










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.32 no.1 Lisboa mar. 2018
REVIEW ARTICLE
Diagnosis of monoclonal gammopathy of renal significance
Sofia O Correia, Sofia Santos, La Salete Martins, Josefina Santos
Nephrology and Kidney Transplantation Department, Centro Hospitalar do Porto, Hospital de Santo António.
ABSTRACT
Monoclonal gammopathies are a heterogeneous group of disorders characterized by clonal proliferation of immunoglobulin produced by B-lymphocytes or plasma cell clone. The term monoclonal gammopathy of renal significance (MGRS) was introduced to distinguish monoclonal gammopathies that result in the development of kidney disease from those that are benign. Screening for monoclonal immunoglobulin and an appropriate hematologic workup are fundamental and sometimes a difficult challenge, with therapeutic and prognostic implications. Kidney biopsy is essential to determine the exact nature of the lesion and to evaluate the severity of renal disease. In this review we discuss the clinical and pathologic features of MGRS, highlighting the most diagnostic difficulties and current therapeutic options.
Keywords: Monoclonal gammopathy of renal significance, M protein, renal pathology, treatment.
INTRODUCTION
Monoclonal gammopathies are a heterogeneous group of disorders characterized by clonal proliferation of immunoglobulin produced by B-lymphocytes or plasma cell clone. The spectrum includes the benign condition known as monoclonal gammopathy of undetermined significance (MGUS), low grade lymphoplasmacytic lymphoma with Waldenstroms macroglobulinemia (WM), chronic lymphocytic leukemia (CLL), B-cell lymphoma and multiple myeloma (MM).
MGUS is defined as a plasma cell proliferative disorder with the presence of serum M-protein <3g/dL or < 10% bone marrow clonal plasma cells and it is not associated with end organ damage1. The term monoclonal gammopathy of renal significance (MGRS) was introduced to distinguish monoclonal gammopathies that result in the development of kidney disease from those that are benign2. MGRS do not meet criteria for MM, WM, CLL or malignant lymphoma but can be associated with high morbidity due to renal lesions induced by a monoclonal immunoglobulin (MIg)2.
An incidentally identification of monoclonal gammopathy should be followed by renal evaluation. On the other hand, unexplained proteinuria or renal dysfunction should involve monoclonal protein screening.
The importance of differentiating the term MGRS from other monoclonal gammopathies lies in the fact that diagnostic and therapeutic procedures aimed at controlling monoclonal protein synthesis and secretion can be indicated. Because treatment is not recommended for MGUS, appropriate therapy is commonly withheld but, in MGRS clone-directed therapy is required for disease control and has impact on the outcome.
In this review we discuss the clinical and pathologic features of MGRS, highlighting the most diagnostic difficulties and current therapeutic options.
HEMATOLOGIC EVALUATION
The M protein may consist of a heavy (commonly G, less commonly M, and rarely A, E or D chain) and light chain (either Kappa(κ) or lambda(λ)), light chain only, or less commonly, heavy chain only. The presence of a clonal IgM suggests a B cell or mixed B and plasma cell clone.
M-protein can be traced in the serum and/or urine in almost all patients, but diagnostic approach in MGRS should be sensitive enough to detect small plasma cell and B cell clones.
A complete screening with urine electrophoresis, immunofixation studies and free light-chain assays (FLC) is obligatory even if serum protein electrophoresis (SPEP) studies are negative. In some cases, the MIg levels are very small and may not be detected by EP that is why serum and urine immunofixation is recommended3.
FLC assay suggests clonality by comparing the concentration and ratio of kappa to lambda in the serum, for that matter, it is useful at diagnosis and as indicator of response to treatment4. In case of renal impairment, low renal clearance of polyclonal FLC induces an elevation of FLC kappa (κ) and lambda (λ) levels. Considering a reference range of 0.37-3.17 has been shown to increase diagnostic accuracy5.
To characterize the clone, a detailed hematologic evaluation should be performed with bone marrow aspirate and biopsy with immunohistological studies.
Flow cytometry can detect clonal populations below the limits of immunostaining3,6,7. Computed tomography scan should be performed in patients with high suspicion for lymphoma or in those with monoclonal IgM, in order to identify pathologically involved lymph nodes for a diagnostic biopsy3,6.
