










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
Print version ISSN 0872-0169
Port J Nephrol Hypert vol.32 no.4 Lisboa Dec. 2018
REVIEW ARTICLE
Renal denervation for resistant hypertension: a glimpse of hope on the horizon?
Davide Bolignano
CNR – Institute of Clinical Physiology, Reggio Calabria, Italy
ABSTRACT
Renal denervation by a minimally‑invasive catheter‑based procedure has been extensively studied over the last decade as a powerful tool for treating resistant hypertension, a high‑risk condition the clinical management of which remains a major challenge. Initial promising results from uncontrolled pilot studies set the stage for a plethora of larger randomized, sham‑controlled trials which, however, had unexpectedly negative findings. Despite this transient setback, positive although weak results from the latest Symplicity Spyral studies and a series of new procedural approaches beyond radiofrequency have rekindled enthusiasm for this procedure. New studies are warranted to fully elucidate, once and for all, the limits and potential of and indications for renal denervation in the treatment of resistant hypertension.
Keywords: renal denervation, resistant hypertension, nerve ablation.
INTRODUCTION
Hypertension remains a major public health problem and one of the most relevant causes of mortality, morbidity and hospitalizations worldwide. In the general populations, the overall prevalence of this condition peaked at 26% in 2000 and it is forecast that more than 1.56 billion patients will be hypertensive by 20251. Roughly 3 to 6 % of the whole hypertensive population is considered as resistant2. Individuals with resistant hypertension, by definition, show an office blood pressure ≥140/90 mmHg despite taking three different classes of antihypertensives (including a diuretic) at maximally tolerated doses or using ≥4 medications irrespective of blood pressure3. Resistant hypertension ranks among the most important prognostic risk factors for adverse cardiovascular and renal outcomes4.
Unfortunately, various dietary, lifestyle or behavioral programs, alone or in addition to stepped therapeutic algorithms, have failed to significantly improve this condition. The search for effective treatments to properly manage resistant hypertension has been acknowledged by the scientific community as a true research priority. In recent years, improved understanding of the role of the sympathetic nervous system and the enormous advancement in health technology have laid the groundwork for several minimally invasive, device‑based approaches targeting nervous reflexes that might contribute to a unstable blood pressure control.
Among these, renal denervation remains the procedure that has accumulated the most relevant amount of pre‑clinical and randomized experience, with over 4000 indexed publications in scientific literature and a wealth of promising, ongoing studies, the results of which are expected to be available within the next few years.
A RATIONALE FOR RENAL DENERVATION IN RESISTANT HYPERTENSION
The pathophysiological rationale for renal denervation as a measure for improving blood pressure control relies on the sophisticated bidirectional interaction between the kidney and the sympathetic nervous system.
Efferent nervous fibers, the stimulation of which elicits renal vasoconstriction, renin release, retention of water and sodium and blood flow reduction, originate in the brain and terminate in the juxtaglomerular apparatus in the renal cortex after traveling through the spinal cord. On the contrary, afferent fibers arise in the renal pelvis, conveying sympatho‑excitatory stimuli to the autonomic regulatory nucleus tractus solitarius in the midbrain5. Sympathetic over‑reactivity of the renal nervous autonomic plexus plays a key role in the pathophysiology of arterial hypertension, a concept that was already known in the pre‑pharmacological era of hypertension management in which the most severe forms were clumsily treated by extensive splanchnicectomy6.
However, although effective, this unselective, highly destructive surgical approach was unsuitable to be routinely performed, taking into consideration the high peri‑operative risk and the several major neurological sequela that impacted patients conditions more significantly than resistant hypertension itself.
In recent years, the smart idea to destruct renal nerves in a minimally invasive way, by means of energy delivered from the lumen of the arterial vascular branches, has injected fresh excitement into the possibility of successfully challenging resistant hypertension using a non‑pharmacological approach.
As a result, myriad highly specialized, catheter‑based devices have been conceived, leading to a wealth of pre‑clinical and clinical experience with contradictory findings that, unfortunately, still prevents the drawing of any final conclusions on the potential use of this procedure in routine practice.
