










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.26 no.1 Porto mar. 2017
CASE REPORTS | CASOS CLÍNICOS
Belly Dancers Syndrome - a diagnostic challenge
Síndrome de Belly Dancer – um desafio diagnóstico
Ana Raquel MoreiraI; Ana Cristina FreitasI; Felisbela RochaI; Raquel CardosoI; Paula FonsecaI
I Department of Pediatrics, Centro Hospitalar Médio Ave. 4761-917 Vila Nova de Famalicão, Portugal. araquelsmoreira@gmail.com; anacrisfrei@gmail.com; rocha.felisbela@gmail.com; raquel.cardoso@chma.min-saude.pt; paulamrfonseca@hotmail.com
Correspondence to
ABSTRACT
Introduction: Belly Dancers syndrome is a rare movement disorder characterized by involuntary contractions of the diaphragm, causing abnormal movements in the abdominal wall. Many different causes were described such as trauma, infections, metabolic disorders and drug ingestion. Sometimes the cause remains uncertain and a psychogenic disturb has been suggested in others.
Case report: A 14-year-old female presented with episodic involuntary movements of the abdomen that had started one week after falling. Besides these abnormal movements, physical examination was unremarkable. Belly Dancers syndrome was suspected and the neuroimaging revealed C3 and C4 nerve root injuries and several vertebral lesions. The treatment performed included oral chlorpromazine, immobilization with Jewett vest, rest and physiotherapy, with remarkable symptoms improvement.
Discussion: This clinical presentation of this syndrome is quite unusual, which may lead to late diagnosis or ineffective treatments. We report a case of traumatic Belly Dancers syndrome that improved significantly with stabilization of the lesion.
Keywords: Belly Dancers syndrome;abdominal movements; adolescence; trauma; involuntary movements
RESUMO
Introdução: A síndrome de Belly Dancer é um distúrbio raro do movimento, caracterizado por contrações involuntárias do diafragma, causando movimentos anormais da parede abdominal. As várias causas descritas incluem trauma, infeções, distúrbios metabólicos ou ingestão de drogas. A causa pode permanecer incerta ou ser atribuída a distúrbios psicogénicos.
Caso Clínico: Adolescente de 14 anos de idade, sexo feminino, recorreu ao serviço de urgência por movimentos abdominais involuntários, com início uma semana após queda. Apesar desses movimentos anormais, o exame físico era normal. Colocada a hipótese de síndrome de Belly Dancer, realizou neuroimagem que revelou várias lesões vertebrais, incluindo a nível das raízes nervosas de C3 e C4. O tratamento incluiu clorpromazina oral, imobilização com colete de Jewett, repouso e fisioterapia, com melhoria dos sintomas.
Discussão: Pela raridade e apresentação clínica incomum, o diagnóstico e respetivo tratamento podem ser tardios. Relatamos um caso com origem traumática e melhoria significativa após estabilização da lesão.
Palavras-chave: Síndrome de Belly Dancer;adolescência; movimentos abdominais; trauma; movimentos involuntários
BACKGROUND
Belly Dancers Syndrome (BDS), also known as diaphragmatic flutter, first described by Antony van Leeuwenhoek in 1723 is a rare movement disorder.1,2 The descriptions in the literature are mostly based on case reports, and the largest series published was by Patterson in 2011. This syndrome is characterized by involuntary, repetitive and irregular contractions of the diaphragm, causing a vibration of the adjacent muscles such as the abdominal wall.2 Although the pathophysiology of this condition is unclear, it has been associated with central and peripheral nervous system disorders, such as encephalitis and phrenic nerve irritation, pleural disorders, mediastinal disorders, intra-abdominal disorders, heart diseases, cardiac and thoracic surgeries, idiopathic cervical spine trauma, and lung diseases.2,3 In some cases the cause remains uncertain and a psychogenic origin has been suggested by others.2,4 The paroxysmal beats of the abdominal wall, especially in the epigastric region, are usually the most common presentation being unrelated to the heart and respiratory rates, commonly disappearing during sleep.4,8 The rate of the contractions is variable, with a frequency rate ranged from 35 to 480 contractions per minute.2 These movements can cause abdominal pain and dyspnea frequently.4 Respiratory distress, hyperventilation, hiccups or belching can also be present.8 These paroxysms usually last from a few seconds to months with variable asymptomatic breaks.2 In the cases described, the age of the patients ranged from four months to ninety-three years.4
CASE REPORT
A healthy 14-year-old female presented in the emergency department with episodic, intermittent involuntary movements of the abdominal wall, which had been started three weeks before. Initially they were infrequent and painless and later they started to occur every day. Although these movements were sporadic,
they sometimes persisted for several minutes causing abdominal pain, mainly in the epigastric region, and sometimes some respiratory distress was associated. There were no exacerbating or relieving factors. These movements did not occur during sleep. She also referred occasionally dorsal pain characterized as a sting pain and sometimes involuntary movements of her left leg, mainly when she was lying supine, which were not related. She denied any drug consumption.
