










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
Print version ISSN 0872-0169
Port J Nephrol Hypert vol.32 no.2 Lisboa June 2018
CASE REPORT
Light and heavy chain deposition disease – Case report
João Cassis1, Henrique Silva Sousa2, Tiago J Carvalho3, Ilídio Rodrigues3, Maria Pedro Silveira4
1Pathology Department, Centro Hospitalar Lisboa Ocidental, Lisbon, Portugal.
2 Nephrology Department, Hospital das Forças Armadas, Lisbon, Portugal.
3 Nephrology Department, Centro Hospitalar Lisboa Ocidental, Lisbon, Portugal.
4 Hematology Department, Centro Hospitalar Lisboa Ocidental, Lisbon, Portugal
ABSTRACT
Monoclonal immunoglobulin deposition disease is part of the spectrum of monoclonal gammopathy of renal significance. We report a case of a light and heavy chain deposition disease treated with anti-plasma cell therapy and peripheral blood stem cell transplantation and over 2 years of follow-up.
Keywords: monoclonal gammopathy, renal disease
INTRODUCTION
Monoclonal immunoglobulin deposition disease (MIDD) is part of the spectrum of monoclonal gammopathy of renal significance (MGRS)1,2. Light and heavy chain deposition disease (LHCDD) is the second most common form of the non-AL amyloid monoclonal immunoglobulin deposition diseases, accounting for 10% of the cases. It occurs primarily in adults at around 60 years of age, presenting with hematuria, nephrotic range proteinuria and reduced glomerular filtration rate.
CASE REPORT
Black male, 58yo, with history of smoking and uncontrolled hypertension, presented at ER with generalized weakness for 3 weeks with no other associated symptoms.
Physical examination was unremarkable except for blood pressure of 172/108 mmHg. No edema.
Bloodwork showed anemia (Hb 10,8g/dL), a serum creatinine of 3.9mg/dl (had ben 1.6 two months earlier), proteins 5.4g/dL, albumin 2.4g/dl; corrected serum calcium 9.4g/dL; serum protein electrophoresis with monoclonal gammopathy IgG Kappa (2.7g/L); serum total light chains kappa and lambda were normal (238mg/dL and 89mg/dL, respectively) with a slightly increased kappa/lambda ratio of 2.674; serum free light chains kappa and lambda were also increased (49.9mg/dL and 100mg/dL, respectively – two and four times the upper limit of the reference range). Bence Jones proteinuria was positive (full immunoglobulin kappa).
Complement, ANA, ds-DNA, ANCA, Anti-GBM, cryoglobulin and viral serologies were normal. Urine had hematuria (++) and proteinuria (++++) with urine protein/creatinine ratio 13g in 24h. Renal ultrasound showed enlarged kidneys compatible with acute medical nephropathy.
A renal biopsy was performed to study a rapidly progressive renal failure with nephrotic range proteinuria and hematuria.
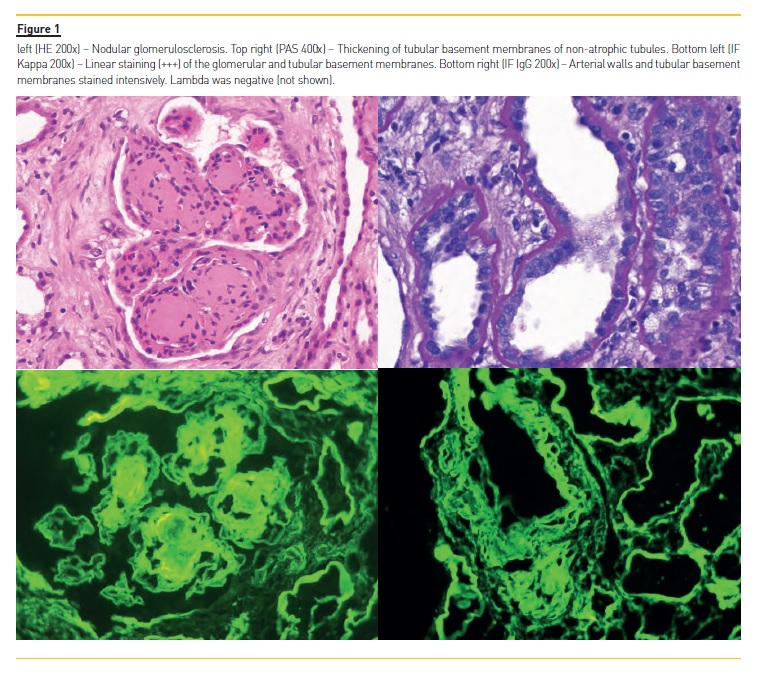
Biopsy showed renal medulla and cortex with 16 glomeruli, 2 (13%) of which were globally sclerotic. The remaining glomeruli were increased in size and cellularity with marked expansion of the mesangium with nodule configuration and thickening of the capillary walls (Figure 1). These nodules were relatively homogenous, stained positive with PAS, negative with silver stain and Congo red.
Tubules showed acute tubular lesions with epithelial simplification, reactive nuclear atypia and loss of brush border. Tubular basement membrane of non-atrophic tubules were thickened. No atypical casts were observed. There was severe interstitial fibrosis and tubular atrophy (around 60%).
There was mild to moderate arterio/arteriolosclerosis.
Immunofluorescence revealed intense linear deposits in the glomeruli, tubular basement membrane and vessel walls for Kappa (+++) and IgG (++). Lambda was negative. IgG subclasses and electron microscopy were not performed.