RENAL DENERVATION BY RADIOFREQUENCY: A MATTER OF SIMPLICITY
Energy delivered by radiofrequency was the first and is the most studied technique to obtain renal nerve ablation and the Symplicity System (Medtronic, US) is the pioneering, catheter‑based device which has led the majority of scientific studies conducted so far on renal denervation.
The first generation of this device consisted of a radiofrequency, generator‑coupled arched catheter with a max 8W energy delivery to target tissue temperature of 40‑75ºC. A second spiral version (Symplicity Spyral) was subsequently conceived to overcome the problem of concentrating focal energy into a single artery segment.
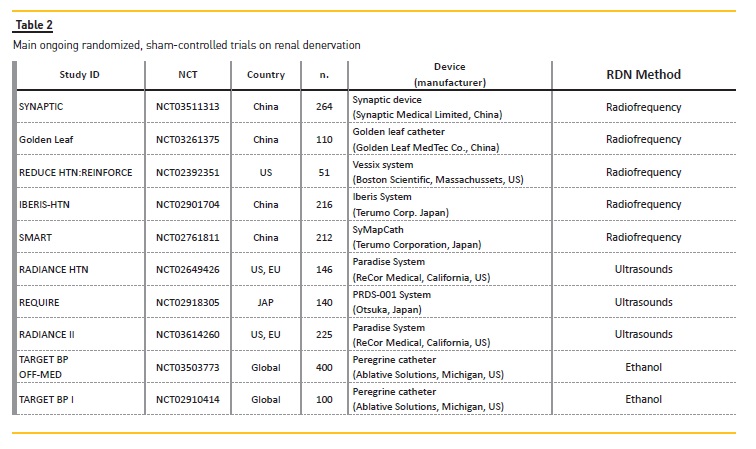
Other radiofrequency catheters exist, including the OneShot (Medtronic, US; formerly Covidien), the Vessix System (Boston Scientific, US), the EnligHTN (Abbott, US; formerly St. Jude), the PRDS‑001 System (Otsuka, Japan), the SyMapCath (Terumo Corporation, Japan), the Synaptic device (Synaptic Medical Limited, China) the Golden Leaf catheter (Shanghai Golden Leaf MedTec Co., China), the saline‑irrigated, radiofrequency catheter Thermacool (Biosense‑Webster, California, US) and the Iberis System (Terumo Corporation, Japan).
Findings on these devices has rapidly accumulated but remains mostly limited to small proof‑of‑principle, uncontrolled studies7‑9.
The SYMPLICITY HTN‑1, a large pilot, uncontrolled prospective study, was the first trial demonstrating the Symplicity radiofrequency catheters capacity to reduce blood pressure by renal denervation in individuals with resistant hypertension and to maintain this benefit long‑term10.
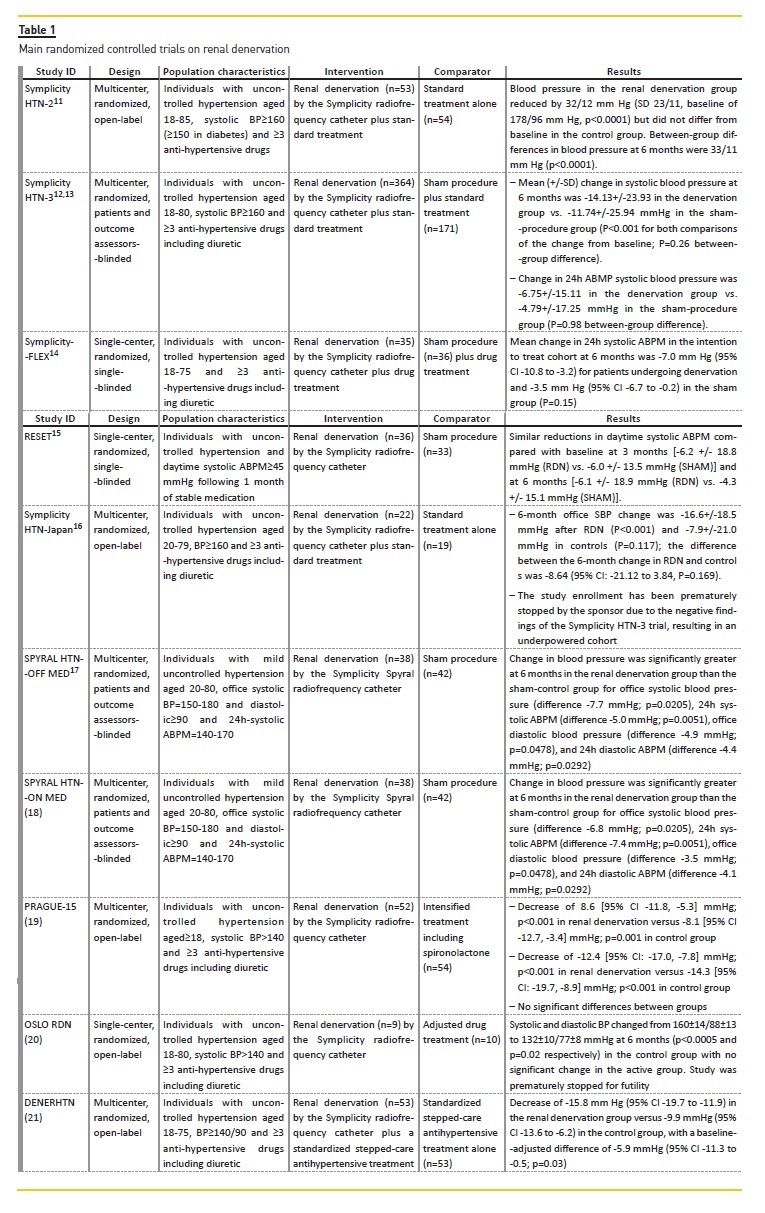
The SYMPLICITY HTN‑211, a multicenter, prospective, open‑label, controlled trial, followed soon after. This study randomized 106 resistant hypertensive patients to renal denervation or standard therapy, demonstrating, after 6 months, a reduction in office systolic/diastolic blood pressure in the renal denervation group by 32/12 mmHg (p<0.0001) with no changes in the control group and a between‑group difference of 33/11 mmHg (p<0.0001).
The following SYMPLICITY HTN‑312 was the first multicenter, randomized, pivotal trial employing a controlled group receiving a sham‑procedure.
