










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
Print version ISSN 0872-0169
Port J Nephrol Hypert vol.34 no.4 Lisboa Dec. 2020
https://doi.org/10.32932/pjnh.2021.01.097
PERSPECTIVE
Ultrasound in vascular access management – How to start and enhance a comprehensive program
Tiago Assis Pereira
Nephrology Department, Hospital Curry Cabral, Centro Hospitalar Lisboa Central, Lisbon, Portugal
INTRODUCTION
Diagnostic medicine has evolved from a solely physical examination to a setting where a diversity of complementary diagnostic methods is applied. Subsequently, most diagnosis and therapeutics are performed after appropriate exams confirming the clinical suspicion.
Similarly, vascular access (VA) creation and monitoring has been revolutionized by ultrasound (US) implementation, thereby supplanting physical examination and sparing angiographic/surgical interventions through 1) deciding the location of VA creation, 2) diagnosing dysfunctional VA and 3) establishing if a vascular lesion needs to be corrected (vs conservative management).
This article presents the author´s perspective of a VA ultrasound program, after its implementation and expansion in the Nephrology Department of Hospital Curry Cabral. The programme was founded in mid‑2017 as an external consultation, and then enhanced to give support to hospitalized patients (dialysis or pre‑dialysis patients admitted for or with vascular issues). A total of 330 vascular mapping and 278 VA ultrasound evaluations were performed by December 2020.
ROLE OF ULTRASOUND MAPPING FOR VASCULAR ACCESS CREATION
After an appropriate history and physical examination, preoperative vascular mapping by US should be the next step in vascular access creation.
At first, it was advocated only for patients with previous multiple or failed access creation, inconclusive physical exam or sociodemographic and clinical risk factors for VA failure. Thereafter, its utilization has been increasingly extended and in some centers a model of universal evaluation has been adopted.
Not all studies were concordant as to US superiority against physical examination, and international guidelines and area specialists still disagree on its performance on a universal basis, a position strongly defended by the Spanish clinical guidelines. Either way, together with clinical findings (history and physical exam) ultrasound information should enable an integrative and structured surgical decision.1,2 Yet, ultrasound’s non‑invasive nature and the avoidance of unnecessary surgeries resulting in mal‑functioning or mal‑functioning VA are benefits to be considered. The latter, ultimately, leads to the need of a central venous catheter for dialysis initiation and discourages patients for future surgeries.
ROLE OF ULTRASOUND FOR VASCULAR ACCESS EVALUATION
The purpose of VA evaluation is to determine if VA is normally functioning, to reduce the risk of thrombosis and ultimately improve survival.1‑3
VA physical exam and, if the patient is already on dialysis, its cannulation, hemostasis difficulty, dialysis efficiency, and vascular pressure determinations can indicate VA dysfunction and the need for evaluation.
However, these features are erratic and difficult to interpret, as each one depends on many variables (cannulation technique, other determinants of dialysis efficacy suhc as dialyzer and needle sizes, for example).
More recently, access flow (Qa) availability has incremented the efficiency of VA surveillance. Qa measurement by dilution methods seems to be the most practical and reliable hemodynamic variable to be used, but it does not identify the underlying lesion and if it can or should be corrected. Moreover, these data cannot be used in a pre‑dialysis setting, since VA is not cannulated and no noninvasive Qa measurement is available.
Second‑generation methods, including US, are recommended for autologous VA surveillance; however this does not apply to prosthetic arteriovenous fistula (PAF), as they are not associated with clinical benefit.1‑4
VA guidelines have pointed out that when 1) low or significant Qa reductions are detected or if 2) poor maturation, patients should be referred to an image method, from which US is considered the first‑line method (if performed by an experienced clinician). Angiographic evaluation should be the next step if inconclusive exam or hemodynamically significant lesion.1‑3
Another US function that is widely recommended is guidance in real‑time VA cannulation, as it results in less complications and more efficient dialysis.1‑3
Overall, VA management can be optimized by US, since it combines anatomical and hemodynamic characterization, if the patient is on dialysis or not. It should be highlighted that Qa measurement is comparable between ultrasound and dilution methods.5
Joining the data gathered by this method and other clinical and semiological data means a more validated decision concerning VA can be performed.
No VA surveillance of pre‑dialysis patients is available, making this process more challenging. As a consequence, a US evaluation is required.
STARTING AN ULTRASOUND PROGRAM IN NEPHROLOGY
Four features are required to implement a US program for VA management – 1) knowledge and 2) experience of US and dialysis, 3) available ultrasound equipment and 4) time. The detail “dialysis” was intentionally placed, as we cannot expect radiologists or surgeons to be the decision‑makers of VA management. The nephrologist, who deals daily with dialysis treatment and VA complications, should be central in this process.