CLINICAL, PATHOLOGY AND TREATMENT CONSIDERATIONS
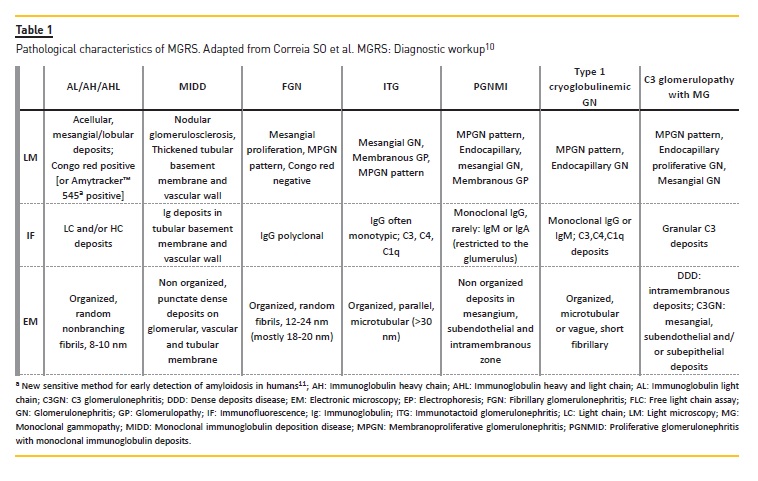
Diagnosis requires integration of clinical parameters, serum and urine analysis, and structural alterations identified by light microscopy, immunofluorescence (IF) and electron microscopy (EM). Anatomopathological characteristics are presented in Table 1. In difficult cases, immunoEM and mass spectrometry may be required to confirm the composition of renal deposits8,9.
The immunoglobulin (Ig) deposits associated to MGRS can be classified into two categories: with organized and with non-organized deposits. MGRS with organized deposits includes Ig related amyloidosis, fibrillar glomerulonephritis, immunotactoid and type I cryoglobulinemic glomerulonephritis. MGRS with nonorganized electro-dense granular deposits includes monoclonal immunoglobulin deposition disease, proliferative glomerulonephritis with monoclonal IgG deposits and C3 glomerulopathy with monoclonal gammopathy.
MGRS also includes tubular disorders such as light chain proximal tubulopathy12.
Most of these disorders are characterized by deposition and precipitation of MIg in the different components of the kidney (glomeruli, vessels, interstitium)13.
MIg can also induce renal injury by dysregulation of the complement pathway14, or by acting like autoantibodies against complement factor or phospholipase A2 receptor15. Other mechanisms are still to be explained.
Treatment is required when symptoms related to the underlying proliferative process are present. No strategy is available in daily practice to inhibit MIg tissue deposition or to clear the already deposited material4. A recent clinical trial with humanized monoclonal
IgG1 anti-serum amyloid P component antibody safely triggered clearance of amyloid deposits from the liver and some other tissues16. Cytotoxic therapy adapted to the underlying clone and renal function has been shown to improve renal outcome and patient survival14,17-19. If a detectable circulating paraprotein is present, response to treatment can be monitor by paraproteins levels (EP, serum and urine immunofixation, FLC).
The agents used to treat MGRS have activity against B cell and plasma cell disorders. The therapeutic regimen chosen should be based on the International Kidney and Monoclonal Gammopathy Working Group consensus4.
Corticosteroids are usually part of these regimens, in monotherapy in cases of mild disease or combined in more severe disease. Bortezomib is a proteasome inhibitor. It can be given at full doses in renal insufficiency and has no renal toxicity. Prophylaxis against herpes zoster reactivation is mandatory20. Cyclophosphamide and melphalan are cytotoxic agents, targeting both plasma cell and B cell. Cyclophosphamide is preferred to melphalan due to its lower toxicity.
Bendamustine, with features from alkylating agents and purine analogs, also has a predominantly nonrenal metabolism and can be given to patients with end stage renal disease (ESRD). Rituximab is a monoclonal antibody directed at CD20, and its use raises no concerns in patients with renal impairment, including ESRD.
RENAL LESIONS ASSOCIATED WITH MGRS
Immunoglobulin related amyloidosis is secondary to the deposition of immunoglobulin (Ig) produced by clonal plasma cells in tissue as amyloid.
AL amyloidosis can be diagnosed if AL deposits can be demonstrated in other tissues such as fat. Microdissection and mass spectrometry can identify the type of renal amyloidosis in more than 97% of cases and can distinguish it from non-amyloid fibrillar glomerulopathy 21,22. A detailed discussion of this pathology goes beyond the scope of this article.
