










Serviços Personalizados
Journal
Artigo
 Português (pdf)
Português (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.26 no.3 Porto set. 2017
CASE REPORTS | CASOS CLÍNICOS
Unilateral renal agenesis and uterine anomalies: how and when can we make this diagnosis?
Agenesia renal unilateral e anomalias uterinas: como e quando devemos fazer o diagnóstico?
Joana GasparI,II; Natália FerreiraIII; Luísa LoboIII; Carla SimãoI
I Department of Pediatrics, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte; Centro Académico Clínico. 1649-035 Lisboa, Portugal. joanagaspar@ymail.com; carla.mail@netcabo.pt
II Department of Pediatrics, Hospital do Espírito Santo Évora. 7000-811 Évora, Portugal. joanagaspar@ymail.com
III Radiology Department, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte; Centro Académico Clínico. 1649-035 Lisboa, Portugal. nataliasanferreira@hotmail.com; mluisalobo@gmail.com
RESUMO
Adolescente de 12 anos de idade com diagnóstico pré-natal de agenesia renal esquerda, foi internada com uma história de quatro meses de evolução de dor abdominal recorrente e dismenorreia após a menarca. A investigação imagiológica revelou uma malformação uterina associada a defeitos de desenvolvimento do canal de Muller – útero duplicado com hemi-utero esquerdo obstruído e com conteúdo hemático (hematometra), um colo uterino único e uma vagina normal. Pretendemos alertar para a associação entre agenesia renal unilateral e malforma ções ginecológicas, a maioria uterinas, mas também vaginais. A sua detecção precoce por métodos imagiológicos permite antecipar medidas terapêuticas para alívio sintomático, sobretudo dor abdominal ou pélvica recorrente, bem como evitar as complicações associadas (endometriose, aderências pélvicas ou infecções).
Palavras-chave: Agenesia renal; malformações uterinas; pediatria
ABSTRACT
A 12-year-old female with a prenatal diagnosis of left kidney agenesis was hospitalized with a history of four months of recurrent abdominal pain and dysmenorrhea after menarche. Imaging investigation revealed a gynecological malformation associated with Müllerian developmental defects – duplicated uterus with an obstructed left hemi-uterus filled with hematic content (haematometra), one cervix and a normal vagina. We pretend to alert pediatric physicians about the association of renal agenesis and gynecological malformations, most frequently uterine, but also vaginal. Early detection of these malformations by imaging will anticipate therapeutic measures to relieve symptoms, mostly recurrent abdominal or pelvic pain, and to avoid complications such as endometriosis, pelvic adherences and infections.
Keywords: Pediatrics; renal agenesis; uterine anomalies
INTRODUCTION
Congenital unilateral renal agenesis occurs in approximately 1:1300 births and is probably underestimated due to its common asymptomatic course.1 It is frequently associated with other abnormalities, including isolated or syndromatic anomalies of the cardiovascular, skeletal, central nervous and urogenital systems. These include Müllerian duct anomalies (MDA) resulting in uterine and/or vaginal defects at the same side of the absent kidney.1 MDA duct anomalies are rarely diagnosed prenatally. The neonatal period is an excellent opportunity to detect gynecologic malformations due to the physiologic enlargement of the uterus influenced by maternal and placental hormones.2 Thereafter, uterine malformations can go undetectable until puberty. Clinical manifestations often start during adolescence, with the onset of menarche, presenting with cyclic pelvic pain caused by an obstructed structure, with or without menstrual abnormalities.3 Additional complications include recurrent infections, pelvic adherences and endometriosis.3
The diagnosis of unilateral renal agenesis must alert the physician to look for associated genital anomalies, ideally during neonatal period or at peri-pubertal age, avoiding complications or even unnecessary emergent surgery in patients with abdominal or pelvic pain that might be confused with other causes of acute pelvic pain.
CASE REPORT
A 12-year-old female, with a prenatal diagnosis of left kidney agenesis, started recurrent abdominal pain and dysmenorrhea after menarche.
Family history was negative for renal or urinary defects.
Her gestation was a full term pregnancy, the first of her mother. At 24 weeks, a prenatal diagnosis of left kidney agenesis was done by fetal ultrasound (US). The newborn was light for gestational age (2495g), but otherwise clinically well. She had an uneventful perinatal period.
She was referred to our pediatric nephrology clinic at the age of eight months. US revealed a single right kidney with compensatory hypertrophy with mild pelvicalyceal dilation. Radiological cystography was negative for vesicoureteral reflux; renal scintigraphy showed a single right kidney with no lesions; DTPA-renogram showed a good kidney function and a normal excretion pattern.
During the first years of life she had several urinary infections, with no renal scar formation. She maintained a normal glomerular filtration rate, and microalbuminuria was first detected by the age of nine. No hypertension was found during follow-up.