The study recruited 535 participants with resistant hypertension worldwide. Despite high hopes, the study failed to prove the superiority of renal denervation over sham to improve office blood pressure. Unexpectedly, the mean systolic blood pressure decreased at 6 months in both the experimental and control group (‑14.13 ± 23.93 and ‑11.74 ± 25.94 mmHg, respectively; p<0.001 for both comparisons of the change from baseline) with a non‑significant between‑group difference(p=0.26), an observation confirmed also when looking at the pattern of 24h ambulatory systolic blood pressure13.
Two other independent randomized studies (14,15) implementing a sham‑controlarm echoed suchnegative findings. Failure of the SYMPLICITY HTN‑3alsoled to premature stopping of another sponsored randomized,(non‑sham)controlled trial, the SYMPLICITYHTN‑JAPAN16,which results were eventually inconclusivedue to underpowering.
Despite this setback apparently crushing spirits and dreams, results from two recent multicenter trials specifically designed to overcome potential limits of the SYMPLICITY HTN‑3 have sparked new enthusiasm about the potential of this procedure.
The SPYRAL HTN‑OFF and ON MED trials (17, 18) were two randomized, sham‑controlled, proof‑of‑principle studies implementing the last‑generation Symplicity Spyral in the absence (SPYRAL HTN‑OFF MED) and presence (SPYRAL HTN‑ON MED) of background antihypertensive therapy. In a 3‑month analysis of the SPYRAL HTN‑OFF MED17, the renal denervation group (n=38) experienced a statistically significant decrease in blood pressure compared with the sham‑controlled group (n=42) although change differences were as little as 5 and 4.4 mmHg for 24‑h systolic and diastolic ambulatory measurement and 7.7 and 4.9 mmHg for office blood pressure, respectively. The first recently published 6‑month interim report of the SPYRAL HTN‑ON MED showed similar, clinically limited, benefits18 with systolic and diastolic drop differences between the renal denervation and the sham‑control group of 7.4 and 4.1 mmHg for 24h‑ABPM and 6.8 and 3.5 mmHg for office blood pressure measurements, respectively.