Monoclonal immunoglobulin deposition disease (MIDD) is secondary to deposition of light-chain (κ inmost cases), light and heavy chain, and heavy chain deposition disease13.The deposits lack affinity for Congo red and do not have a fibrillar organization23. Most often presents in the sixth decade, in the presence of renal insufficiency and proteinuria and hypertension24.
Fibrillary glomerulonephritis (FGN) occurs in patients with solid malignancies, autoimmune diseases, and hepatitis C. It is nearly always characterized by polyclonal IgG deposits without a detectable clonal B-cell disorder; the reason it is not considered an MGRS by some groups25,26. Most often presents with proteinuria, 50% within nephrotic range, with or without renal insufficiency, hematuria or hypertension25,26.
Deposits are thicker than amyloid and are Congo red negative26. In a case series report, M-spike was detected by SPEP/immunofixation in only 16% of 61 patients27.
Immunotactoid (microtubular) glomerulopathy (ITG) occurs in an older population and typically presents as a nephrotic syndrome. Cryoglobulinemic GN must be ruled out, because they are difficult to differentiate histopathologically. ITG is associated with an underlying hematologic malignancy such as CLL or small lymphocytic lymphoma, but the association with MGRS is also possible28. Therapeutic choice depends on the underlying disorder. In patients with gammopathy only, the role of rituximab is questionable and bortezomibbased therapy may be considered4.
Proliferative glomerulonephritis with monoclonal IgG Deposits (PGNMID) typically presents with proteinuria,variable degrees of hematuria, renal insufficiencyand hypertension. The diagnosis is established byEM29,30. Some authors are reluctant to recommendchemotherapy in PGNMID with no detectable MIg. Thepresence of an underlying B-cell disorder is suggestedby the presence of monotypic glomerular deposits andthe recurrence after renal transplantation29,31. The InternationalKidney and Monoclonal Gammopathy ResearchGroup recommends chemotherapy (Cyclophosphamideand bortezomib) in patients with stages 1 and 2 CKD andhigh-grade proteinuria (>1 g/day) or progressive disease,and in patients with stages 3 and 4 CKD4.
Cryoglobulinemic glomerulonephritis presents mainly in a membranoproliferative pattern. Type 1 cryoglobulinemia is monoclonal, usually composed of an IgM but can be IgG or IgA, is associate with plasma cell dyscrasias or B-cell lymphoproliferative disorders (multiple myeloma, Waldenstrom macroglobulinemia, chronic lymphocytic leukemia, B-cell non-Hodgkin lymphoma, MGRS, and hairy cell leukemia)32,33.
Type 2 mixed cryoglobulins are composed of an MIg, usually an IgM k with a rheumatoid factor activity, associated with polyclonal immunoglobulin. The most common cause is hepatitis C and in this case antiviral therapy should be given.
In those with vasculitis, antiviral therapy should be combined with rituximab. High-dose steroids are efficient against symptoms but should be avoid in the long term4.
In patients with no detectable viral replication with recurrent symptoms or renal involvement, rituximab is the treatment of choice4. Total plasma exchange should be considered in rapidly progressive renal disease.
Rituximab-containing regimens and bendamustine can be used in all levels of renal dysfunction34.
CONCLUSION
MGRS are associated with a wide range of kidney diseases resulting from the depositions of immunoglobulin or its components in the kidneys, or through the deregulation of the complement system. The likelihood of developing advanced chronic kidney disease is very high, although the mortality of patients with MGRS is lower than that of myeloma or other related gammopathies.
In MGRS, the clinical challenge begins with our ability to identify the underlying clone. So, an evaluation by a multidisciplinary team, that includes nephrologists and hematologists with expertise in this area, is highly recommended. Renal characteristics of the disease, risk of CKD progression, presence and severity of extrarenal manifestations, safety profile of antineoplastic drugs in renal impairment should be all taken into account. After the correct diagnosis and stratification of the disease, the treatment should be instituted based on the International Kidney and Monoclonal Gammopathy Working Group consensus4.
Advances in the understanding of MGRS have made it possible to improve the prognosis of this disease.