A US machine available full‑time or almost full‑time is essential to perform a specific and time‑consuming activity like this. An automated volume flow calculation (Qa), as specified for VA evaluation, should be inserted in the pulsed wave doppler mode.
A specific weekly time should be dedicated for first consultations (vascular mapping or VA first evaluation) and subsequent ones (VA revaluations). Ideally, in this consultation, another period should be warranted for emergencies.
There also should be availability for a prompt US evaluation as VA complications present, either at dialysis units or in‑patient departments.
MAINTENANCE AND EXPANSION OF VA ULTRASOUND PROGRAMME
There are some steps that should be featured at each VA center to grant continuous high‑standard care continuity taken to enhance scientific progression and divulgation:
– Continuous self‑formation and results monitoring – in addition to scientific accompanying and vascular access courses, self‑monitoring of individual cases by assessing construction success and survival follow‑up (in case of vascular mapping) as well as angiographic or surgical results of VA referred from US evaluation (and confronting respective US findings).
– Formation of staff – it is crucial to expand the pool of staff capable of performing US to maintain current and future activity; these should include Nephrology, Surgery, and Nursing, integrated in a comprehensive formation that also includes angiographic and operating room participation.
– Results divulgation, through scientific reunions and publications, concerning not only immediate results (e.g., vascular access construction success) but also long‑term survival.
– Reinforcement of efforts for a good vascular access – it should be noted that an arteriovenous access has to be more than just functioning; it should be usable and proportionate consistently and long‑term efficient dialysis; considering a (bad) functioning access per se as a success can be misleading; that’s why a complete characterization of an access should be performed recurring to US, and not only by physical examination.
ENTHUSIASM ON ULTRASOUND FOR VA MANAGEMENT – RISKS AND ILLUSIONS
Once US turn out to be useful and widely implemented, it can be dangerous if exam quality (image capture, full and exhaustive evaluation) and subsequent clinical decisions are not assured. As much as more clinicians at predialysis and dialysis settings have access to US machinery and predisposition to perform this practical exam, if quality is compromised the results can be as well. Ultimately, it would lead to discrediting US and blocking its stepwise pathway to a central position in VA management.
Additionally, US is not the gold standard exam to diagnose central vascular lesions and, unlike angiography, it is not interventional. Compared to the gold standard, which is angiography, US sensibility and specificity values are not superior to 90 and 95%, respectively.1
With respect to diagnosis or ultrasonographic characterization, US is operator‑dependent and it is based on hand‑technique, hemodynamic and anatomical understanding of this peculiar vascular area, and integration of semiological and dialytic data to arrive at a right decision.
PENDING DOUBTS AND RESEARCH AREAS TO EXPLORE
Acquiring knowledge, experience and changing practical paradigms are essential in VA ultrasound. As long as data is gathered and clinical challenges are presented, many doubts arise. Below, are presented some examples of particular situations, whose answer is not obvious:
Venous branching proximally to radiocephalic fistulae – When to discard this option? – Although an adequate radial artery and distal cephalic vein are available, the venous drainage is often challenging, either due to erratic paths or further divisions. These can compromise a viable segment for bipunction or create high venous pressure due to tightened drainage.
Median basilic vein – When radiocephalic or brachiocephalic fistulas do not seem advisable, the next option would be a brachiobasilic fistula. Due to its profound and internal location, the basilic system is usually spared from venous punctures or cannulations. However, it is not the case of the median basilic vein, which can be accessed or be constitutively suboptimal. Some kind of narrowing or parietal changes (sclerosis, lesser compression) that can compromise its maturation are frequent along its trajectory. Should we try median basilica veins? Most times yes, because of the lack of other native options and a regular and tight follow‑up post‑construction should identify if the access needs angiographic or surgical revision.
Biphasic arterial waveform – is it to be anastomosed? – It is not rare to find biphasic waveforms in distal arteries, including in young and low vascular burden patients. Apart from absent proximal arterial stenosis and radial acceptable diameters and SPV, experience has not been favorable (non‑ published data).
Prosthetic arteriovenous fistula – should we be strict about vascular diameters? – Usually, it is advisable that PAF would be anastomosedto vessels with at least 4 mm, to maintain an adequate flow andminimizing risk of anastomosis stenosis.1,6 However, this arterialdiameter is difficult to achieve, mainly in some patients (female,diabetic, small patients) and if we were strict, it could lead to recommendationof a proximal loop prosthesis (recurring to proximalbrachial artery), whose surgery is challenging and VA survival ishampered.