After being questioned again she admitted that these episodes had started a week after falling 1.5 meters high, while she was playing with friends at school, without significant pain, conscience loss or other symptoms associated. On the day of the fall it was activated the school insurance and she was taken to the emergency room of a local hospital. She was observed and a spine x-ray was performed, which was normal. She was discharged recommending clinical surveillance.
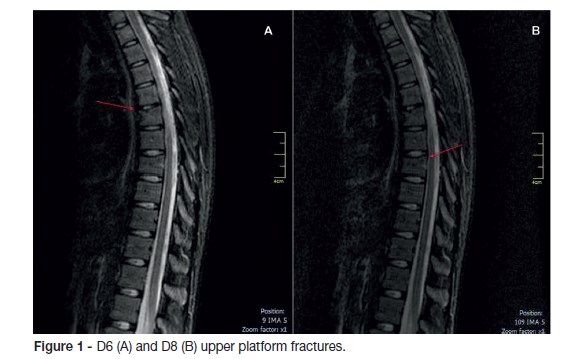
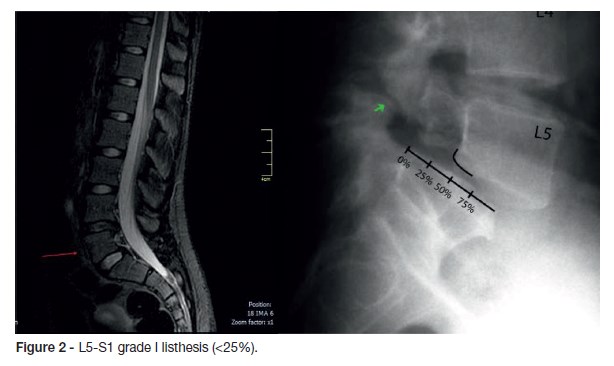
Because of the appearance of movements previous described, with progressive worsening she was admitted to the emergency pediatrics department of a level 2 hospital. On her physical examination she was conscious and presented no focal neurologic deficit, including sensitivity asymmetries. It was evident rapid involuntary abdominal wall movements observed either in orthostatic and supine position (about 200 abdominal movements per minute, unrelated to respiratory cycles). When lying down there was observed involuntary, repetitive and rhythmic movements of her left leg. No other abnormal movements were detected. Physical and neurological exam were otherwise normal. The episodes were video recorded. The workup, including cells blood count, electrolytes and blood gases had no abnormalities. Vertebral magnetic resonance imaging (MRI) showed C3 and C4 signs of nerve root injury, D6 and D8 upper platform fractures, L4-L5 median and right paramedian herniated disc and L5-S1 grade I listhesis (images 1 and 2). In spite of being specifically asked it wasnt possible to visualize the phrenic nerve tract in the MRI. The electromyography (EMG) of the abdominal muscles was not performed, due to lack of cooperation.
The clinical case was discussed both with Orthopedics and Neurosurgery and it was decided an expectant attitude.
She was then admitted to the Pediatric Department with oral chlorpromazine (25 mg, PO) for acute symptoms exacerbation, column stabilization with Jewett vest and physiotherapy. There was a remarkable improvement after the immobilization and therapy with chlorpromazine was just required on the first day of admission. She maintained immobilization with the vest and physiotherapy for five weeks. She remained follow-up in the outpatient consultation for two years.