References
1. Kyle RA, Durie BG, Rajkumar SV, Landgren O, Blade J, Merlini G, et al. Monoclonal gammopathy of undetermined significance (MGUS) and smoldering (asymptomatic) multiple myeloma: IMWGconsensus perspectives risk factors for progression and guidelines for monitoring and management. Leukemia. 2010;24(6):1121-7. [ Links ]
2. Leung N, Bridoux F, Hutchison CA, Nasr SH, Cockwell P, Fermand J, et al. Monoclonal gammopathy of renal significance: when MGUS is no longer undetermined or insignificant. Blood. 2012;120(22):4292-6. [ Links ]
3. Bridoux F, Leung N, Hutchison CA, Touchard G, Sethi S, Fermand JP, et al. Diagnosis of monoclonal gammopathy of renal significance. Kidney Int. 2015; 87: 698-711. [ Links ]
4. Fermand JP, Bridoux F, Kyle RA, Kastritis E, Weiss BM, Cook MA, Drayson MT, Dispenzieri A, Leung N; International Kidney and Monoclonal Gammopathy Research Group. How I treat monoclonal gammopathy of renal significance (MGRS). Blood. 2013;122:3583-3. [ Links ]
5. Hutchison CA, Plant T, Drayson M, Cockwell P, Kountouri M, Basnayake K, et al. Serum free light chain measurement aids the diagnosis of myeloma in patients with severe renal failure. BMC Nephrol. 2008;9:11. [ Links ]
6. Hogan JJ, Weiss BM. Bridging the Divide: An onco-nephrologic approach to the monoclonal gammopathies of renal significance. Clin J Am Soc Nephrol. 2016; 11:1681-91. [ Links ]
7. Landgren O, Gormley N, Turley D, Owen RG, Rawstron A, Paiva B, et al. Flow cytometry detection of minimal residual disease in multiple myeloma: Lessons learned at FDA-NCI roundtable symposium. Am J Hematol. 2014; 89(12): 1159-60. [ Links ]
8. Royal V, Quint P, Leblanc M, Leblanc R, Duncanson GF, Perrizo RL, et al. IgD heavy-chain deposition disease : detection by laser microdissection and mass spectrometry. J Am Soc Nephrol. 2015;784-90. [ Links ]
9. Sanjeev Sethi, Julie A Vrana, Jason D Theis, Nelson Leung, Anjali Sethi, Samih H Nasr, Fernando C Fervenza, Lynn D Cornell, Mary E Fidler and AD. Laser microdissection and mass spectrometry-based proteomics aids the diagnosis and typing of renal amyloidosis. Kidney Int. 2012; 82(2):226-34. [ Links ]
10. Correia SO, Santos S, Malheiro J, Cabrita A, Martins LS, Santos J. Monoclonal gammopathy of renal significance: Diagnostic workup. World J Nephrol. 2017;6(2):72-8. [ Links ]
11. Sjölander D, Röcken C, Westermark P, Westermark GT, Nilsson KPR, Hammarström P. Establishing the fluorescent amyloid ligand h-FTAA for studying human tissues with systemic and localized amyloid. Amyloid. 2016; 23:98-108. [ Links ]
12. Sethi S, Fervenza FC, Rajkumar SV. Spectrum of manifestations of monoclonal gammopathy- associated renal lesions. Curr Opin Nephrol Hypertens. 2016;25(2):127-37. [ Links ]
13. Lin J, Markowitz GS, Valeri AM, Kambham N, Sherman WH, Appel GB, et al. Renal monoclonal immunoglobulin deposition disease : the disease spectrum. J Am Soc Nephrol. 2001;1482-92. [ Links ]
14. Zand L, Kattah A, Fervenza FC, Smith RJH, Nasr SH, Zhang Y, et al. C3 glomerulonephritis associated with monoclonal gammopathy: a case series. Am J Kidney Dis. 2013;62(3):506-14. [ Links ]
15. Debiec H, Hanoy M, Francois A, Guerrot D, Ferlicot S, Johanet C, et al. Recurrent membranous nephropathy in an allograft caused by IgG3 k targeting the PLA2 receptor. 2012;1949-54.