Stenosis due to neointimal hyperplasia vs constitutive narrowing – After diagnosing a stenosis, the morphological aspects of US canbe distinct. Roughly, two types of stenosis are apparent, based onthe presence /absence of luminal defect and previous inner diameterdevelopment – neointimal hyperplasia and simple constitutive narrowing.The latter corresponds to an undeveloped vascular segment (smaller diameter compared to adjacent segments and minor parietal changes). This classification can be relevant, as the nature of stenosis can be associated with different risks of recurrence and angioplastycomplications (rupture), thereby changing therapeutic approaches.Significant radial stenosis but functioning radiocephalic fistula through palmar arch and cubital development – Arterial stenosishas been increasingly recognized, and US can easily identify it, if thelesion is peripheral. One peculiar finding has been a normofunctioningfistula, yet with hemodynamically significant arterial stenosis,but whose survival depends on palmar arch and cubital compensatorydevelopment. Necessarily arterial flow has to pass through a highresistance circuit before reaching the drainage vein. If an access issuccessfully and efficiently used, there is no question. But if thisquestion is launched in a predialytic setting (and signs such as cannulation difficulties or low dialysis efficiency are not necessarily obvious)? Can we assure that arterial flow will be enough for dialysis success?
Vascular mapping and VA ultrasound in children – what is the “normal”? – When hemodialysis and AV creation are considered in pediatricpatients, we should bear in mind the particular anatomic and hemodynamicdifferences in pediatric patients. In sum, a lower diameter,reduced arterial flow and cardiac debit are expected; differently toadults, arterial disease is less probable due to reduced vascular burdenand short‑timeof uremia exposition. The big question is if the usualvascular parameters applied in adults should be recommended in pediatricpatients. If not, what are the thresholds? Recent publicationshave addressed this question and analysis of morphological parameterssuggests similar results to adults, but more data is needed.7,8
A FINAL PRAGMATIC PROPOSAL
Previous practice was to leave vascular access approach creation to surgeons and to refer a dysfunctional access to surgery or to angiographic evaluation.
At the present time, US assumes an intermediate/pivotal position in these processes.
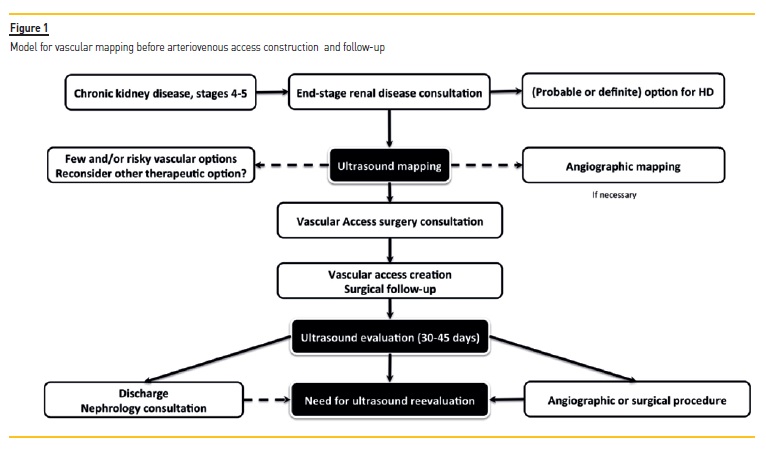
Given the theoretical advantages, the favorable clinical results and local experience, the following diagram for vascular access creation is suggested (Figure 1)
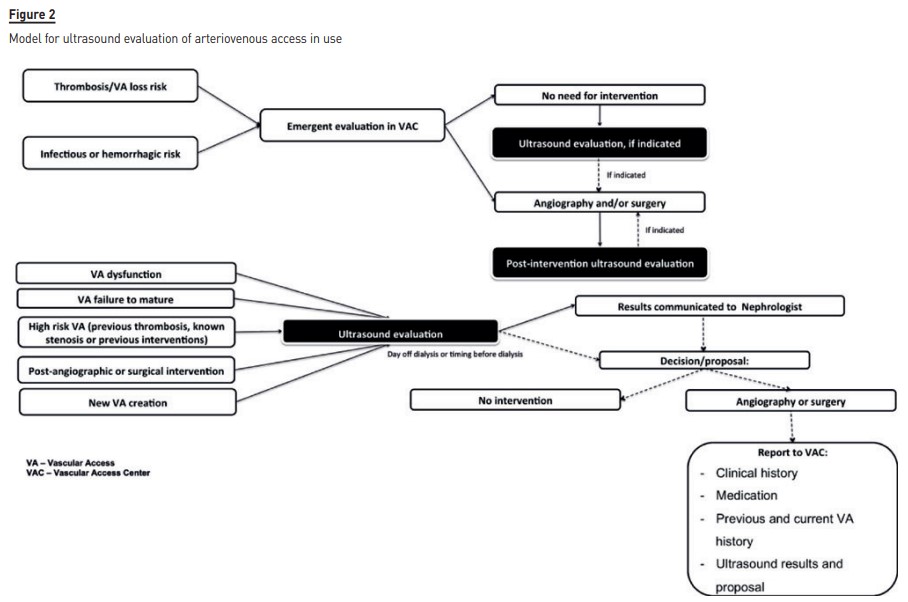
A different model should be adopted for prevalent arteriovenous access, i.e., for access that is being used. Figure 2)
Portugal has a hemodialysis providing system based mainly in extra‑hospital centers, and these are aggregated in different companies (and its respective vascular access centers). As such, a more complex model is required to uniformly assure optimal vascular access care.
