/Purgativo relatou um autoconceito inferior e uma maior gravidade da patologia do comportamento alimentar, mas não houve diferenças clínicas entre os dois grupos. Esse achado pode ser explicado pela menor consciência mórbida do grupo Restritivo.
Palavras-chave: Adolescentes; anorexia nervosa; autoconceito; bulimia nervosa
INTRODUCTION
Self-concept refers to the image each one has of himself, his thoughts, feelings and characteristics of each ones identity. Self-concept gives subjectivity to experiences and influences the way people behave and interpret personal, interpersonal and social realities.1 In this sense, the evaluation of self-concept is of particular importance in the understanding of the adolescent.
Eating disorders (ED), currently categorized in DSM-5 as Feeding and Eating Disorders (FED), include different but overlapping syndromes, characterized by abnormal eating behaviors and concerns with body image. These include Anorexia Nervosa (AN), Bulimia Nervosa (BN), Binge Eating Disorder and Unspecified Feeding or Eating Disorder (UFED), among others.2
Although many important differences have been identified between AN and BN, changes in self-concept have been considered to play a crucial role in the etiology in both disorders.3,4 A low or negative self-concept assumes a central role in many etiological theories of eating disorders. Deficits in self-concept in these patients are considered central symptoms and necessary criteria for the diagnosis: ...undue influence of body weight and shape on self-evaluation....2 In the field of ED, the concepts of self-esteem, ineffectiveness, and negative self-evaluation have been examined in a large number of cross-sectional studies.5 Patients with AN and BN exhibit lower self-esteem or a more negative self-concept than healthy control groups.3 One of the consequences of this sense of personal ineffectiveness and powerlessness is that the individual might attempt to gain some degree of personal power and control by rigid control of his eating behaviors.6
With this relation in mind, we hypothesize that adolescents in a more severe stage of the disease will have lower self-concept.
In this study we propose to characterize the self-concept and severity of the disease of a clinical population of adolescents with FED and study their correlations.
METHODS
Population under study
Adolescents who attend the Eating Disorders Inpatient and Outpatient Clinic at the Child and Adolescent Psychiatry Adolescent Service in Centro Hospital do Porto, aged between 12 and 18 years, were asked to participate in the study willingly. Inclusion criteria were a DSM-5 diagnosis of FED in any stage of disease, as necessary to attend this Eating Disorders Outpatient Clinic, other than Pica, Rumination Disorder, Avoidant/Restrictive Food Intake Disorder and Binge Eating Disorder. Patients were excluded if they had intellectual disability, however none of the adolescents recruited did so.
The data was collected through international self-report questionnaires: the Piers-Harris Childrens Self-Concept Scale (PHCSCS) and the Eating Disorder Examination - Questionnaire (EDE-Q), both validated for the Portuguese population.7,8 In clinical or research context, self-evaluation scales are the most used techniques to evaluate self-concept.9 Anthropometric data were collected (weight and height with BMI and weight percentile calculation).
Scales used description
The Piers-Harris Childrens Self-Concept Scale (PHCSCS) is a self-concept assessment tool. The scale consists of 60 items, in its short form version, which is divided into six factors: behavioral adjustment (BA), intellectual and school status (IS), physical appearance and attributes (PA), freedom from anxiety (AN), popularity (PO) and happiness and satisfactions (HS). A higher score on any subscale means a better self-concept.
The Eating Disorder Examination Questionnaire (EDE-Q) is the self-reported version of the Eating Disorders Examination Interview.10 It consists of 33 items and contains 4 subscales: Dietary Restraint, Eating Concern, Weight Concern, and Shape Concern.11 A higher value means greater severity of dysfunctional eating behavior and a value >4 means pathologic eating behavior.
The entire study was conducted between 2013 and 2016 and authorized by the Ethics Committee of Centro Hospitalar do Porto.
Data analysis
All subjects were included in the data set. Demographics were evaluated with descriptive statistics and inferential statistical analysis. Differences between groups and correlations were tested using non-parametric tests (Mann-Whitney test and Spearman test, respectively), due to the non-normal distribution of the sample. T-tests were used when the variable had a normal distribution. Results are presented in mean (standard deviation - SD). Differences were interpreted at the 5% significance level (2-tailed).
RESULTS
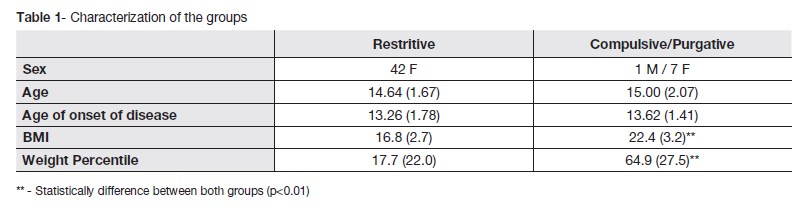
A total of 50 adolescents accepted to fill the questionnaires (1 male and 49 females), with a mean age 14.7 years (SD = 1.8). Age of disease onset was 13.3 years (+-1.7).