DISCUSSION
The diaphragm is the main inspiratory muscle in humans. The third to the fifth cervical ventral spinal rami form the phrenic nerves in the upper part of the scalenus anterior muscle, innervating the diaphragm.5 BDS is a form of myoclonic contraction of the diaphragm, similar to hiccups, but with a higher frequency and with no inspiratory sound associated.1-3 Spinal mechanisms have been postulated as an etiology, especially neuronal reorganization in response to a structural lesion in the spinal cord.6 The mechanism involved on the production of this flutter may be related with abnormal excitation of the phrenic nerve: by disturbances of the central nervous system, over the presence of irritating factors anywhere along the phrenic nerve, or even by the irritation of the phrenic nerve itself.2,3,7 Usually, the involvement is unilateral in peripheral lesions and bilateral in central lesions.1,4 No standardized treatment has proven to be effective.4 It should be directed toward the etiology.2 A range of therapies have been described, including diazepam, carbamazepine, phenytoin, chlorpromazine, phrenic nerve block or transection.9
In our patient, C3 and C4 nerve root lesions as well as the other lesions previously described, were linked to trauma. The rhythm and frequency of her abdominal movements might translate bilateral diaphragmatic flutter. Trauma may precede movement disorders, such as BDS, complex regional pain syndrome, and hemifacial spasm, changing functional connectivity of spinal sensoriomotor circuits.7 This may explain the atypical leg movements in our patient.
BDS diagnosis is clinical, and can eventually be proven by fluoroscopy or electrophysiological studies showing diaphragm movement.10 An EMG was performed in our patient but, because of lack of collaboration, it was possible only of her leg muscles.
The etiology can be multifactorial; in this case the evidence of a significant previous falling and spine lesions observed can explain the traumatic cause.
It was used chlorpromazine (for acute symptom relive), due to its efficacy in persistent hiccups; it may have also been helpful once it acts centrally by dopamine antagonism in the hypothalamus. It has been reported a similar case, in a newborn male, in whom symptoms improved with use of chlorpromazine.11 Due to its rarity, this syndrome is often undervalued and underdiagnosed, being frequently attributed to psychosomatic disorders. A detailed history and careful physical examination are crucial for a correct diagnosis, avoiding unnecessary investigations and drugs. Although a traumatic etiology might be more readily recognized, other causes of BDS must be considered, which may be reversible with specific treatment.
REFERENCES
1. Phillips JR, Eldridge FL. Respiratory myoclonus (Leeuwenhoeks disease). N Engl J Med. 1973 Dec 27;289:1390-5. [ Links ]
2. Rigatto M, Medeiros N. Diaphragmatic flutter. Report of a case and review of literature. Am J Med. 1962 Jan;32:103-9. [ Links ]
3. Inglhilleri M, Conte A, Frasca V, et al. Belly Dance Syndrome Due to Spinal Myoclonus. Mov Disord. 2006; 2:394-6. [ Links ]
4. Patterson V. Belly Dancers Syndrome: causes, clinical presentations, and treatment. In: http://www.logan.edu/mm/files/LRC/Senior-Research/2011-Dec-31.pdf. Accessed Jun 2014. [ Links ]
5. Romanes GJ. Cunninghams manual of practical anatomy. Oxford: Oxford University Press; 1986. [ Links ]
6. Iliceto G, Thompson PD, Day BL, et al. Diaphragmatic flutter, the moving umbilicus syndrome, and belly dancers dyskinesia. Mov Disord. 1990;5:15-22. [ Links ]
7. Alvarez MV, Driver-Dunckley EE, Caviness JN, et al. Case series of painful legs and moving toes: clinical and electrophysiologic observations. Mov Disord. 2008;23:2062-6. [ Links ]
8. Chen, R. Remtulla, H. Bolton, C. Electrophysiological study of diaphragmatic myoclonus. J Neurol Neurosurg Psychiatry. 1995; 58:480-3. [ Links ]
9. Katz ES, Gauda E, Crawford T, et al. Respiratory flutter syndrome an underrecognized cause of respiratory failure in neonates. Am J Respir Crit Care Med. 2001;164:1161-4. [ Links ]
10. Ramírez JD, Gonzales M, Hoyos JA, Grisales L. Aleteo diafragmático. Descripción de caso y revisión de la literatura. Neurología. 2015;30:249-51. [ Links ]
11. Panigrahy N, Kumar PP and Chirla DK. Respiratory Flutter Symdrome in a Neonate. Indian Pediatr 2013;50:242-3. [ Links ]
CORRESPONDENCE TO
Ana Raquel Moreira
Department of Pediatrics
Centro Hospitalar Médio Ave
Rua Cupertino de Miranda s/n Apartado 31
4761 - 917 Vila Nova de Famalicão
Email: araquelsmoreira@gmail.com
Received for publication: 30.03.2016 Accepted in revised form: 28.07.2016


{kind=link}
{kind=link}