The diagnosis was light and heavy chain deposition disease (γ - κ LHCDD) with a severe chronicity score (8 out of 10). A complete hematological study was performed. Bone marrow biopsy and flow cytometry were compatible with Monoclonal Gammopathy of Unknown Significance (MGUS) with 5% atypical plasma cells.
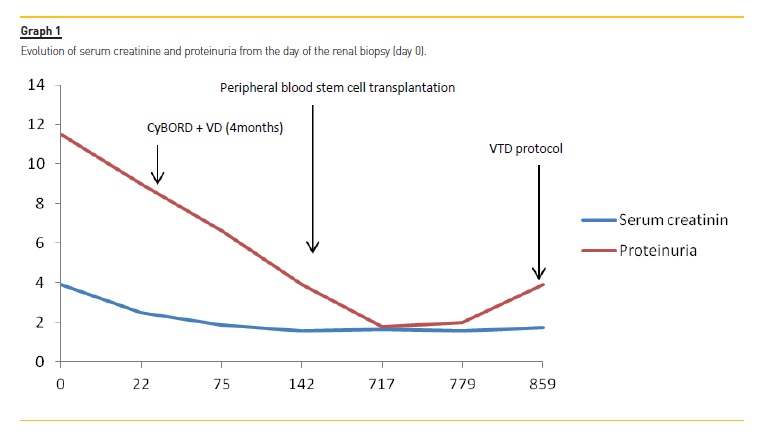
Multiple myeloma, amyloidosis and lymphoma were ruled out and there was no evidence of extrarenal disease. Patient was started on CyBORD protocol (bortezomib, cyclophosphamide, dexamethasone) 22 days after the renal biopsy. He did 4 cycles of CyBORD plus 2 cycles of VD (bortezomib plus dexamethasone) for 4 months with steady improvement of serum creatinine and proteinuria (Graph 1). Patient was then referred to another Institution for tandem autologous stem cell transplantation and achieved a Very Good Partial Response (VGPR). After 2 years of followup, renal function was stable with serum creatinine of 1.73mg/dl, estimated GFR of 41 mL/min/1.73 m2 but proteinuria is back to nephrotic range (3.9g).
Patient was started on second-line VTD protocol (bortezomib, thalidomide, dexamethasone) recently and no data is available since then.
DISCUSSION
A diagnosis of MGRS is suspected in patients with unexplained renal impairment and/or proteinuria who are found to have a monoclonal gammopathy during work-upof the renal disease. In this case, a renal biopsy is usually performed. The presence of monoclonal immunoglobulin deposits in the kidney confirms the diagnosis of MGRS3. A subset of patients with MGRS is diagnosed with LHCDD. It is considered a variant of light chain deposition disease (LCDD) and the morphological aspects on renal biopsy are similar4. The most common pattern is nodular glomerulosclerosis, as seen in this case. The differential diagnosis is with diabetic nephropathy and renal amyloidosis.Immunofluorescence is crucial for diagnosis as it stains for the corresponding monoclonal light and heavy chain, most often γ (the heavy chain of IgG) and κ.
Clinical trials for LHCDD are sparse. Because of the rarity of this disease there is no standard treatment for LCDD. Most recent recommendations suggest targeting the B-cell clone responsible for MGRS, as in multiple myeloma or amyloidosis5. The use of protocols including bortezomib followed or not by autologous stem cell transplantation have induced hematological responses and improvement of renal injury6,7. There are a number of case reports that show that, as in multiple myeloma, immunomodulatory drugs like thalidomide or lenalidomide can be used with success5. We used CyBORD protocol because of the vast experience we have had in our Institution treating patients with multiple myeloma with this protocol. We referred this patient to autologous stem cell transplantation because we felt it was the best option to achieve a prolonged control of the disease. Due to increased proteinuria, he was recently started on VTD – he was on bortezomib more than 2 years ago so we expect that the patient will respond again, and associated thalidomide because it has been shown to induce good responses in these patients. The need of maintenance therapy in this case is debatable.
References
1. Leung N, et al. Monoclonal gammopathy of renal significance: when MGUS is no longer undetermined or insignificant. Blood 2012; 120(22): 4292-4295. [ Links ]
2. Lin J, et al. Renal monoclonal immunoglobulin deposition disease: the disease spectrum. Journal of the American Society of Nephrology 2001; 12(7):1482-1492. [ Links ]
3. Bridoux F, Leung N, Hutchison C, et al. Diagnosis of monoclonal gammopathy of renal significance. Kidney International 2015; 87:698. [ Links ]
4. Jennette JC, et al. Heptinstalls Pathology of the Kidney, Lippincott Williams & Wilkins, 2014:971-973 [ Links ]
5. Royer B, et al. High dose chemotherapy in light chain or light and heavy chain deposition disease. Kidney international 2004; 65(2): 642-648. [ Links ]
6. Jimenez-Zepeda VH. Light chain deposition disease: novel biological insights and treatment advances. International Journal of Laboratory Hematology 2012; 34(4):327-355. [ Links ]
7. Stringaris K, et al. Longterm Outcomes and Improved Renal Function with Autologous Stem Cell Transplantation (ASCT) in Light Chain Deposition Disease (LCDD). Blood 2014; 124:1198. [ Links ]
João Cassis, MD
Pathology Department, Centro Hospitalar Lisboa Ocidental
Lisbon, Portugal
E-mail: joaopcassis@gmail.com
Disclosure of potential conflicts of interest: none declared.
Received for publication: Sep 29, 2017
Accepted in revised form: Apr 30, 2018


{kind=link}
{kind=link}