The sample was divided into two groups according with diagnostic characteristics: Restrictive type (38 Anorexia Nervosa (AN) + 4 UFED with insufficient criteria for AN) and Compulsive / Purgative type (5 Bulimia Nervosa (BN) + 3 Unspecified Feeding and Eating Disorder with insufficient criteria for BN).
These groups didnt differ in age or age of disease onset. Differences were found in BMI (t-test p<0.01) and weight percentile (Mann-Whitney p<0.01). Table 1 describes groups characteristics.
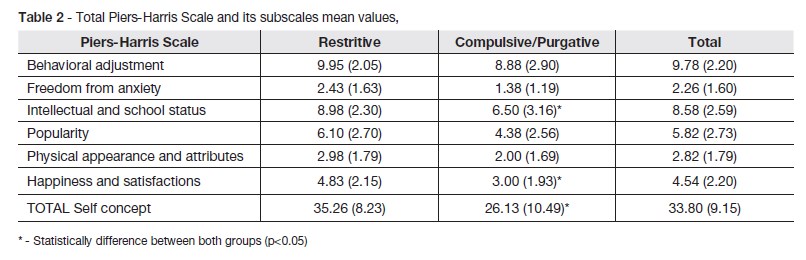
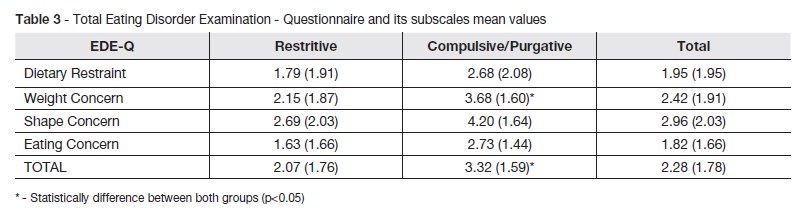
The mean results for the utilized scales for both groups and the total sample are exposed on table 2 and table 3.
The Compulsive / Purgative group had lower Self-concept than the Restrictive group (p<0.05). This first group also presented inferior results in relation to the Restrictive group in all subscales of the PHCSCS, but with statistical significance only in the Intellectual and School Status and HS.
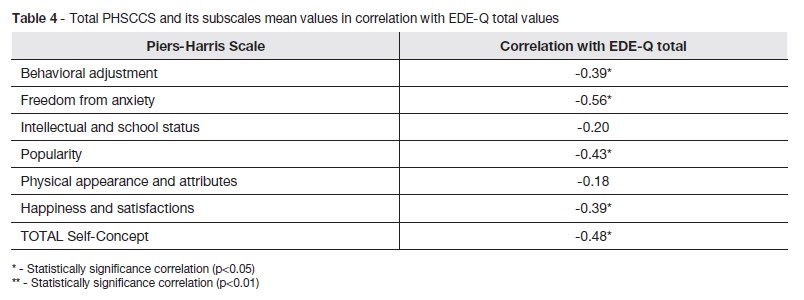
The Compulsive/Purgative group presented higher disease severity (p<0.05), with higher values in all four EDE-Q subscales, but with statistical significance only in Weight Concern (p<0.05). The correlations values between scale values are exposed on table 4 and table 5.
Self-concept had a moderate negative correlation with disease severity (p<0.05). Four of the PHCSCS subscales (BA, AN, PO and HS) showed a negative correlation with the severity of the disease.
Self-concept had moderate negative correlation with EDE-Q all four subscales (p<0.01).
DISCUSSION
There were two important findings in this study. First, there is a statistically significant association between levels of self-concept and dysfunctional eating behaviors. A low self-concept may be at the origin of dysfunctional behaviors and these may be used as an illusory tool to increase it, creating a self-perpetuating pattern of pathologic eating behavior. Higher values of self-concept may be protective against the onset of eating disorders and promote a positive assessment of the body that will attenuate events that threaten body image.12
The fact that EDE-Q and all its subscales had a highly significant statistic relation with total self-concept confirms the pathological importance of eating behavior in the self-concept of these patients.