Three more randomized, open‑label, controlled trials adopting the first generation Symplicity catheter deserve mentioning. The PRAGUE‑15 trial19, allocated 106 individuals with resistant hypertension to renal denervation or an intensified drug treatment. Again, a significant reduction in 24‑h and office systolic blood pressure was observed in both groups with no significant between‑group difference after 6‑months.
The OSLO RDN study20, randomized 19 patients with uncontrolled hypertension to renal denervation (n=9) or clinically adjusted drug treatment (n=10). The study was interrupted prematurely due to futility of results on the main blood pressure endpoints.
Finally, the DENERHTN21 compared the efficacy of renal denervation on daytime ambulatory blood pressure control in addition to a structured, stepped‑care antihypertensive treatment versus the same treatment alone.
Interestingly, this study was apparently the only one reporting convincing results in favor of renal denervation with a mean change in systolic ABPM at 6 months of ‑15.8 mmHg (95% CI ‑19.7 to ‑11.9) versus ‑9.9 mmHg (95% CI ‑13.6 to ‑6.2) in the control group, with a significant baseline‑adjusted, between‑group difference of ‑5.9 mmHg (95% CI ‑11.3 to ‑0.5; p=0.03). An overview of the most important randomized controlled trials of renal denervation is provided in Table 1.
RENAL DENERVATION BEYOND RADIOFREQUENCY: ALTERNATIVE METHODS
Alternative techniques to radiofrequency have been studied for improving renal nerve ablation success and minimize safety risks. The Paradise system (ReCor Medical, US), the TIVUS (Cardiosonic, Israel), the Kona (Kona Medical, US) and the Sound 360 system (Sound Interventions, US) are device‑based catheters designed to ablate renal nerves via ultrasound‑derived energy generated by a piezoelectric micro‑transducer usually placed inside a low‑pressure balloon. Efficacy and safety of these devices is object of several ongoing investigations (Table 2).
The Peregrine catheter (Ablative Solutions, US) is coupled with a triple micro‑needle system to inject ethanol into the perivascular space. Alcohol is endowed with strong neurolytic effects, leading to fast nerve disruption22. Efficacy and safety of this approach is presently being tested by two global, randomized, double‑blind, multicenter, sham‑controlled trials23,24.
Alternative to ethanol, other neurotoxic agents such as vincristine and the pro‑apoptotic neurotrophic agent NW2013 have shown promising findings in small uncontrolled studies25.
Further, innovative procedures to achieve renal nerve ablation include vascular brachytherapy with renal sympathetic nerve destruction via β‑radiation exposure26 and cryotherapy27.
This latter procedure was successfully conducted in two case series27,28 of individuals who were refractory to standard renal denervation by radiofrequency, through a standard electrophysiology cardiac cryoablation catheter (Freezor(R)Xtra, Medtronic, US) targeting a tissue temperature of −75 °C for 4 mins in each renal artery. Positive results with no major damages to kidney and vasculature have laid the groundwork for a larger, non‑randomized, controlled study that is currently ongoing29.
DISCUSSION
Failure of the SYMPLICITY HTN‑3 and the other sham‑controlled RCTs have brought renal denervation to a screeching halt, which was duly justified by negative findings from pooled efficacy meta‑analyses30,31.
Nevertheless, recent bittersweet results in clinical benefits from the SPYRAL HTN‑OFF/ON MED studies and the large bunch of ongoing studies at the horizon are suggesting that the momentum for renal denervation may continue.
Some key issues which emerged from the SYMPLICITY HTN‑3 and the other large sham‑controlled trials were not or only marginally addressed by the following SPYRAL evidence. Overcoming these limitations represents a plausible basis for intelligent and unbiased investigations designed to clarify the true usefulness of this procedure in the real world.