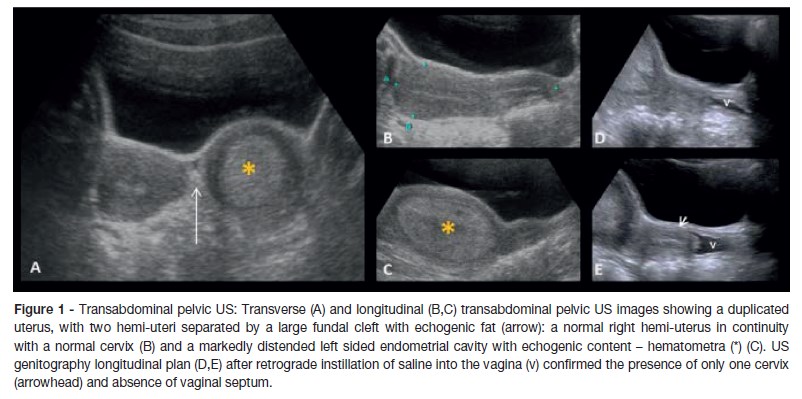
By the 12 years of age, coincident with menarche, she started recurrent abdominal pain and continuous menstrual bleeding. She was observed by gynecologist and started on a contraceptive pill (ethinylestradiol and gestodeno) without improvement. She was admitted four months later with severe abdominal pain, especially in the lower quadrants without fever, vomiting, diarrhea or urinary symptoms. On physical examination vital signs were normal, and there was no palpable abdominal mass. Analytic assessment (blood count, renal function and urine analysis) was normal. Transabdominal pelvic US (fig.1 A-C) revealed two divergent hemi-uteri, one single cervix and a non-septate vagina. The right hemi-uterus was normal, and in continuity with the cervix and vagina. The left hemi-uterus had normal size but its endometrial cavity was obstructed and filled with echogenic fluid (haematometra). At the level of the istmus, the left-sided uterus was in close connection with the right-sided uterus, although a normal cervix could not be detected. The ovaries were normal in size and shape. Even after US genitography performed during retrograde instillation of saline into the vagina (fig.1 D, E), it was difficult to assure the exact level of obstruction. For further anatomic delineation, a pelvic magnetic resonance imaging (MRI) was performed (fig.2), revealing two normal-sized divergent hemi-uteri with non-communicating endometrial cavities and a preserved myometrial width in both uterine horns. The right hemi-uterus showed a normal size and morphology in continuity with one apparent normal cervix. The left hemi-uterus was obstructed at the level of the istmus with haematometra. No evidence of vaginal duplication was seen. According to these findings, the girl had a left renal agenesis and an associated MDA probably an anatomic variant of didelphys uterus with left cervical atresia and a normal vagina.
Surgery has been considered the most appropriate treatment, and is planned to be performed soon.
DISCUSSION
In unilateral renal agenesis, the embryonic insult that occurs in the ureteral bud may also affect the Wollfian duct in males and the Müllerian duct in females. From an embryologic perspective, the Müllerian system defects can result from agenesis of structures, vertical fusion defects and lateral fusion defects, which can occur isolated or combined in more complex malformations. Lateral fusion defects are the most common MDA and also more often associated with renal abnormalities. MDA are usually categorized according the American Fertility Society classification.3,4
Despite undoubtful usefulness of this grading system in clinical practice, there are some cases that may be difficult to classify, particularly when lateral fusion defects are associated with partial agenesis of structures, like in our patients case.
The above mentioned classification, divides uterine defects in septate uterus (one uterus with endometrial cavity divided by a total or partial septum), unicornuate uterus (normal hemiuterus, fallopian tube and cervix in one side, and abnormal structures on the other side – mostly a rudimentary horn, which may not communicate with the uterus); bicornuate uterus (one uterus with an indented fundus, having various separation degrees of the uterine horns) and didelphys uterus (duplication of the reproductive structures – two uterus and two cervix, often associated with vaginal septum double vagina).3-6
Almost all of these defects can result in some degree of obstruction, particularly if associated with partial agenesis of structures or with a transverse vaginal septum, causing pain after the onset of menarche when the endometrial cavities shed.6 Nevertheless, some defects may be asymptomatic and diagnosed in later in life, during investigation of infertility or recurrent miscarriage.3
The diagnosis of unilateral renal agenesis can be done as soon as 10-12 weeks of gestation by US.1 Unilateral renal agenesis is accompanied by gynecological malformations in around 3760% of cases.7 Other less frequent urinary tract malformations, such as horseshoe kidney, pelvic kidney, multicystic dysplastic kidney and duplication of the collecting system, can also be associated with MDA.3,8
These anomalies are usually asymptomatic, and very difficult to detect by imaging studies during infancy, except in the first two to three months of life and around or after puberty.2,3 US is a very important tool for kidney evaluation, but it has some limitations in the evaluation of pre-pubertal uterus due to its small size in the absence of estrogenic stimulation. Nevertheless, US is the first-line imaging modality in the evaluation of the gynecologic system.9 Additional information can be obtained by US after retrograde saline filling of the vagina (US genitography), and adequate acoustic window can be achieved using retrograde saline filling of the bladder (before achievement of urinary sphincter control) and/or of the rectum.2,9