Second, self-concept can be low for different reasons in different eating disorders. When we compare the two groups: Restrictive and Compulsive/Purgative, we find higher values of total self-concept and Intellectual Status in the first group. As it is known, these young people with restrictive anorectic behavior tend to be perfectionistic and invest heavily in their studies, as these are a way of valuing themselves, therefore maintaining a high Intellectual status.13 The Compulsive/Purgative group shows lower levels of self-concept probably due to dissatisfaction with their lower self-control ability and failure to achieve their goal of reducing weight. It is described that this group also has more mood variations (depression and low self-esteem are highly correlated), coinciding with the inferior result in the Satisfaction and Happiness subscale.14
The Restrictive group also had lower levels in the EDE-Q (less self-reported dysfunctional eating behaviors) that can be explained by a poor morbid awareness, disease negation, more egosynthonic symptoms and more difficulty identifying them as intrusive, and the need to please (reinforced by the questionnaires being self-report and of subjective and personal evaluation of their image and illness). Thus, this group appears to have less psychopathology than the Compulsive/Purgative, but this is not confirmed by clinical and anthropometric data. The Compulsive/Purgative group having higher Weight Concern can be explained by its higher BMI.
There are some limitations to our study, including absence of a healthy control group, a small sample of the Compulsive/Purgative group and no objective evaluation of depressive symptoms, which interferes with self-concept, or other comorbilities other than clinical observation.
CONCLUSIONS
These results are in agreement with the literature that Self-concept is altered in Eating disorders. In our study, we report an inverse correlation between self-concept and dysfunctional eating behaviors. However, different ED show different presentations of low self-concept and further studies should focus on these different groups and investigate the reasons behind this finding. A low self-concept seems to be causative of dysfunctional eating behaviors and can be a potential therapeutic target to avoid the development of such behavior. Self-concept should then be evaluated in recovered patients and identify its role on recovery. Mood alterations on Compulsive/Purgative patients should also be addressed. To our knowledge this original contribution is the first characterization of self-concept of patients with ED in a Portuguese clinical adolescent psychiatry setting.
REFERENCES
1. Baumeister RF. Identity, self-concept, and self-esteem. In: Hogan R, Johnson JA, Briggs SR, editors. Handbook of Personality Psychology. Academic Press; 1997. p. 681-711. [ Links ]
2. American Psychiatric Association. American Psychiatric Association. DSM-5 Task Force. : Diagnostic and statistical manual of mental disorders : DSM-5. 5th ed. Washington D.C: American Psychiatric Association; 2013. [ Links ]
3. Jacobi C, Paul T, de Zwaan M, Nutzinger DO, Dahme B. Specificity of self-concept disturbances in eating disorders. Int J Eat Disord. 2004; 35:204-10. [ Links ]
4. Stein KF. The self-schema model: a theoretical approach to the self-concept in eating disorders. Arch Psychiatr Nurs, 1996; 10:96-109. [ Links ]
5. Jacobi C. Self-concept disturbances in patients with eating disorders. Zeitschrift für Klinische Psychologie-Forschung und praxis. 2000; 29:75-96. [ Links ]
6. Guidano VF, Liotti G. Cognitive processes and emotional disorders : a structural approach to psychotherapy. The Guilford clinical psychology and psychotherapy series. New York: Guilford Press; 1983. [ Links ]
7. Veiga FH. Escala de autoconceito: adaptação portuguesa do Piers-Harris Childrens Self-Concept Scale. Psicologia. 1989. 7: 275-84. [ Links ]
8. Machado PP, Martins C, Vaz AR, Conceição E, Bastos AP, Gonçalves S. Eating disorder examination questionnaire: psychometric properties and norms for the Portuguese population. Eur Eat Disord Rev. 2014; 22:448-53. [ Links ]
9. Butler RJ, Gasson SL. Self Esteem/Self Concept Scales for Children and Adolescents: A Review. Child and Adolescent Mental Health. 2005. 10:190-201. [ Links ]
10. Cooper Z, Fairburn C. The Eating Disorder Examination: a semi-structured interview for the assessment of the specific psychopathology of eating disorders. Int J Eat Disord. 1987; 6:1-8. [ Links ]
11. Tury F, Gulec H, Kohls E. Assessment methods for eating disorders and body image disorders. J Psychosom Res. 2010. 69:601-11. [ Links ]
12. Stein KF, Corte C. Identity impairment and the eating disorders: content and organization of the self-concept in women with anorexia nervosa and bulimia nervosa. European Eating Disorders Review. 2007; 15: 58-69. [ Links ]
13. Halmi KA, Sunday SR, Strober M, Kaplan A, Woodside DB, Fichter M, et al., Perfectionism in anorexia nervosa: variation by clinical subtype, obsessionality, and pathological eating behavior. Am J Psychiatry. 2000;157:1799-805. [ Links ]
14. Bernet CZ, Ingham RE, Johnson BR. Self-esteem. IN: Costello CG, editor. Symptoms of Depression. New York: Wiley; 1993. p. 141-59. [ Links ]
CORRESPONDENCE TO
David Moreira
Department of Child and Adolescent Psychiatry
Centro Hospitalar do Porto
Largo Professor Abel Salazar
4099-001 Porto
Email: dnomoreira@hotmail.com
Received for publication: 27.09.2017
Accepted in revised form: 14.12.2017


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}