One main problem, for instance, is the importance of the study population selection. As a successful blood pressure decrease is usually manifested one month after the procedure, early prediction of responding individuals becomes rather challenging. Renal nerve ablation by radiofrequency or ultrasound energy is mediated by inflammatory or degenerative processes that require some days before leading to a concrete functional damage. This paradigm justifies the search for alternative strategies to speed up or make more efficient the ablation process. As briefly alluded to, various innovative approaches (e.g. brachytherapy, cryotherapy or ethanol injection) for achieving renal nerve ablation are currently the object of multiple investigations.
At present, no concrete, reproducible surrogates of successful denervation exist. Yet, various observations indicate that one size cannot fit all, suggesting that future trials should target selected sub‑groups of patients rather than the whole resistant hypertensive population. For example, specific analyses of the Global SYMPLICITY Registry32, a prospective, multicenter international database collecting information from over 3000 patients who underwent renal denervation, advised excluding persons with large pulse pressure or isolated systolic hypertension as less likely to benefit from this procedure, probably due to pervasive arterial stiffness. Another stratified analysis by racial origin in the SYMPLICITY HTN‑3 trial pointed out Caucasian patients in the intervention group as being more prone to experience improvements in systolic BP33. Conversely, although initially hypothesized, no impact of BMI on successful renal ablation has been clearly established34.
Another important lesson from the SYMPLICITY HTN‑3 was the high frequency of medication changes.
Roughly 40% of subjects underwent known modifications in their therapeutic regimen during the trial and further data published during and after the study suggested an additional high rate of drug non‑adherence that would not otherwise have been known to the investigators35. Although the design of subsequent trials of renal denervation began to incorporate serum and urine medication adherence testing, therapeutic compliance remains a significant factor in studies which evaluate this procedure.
The fact that the renal nerves have a specific anatomy in the renal arteries is another key problem. In fact, the distance to the lumen increases as renal nerves track back in the direction of the vessel origin. Therefore, performing the procedure in the lumen of more distal renal vessels may improve success, but may significantly increase the risk of damaging the ureter or the renal veins5. Inadequate renal denervation may also depend on the operators skills and practice and on inter‑operator variability. And, very disappointingly, the majority of specialists performing renal denervation in the SYMPLICITY HTN‑3 study were relatively unfamiliar with this technique and performed no more than two procedures during the trial12.
CONCLUSIONS
In the wasteland of clinical research into improving blood pressure control and key outcomes in individuals with resistant hypertension, renal denervation remains a very promising technique that, however, deserves additional research efforts to fully elucidate its limits, potential and suitability.
Lessons from past mistakes underline the need to identify early markers of procedural response, defining subpopulations that are more likely to be responsive and optimizing ablation success, perhaps by innovative and more efficacious techniques that are an alternative to radiofrequency. Upcoming research is warranted in the near future, intended to revolutionize the intricate clinical management of such a complex disease condition.