Although MRI has been considered the gold standard for the diagnosis of reproductive tract defects, because of its excellent imaging of both internal and external contour of the uterus in adulthood and older children; this might not be true for small children.3,5,6,9 Even with MRI, detailed anatomic assessment of the infantile non-obstructed uterus might be difficult. Some authors recommend genital tract evaluation by MRI in all prepubertal girls with known renal abnormalities in order to prevent later complications.10 In our opinion, and also according to other authors, in pediatric patients a dedicated and complete genital US examination is still the most important imaging technique, and MRI should be regarded as an additional tool for doubtful and/or complex cases.9
Several cases are described in the literature associating unilateral renal agenesis and uterine and/or vaginal defects. A recent series of 87 patients with uterine anomalies and renal agenesis showed a predominance of uterus didelphys (77%) followed by bicornuate uteri (11,5%); and over 95% of associated obstructed hemivagina.11 The association of renal agenesis and didelphys uterus with unilateral cervical atresia, as in our case description, was found in only 4,5% of those cases.11
Our case illustrates a 12-year-old female with a rare association of unilateral renal agenesis and a didelphys uterus with unilateral cervical atresia and a normal vagina. The diagnosis was done by US and MRI, after four months of pelvic and abdominal pain associated with metrorrhagia. At that point, an obstructed left hemi-uterus with haematometra was found.
We intend to alert pediatricians, nephrologists and radiologists for the association between unilateral renal agenesis and uterovaginal anomalies. The neonatal period is an excellent opportunity to detect gynecologic malformations. US and MRI are very important non-invasive tools to characterize the possible abnormality. The early detection of defects will anticipate uterovaginal therapeutic measures to prevent symptoms and future complications.
REFERENCES
1. Tozcan T. Prenatal diagnosis of renal agenesis. UpToDate. acessed in April 2015. [ Links ]
2. Gassner I, Geley TE. Ultrasound of female genital anomalies. Eur Radiol. 2004; 14:L107-22. [ Links ]
3. Iverson RE, DeCherney AH, Laufer MR. Clinical manifestations and diagnosis of congenital anomalies of the uterus. UpToDate. acessed in April 2015. [ Links ]
4. The American Fertility Society Classification of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Müllerian anomalies and intrauterine adhesions. Fertil Steril 1988; 49:944-5. [ Links ]
5. Behr SC, Courtier JL, Qayyum A. Imaging of Müllerian duct anomalies. Radio Graphics. 2012; 32: E233-50. [ Links ]
6. Junqueira BLP, Allen LM, Spitzer RF, Lucco KL, Babyn PS, Doria AS. Müllerian duct anomalies and mimics in children and adolescents: correlative intraoperative assessment with clinical imaging. Radio Graphics. 2009; 29:1085–103. [ Links ]
7. Barakat AJ. Association of unilateral renal agenesis and genital anomalies. Case Rep Clin Pract Rev. 2002; 3: 57-60. [ Links ]
8. Kiechl-Kohlendorfer U, Geley T, Maurer K, Gassner I. Uterus didelphys with unilateral vaginal atresia: multicystic dysplastic kidney is the precursor of renal agenesis and the key to early diagnosis of this genital anomaly. Pediatr Radiol. 2011; 41:1112–6. [ Links ]
9. Riccabona M, Lobo ML, Willi U, Avni F, Damasio B, Ording- Mueller, et al. ESPR uroradiology taskforce and ESUR paediatric work group -Imaging recommendations in paediatricuroradiology, part VI: childhood renal biopsy and imaging of neonatal and infant genital tract. Minutes from the task force session at the annual ESPR Meeting 2012 in Athens on childhood renal biopsy and imaging neonatal genitalia. Pediatr Radiol. 2014; 44:496-502. [ Links ]
10. Hollander MH, Verdonk PV, Trap K. Unilateral Renal Agenesis and Associated Müllerian Anomalies: A Case Report and Recommendations for Pre-adolescent Screening. J Pediatr Adolesc Gynecol. 2008, 21:151-3. [ Links ]
11. Fedele L, Motta F, Frontino G, Restelli E, Bianchi S. Double uterus with obstructed hemivagina and ipsilateral renal agenesis: pelvic anatomic variants in 87 cases. Human Reproduction. 2013; 28; 6:1580-3. [ Links ]
CORRESPONDENCE TO
Joana Gaspar
Department of Pediatrics
Hospital de Santa Maria
Centro Hospitalar Lisboa Norte
Avenida Professor Egas Moniz, 1649-035 Lisboa
Email: joanagaspar@ymail.com
Received for publication: 27.10.2016 Accepted in revised form: 05.12.2016


{kind=link}
{kind=link}