There is an increasing availability of US machines; however nowadays there are still few in use. To address the needs of our population, two models are currently in use: 1) ultrasound is centralized in one site (vascular access center, for example), along with its difficult logistic and economical and patient burden and 2) rotation of the US machines in each peripheral unit, the last depending on the attributes of the local personnel (see previous chapter referring to risks and illusions in US evaluation).
Dealing with the current lack of US apparatus, the author would propose one paradox model where there is centralization of US evaluation but at a peripheral localization.
In sum, recognizably competent nephrologists in US evaluation would assume the evaluation of vascular access patients at their dialysis center, after referral. These evaluations would be performed jointly with nursing and local medical staff, to ultimately decide the plan (vigilance, puncture counselling, angiographic or surgical referral). Despite this, emergency evaluation should be still be assured by a vascular access center.
This allows for a less‑error prone and uniform method of vascular access approach.
CONCLUSIONS
As with everything in life, innovation is at first mistrusted, then accepted and, eventually, becomes widely implemented.
This process is happening at an accelerated pace for US for vascular access care, as US seems to be one of the more breakthrough advances in this area. Along the way, many difficulties are encountered, and a mix of learning and effort is required to correctly implement this new tool.
Last, but not least, after its implementation, care should be taken to allow 1) maintenance of US‑based decisions’ quality and reliability, 2) continuous training and practice of medical personal and 3) enhancement of vascular access programs (dialysis and pre‑ References 1. Ibeas J, Roca‑Tey R. Guía Clínica española del acceso vascular para hemodiálisis. Nefrologia. 2017;37(1): 1‑191. [ Links ] 2. Lok C, Huber T, Lee T, Shenoy S, Yezlin A, Abreo K, Allon M et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. 2020; 75(4): S1‑S164. [ Links ] 3. Gallieni M, Hollenbeck M, Inston N, Kumwenda M, Powell S, Tordoir J et al. Clinical practice guideline on peri and postoperative care of arteriovenous fistulas and grafts for haemodialysis in adults. Nephrol Dial Transplant. 2019; 34(2): 1‑42. [ Links ] 4. Tonelli M, James M, Wiebe N, Jindal K, Hemmelgarn B. ultrasound monitoring to detect access stenosis in hemodialysis patients: a systematic review. Am J Kidney Dis. 2008; 51: 630‑640. [ Links ] 5. Roca‑Tey R, Rivas A, Samon R, Ibrik O, Viladoms J. Study of vascular access by color Doppler ultrasonography. Comparison between delta‑h and cdu methods in measuring VA blood flow rate. Nefrología. 2005; 25: 678‑683. [ Links ] 6. Akoh J. Prosthetic arteriovenous grafts for hemodialysis. J Vasc Access. 2009; 10: 137‑147. [ Links ] 7. Shroff R, Sterenborg R, Kuchta A, Arnold A, Thomas N, Stronach L, Padayachee S, Calder F. A dedicated vascular access clinic for children on haemodialysis: two years’ experience. Pediatr Nephrol. 2016; 31(12): 2337‑2344. 8. Huynh T, Garza B, Geer J, Broadbent K, Martinek W, Correa A, Swartz S, Srivaths S, Brewer E. The role of preoperative duplex ultrasound vessel mapping in determining primary failure of pediatric hemodialysis arteriovenous fistula. J Vasc Ultrasound. 2019. 43 (2): 63‑68 [ Links ] Tiago Assis Pereira, MD Nephrology Department, Hospital Curry Cabral, Centro Hospitalar Lisboa Central Lisboa, Portugal E‑mai: tiagoassispereira@gmail.com Disclosure of potential conflicts of interest: none declared Received for publication: Dec 11, 2020 Accepted in revised form: Dec 21, 2020


{kind=link}
{kind=link}