References
1. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217‑23. [ Links ]
2. Weitzman D, Chodick G, Shalev V, Grossman C, Grossman E. Prevalence and factors associated with resistant hypertension in a large health maintenance organization in Israel. Hypertension. 2014;64(3):501‑7. [ Links ]
3. Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51(6):1403‑19. [ Links ]
4. De Nicola L, Gabbai FB, Agarwal R, Chiodini P, Borrelli S, Bellizzi V, et al. Prevalence and prognostic role of resistant hypertension in chronic kidney disease patients. J Am Coll Cardiol. 2013;61(24):2461‑7. [ Links ]
5. Sakakura K, Ladich E, Cheng Q, Otsuka F, Yahagi K, Fowler DR, et al. Anatomic assessment of sympathetic peri‑arterial renal nerves in man. J Am Coll Cardiol. 2014;64(7):635‑43. [ Links ]
6. Larsen R, Thorp A, Schlaich M. Regulation of the sympathetic nervous system by the kidney. Curr Opin Nephrol Hypertens. 2014;23(1):61‑8. [ Links ]
7. Tsioufis CP, Papademetriou V, Dimitriadis KS, Kasiakogias A, Tsiachris D, Worthley MI, et al. Catheter‑based renal denervation for resistant hypertension: Twenty‑four month results of the EnligHTN I first‑in‑human study using a multi‑electrode ablation system. Int J Cardiol. 2015;201:345‑50. [ Links ]
8. Verheye S, Ormiston J, Bergmann MW, Sievert H, Schwindt A, Werner N, et al. Twelve‑month results of the rapid renal sympathetic denervation for resistant hypertension using the OneShotTM ablation system (RAPID) study. EuroIntervention. 2015;10(10):1221‑9. [ Links ]
9. Sievert H, Schofer J, Ormiston J, Hoppe UC, Meredith IT, Walters DL, et al. Bipolar radiofrequency renal denervation with the Vessix catheter in patients with resistant hypertension: 2‑year results from the REDUCE‑HTN trial. J Hum Hypertens. 2017;31(5):366‑8. [ Links ]
10. Krum H, Schlaich MP, Sobotka PA, Bohm M, Mahfoud F, Rocha‑Singh K, et al. Percutaneous renal denervation in patients with treatment‑resistant
hypertension: final 3‑year report of the Symplicity HTN‑1 study. Lancet. 2014;383(9917):622‑9.
11. Symplicity HTNI, Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, et al. Renal sympathetic denervation in patients with treatment‑resistant hypertension (The Symplicity HTN‑2 Trial): a randomised controlled trial. Lancet. 2010;376(9756):1903‑9. [ Links ]
12. Bhatt DL, Kandzari DE, ONeill WW, DAgostino R, Flack JM, Katzen BT, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393‑401. [ Links ]
13. Bakris GL, Townsend RR, Liu M, Cohen SA, DAgostino R, Flack JM, et al. Impact of renal denervation on 24‑hour ambulatory blood pressure: results from SYMPLICITY HTN‑3. J Am Coll Cardiol. 2014;64(11):1071‑8. [ Links ]
14. Desch S, Okon T, Heinemann D, Kulle K, Rohnert K, Sonnabend M, et al. Randomized sham‑controlled trial of renal sympathetic denervation in mild resistant hypertension. Hypertension. 2015;65(6):1202‑8. [ Links ]
15. Mathiassen ON, Vase H, Bech JN, Christensen KL, Buus NH, Schroeder AP, et al. Renal denervation in treatment‑resistant essential hypertension. A randomized, SHAM‑controlled, double‑blinded 24‑h blood pressure‑based trial. J Hypertens. 2016;34(8):1639‑47. [ Links ]
16. Kario K, Ogawa H, Okumura K, Okura T, Saito S, Ueno T, et al. SYMPLICITY HTN‑Japan – First randomized controlled trial of catheter‑based renal denervation in Asian patients. Circ J. 2015;79(6):1222‑9. [ Links ]
17. Townsend RR, Mahfoud F, Kandzari DE, Kario K, Pocock S, Weber MA, et al. Catheter‑based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN‑OFF MED): a randomised, sham‑controlled, proof‑of‑concept trial. Lancet. 2017;390(10108):2160‑70. [ Links ]
18. Kandzari DE, Bohm M, Mahfoud F, Townsend RR, Weber MA, Pocock S, et al. Effect of renal denervation on blood pressure in the presence of antihypertensive drugs: 6‑month efficacy and safety results from the SPYRAL HTN‑ON MED proof‑of‑concept randomized trial. Lancet. 2018;391(10137):2346‑55. [ Links ]
19. Rosa J, Widimsky P, Tousek P, Petrak O, Curila K, Waldauf P, et al. Randomized comparison of renal denervation versus intensified pharmacotherapy including spironolactone in true‑resistant hypertension: six‑month results from the Prague‑15 study. Hypertension. 2015;65(2):407‑13. [ Links ]
20. Fadl Elmula FE, Hoffmann P, Larstorp AC, Fossum E, Brekke M, Kjeldsen SE, et al. Adjusted drug treatment is superior to renal sympathetic denervation in patients with true treatment‑resistant hypertension. Hypertension. 2014;63(5):991‑9. [ Links ]
21. Azizi M, Sapoval M, Gosse P, Monge M, Bobrie G, Delsart P, et al. Optimum and stepped care standardised antihypertensive treatment with or without renal denervation for resistant hypertension (DENERHTN): a multicentre, open‑label, randomised controlled trial. Lancet. 2015;385(9981):1957‑65. [ Links ]
22. Fischell TA, Ebner A, Gallo S, Ikeno F, Minarsch L, Vega F, et al. Transcatheter alcohol‑mediated perivascular renal denervation with the peregrine system: first‑in‑human experience. JACC Cardiovasc Interv. 2016;9(6):589‑98. [ Links ]
23. TARGET BP I Clinical Trial (TARGET BP I) 2018 [Available from: https://clinicaltrials.gov/ct2/show/NCT02910414. [ Links ]
24. The TARGET BP OFF‑MED Trial 2018 [Available from: https://clinicaltrials.gov/ct2/show/NCT03503773. [ Links ]
25. Kipshidze N, Sievert H, Wholey MH, Kipiani K, Kipiani V, Mukhuradze T, et al. First clinical experience with targeted renal nerve femodulation (TREND‑1) using a neurotropic sgent for the treatment of sympathetic hypertension. J Invasive Cardiol. 2017;29(3):97‑103. [ Links ]
26. Waksman R, Barbash IM, Chan R, Randolph P, Makuria AT, Virmani R. Beta radiation for renal nerve denervation: initial feasibility and safety. EuroIntervention. 2013;9(6):738‑44. [ Links ]
27. Prochnau D, Figulla HR, Surber R. Cryoenergy is effective in the treatment of resistant hypertension in non‑responders to radiofrequency renal denervation. Int J Cardiol. 2013;167(2):588‑90. [ Links ]
28. Prochnau D, Heymel S, Otto S, Figulla HR, Surber R. Renal denervation with cryoenergy as second‑line option is effective in the treatment of resistant hypertension in non‑responders to radiofrequency ablation. EuroIntervention. 2014;10(5):640‑5. [ Links ]
29. Pilot Study of of Renal Arterial Sympathetic Denervation by Cryotherapy (PRASDEN) 2018 [Available from: https://clinicaltrials.gov/ct2/show/NCT02345603. [ Links ]
30. Pappaccogli M, Covella M, Berra E, Fulcheri C, Di Monaco S, Perlo E, et al. Effectiveness of renal denervation in resistant hypertension: a meta‑analysis of 11 controlled studies. High Blood Press Cardiovasc Prev. 2018;25:167. [ Links ]
31. Coppolino G, Pisano A, Rivoli L, Bolignano D. Renal denervation for resistant hypertension. Cochrane Database Syst Rev. 2017;2:CD011499. [ Links ]
32. Mahfoud F, Bakris G, Bhatt DL, Esler M, Ewen S, Fahy M, et al. Reduced blood pressure‑lowering effect of catheter‑based renal denervation in patients with isolated systolic hypertension: data from SYMPLICITY HTN‑3 and the Global SYMPLICITY Registry. Eur Heart J. 2017;38(2):93‑100. [ Links ]
33. Kotsis V, Stabouli S. Renal denervation for resistant hypertension. N Engl J Med. 2014;371(2):183. [ Links ]
34. Bhatt DL, Bakris GL. Renal denervation for resistant hypertension. N Engl J Med. 2014;371(2):184. [ Links ]
35. Patel P, Gupta PK, White CM, Stanley AG, Williams B, Tomaszewski M. Screening for non‑adherence to antihypertensive treatment as a part of the diagnostic pathway to renal denervation. J Hum Hypertens. 2016;30(6):368‑73. [ Links ]
Dr. Davide Bolignano, MD
CNR – Institute of Clinical Physiology,
c/o EUROLINE, Via Vallone Petrara 55‑57,
89124 Reggio Calabria, Italy
Telephone: +39 0965393252
Fax:+39096526879
Disclosure of potential conflicts of interest: none declared.
Received for publication: Nov 11, 2018
Accepted in revised form: Nov 16, 2018


{kind=link}
{kind=link}