16. Richards DB, Cookson LM, Berges AC, Barton SV, Lane T, Ritter JM, et al. Therapeutic clearance of amyloid by antibodies to serum amyloid P component. N Engl J Med. 2015; 373:1106-14. [ Links ]
17. Chauvet S, Frémeaux-Bacchi V, Petitprez F, Karras A, Daniel L, Burtey S, et al. Treatment of B-cell disorder improves renal outcome of patients with monoclonal gammopathyassociated C3 glomerulopathy. Blood. 2017;129(11):1437-47. [ Links ]
18. Leung N, Dispenzieri A, Fervenza FC, Lacy MQ, Villicana R, Cavalcante JL, et al. Renal response after high-dose melphalan and stem cell transplantation is a favorable marker in patients With primary systemic amyloidosis. Am J Kidney Dis. 2005;46(2):270-7. [ Links ]
19. Leung N, Drosou ME, Nasr SH. Dysproteinemias and glomerular disease. Clin J Am Soc Nephrol. 2017; 13(1):128-39. [ Links ]
20. Chanan-Khan AA, Kaufman JL, Mehta J, Richardson PG, Miller KC, Lonial S, et al. Activity and safety of bortezomib in multiple myeloma patients with advanced renal failure: a multicenter retrospective study. Blood. 2007;109(6):2604-6. [ Links ]
21. Nasr SH, Said SM, Valeri AM, Sethi S, Fidler ME, Cornell LD, et al. The diagnosis and characteristics of renal heavy-chain and heavy/light-chain amyloidosis and their comparison with renal light-chain amyloidosis. Kidney Int. 2013; 83(3):463-70. [ Links ]
22. Sethi S, Theis JD, Leung N, Dispenzieri A, Nasr SH, Fidler ME, et al. Mass spectrometrybased proteomic diagnosis of renal immunoglobulin heavy chain amyloidosis. Clin J Am Soc Nephrol. 2010;2180-7. [ Links ]
23. Sanders PW, Herrera GA. Monoclonal immunoglobulin light chain-related renal diseases. Semin Nephrol. 1993; 13(3):324-41. [ Links ]
24. Nasr SH, Valeri AM, Cornell LD, Fidler ME, Sethi S, Agati VDD, et al. Article renal monoclonal immunoglobulin deposition disease: a report of 64 patients from a single institution. Clin J Am Soc Nephrol. 2012; (1):231-9. [ Links ]
25. Rosenstock JL, Markowitz GS, Valeri AM et al. Fibrillary and immunotactoid glomerulonephritis: distinct entities with different clinical and pathologic features. 2003; 63:1450-61.
26. Bridoux F, Hugue V, Coldefy O et al. Fibrillary glomerulonephritis and immunotactoid (microtubular) glomerulopathy are associated with distinct immunologic features. 2002; 62:1764-75.
27. Nasr SH, Valeri AM, Cornell LD, Fidler ME, Sethi S, Leung N. Fibrillary glomerulonephritis: a report of 66 cases from a single institution. 2011; 775-84.
28. Nasr SH, Fidler ME, Cornell LD, Leung N, Cosio FG, Sheikh SS, et al. Immunotactoid glomerulopathy: clinicopathologic and proteomic study. 2012; 27(11):4137-46.
29. Nasr SH, Satoskar A, Markowitz GS, Valeri AM, Appel GB, Stokes MB, et al. Proliferative glomerulonephritis with monoclonal IgG deposits. J Am Soc Nephrol. 2009; 20(9):2055-64. [ Links ]
30 Bhutani G, Nasr SH, Said SM, Sethi S, Fervenza FC, Morice WG, et al. Hematologic characteristics of proliferative glomerulonephritides with nonorganized monoclonal immunoglobulin deposits. Mayo Clin Proc. 2016; 90(5):587-96. [ Links ]
31. Nasr SH, Sethi S, Cornell LD, Fidler ME, Boelkins M, Fervenza FC, et al. Proliferative glomerulonephritis with monoclonal IgG deposits recurs in the allograft. Clin J Am Soc Nephrol. 2011; 6(1):122-32. [ Links ]
32. Terrier B, Karras A, Kahn J, Guenno G Le, Marie I, Benarous L, et al. The spectrum of type I cryoglobulinemia vasculitis. 2013; 92(2):61-8.
33. Nasr SH, Markowitz GS, Reddy BS, Maesaka J, Swidler MA, Agati VDD. Dysproteinemia, proteinuria, and glomerulonephritis. Kidney Int. 2006; 69(4):772-5. [ Links ]
34. Terrier B, Krastinova E, Marie I, Launay D, Lacraz A, Belenotti P, et al. Management of noninfectious mixed cryoglobulinemia vasculitis: data from 242 cases included in the CryoVas survey. Blood. 2012; 119(25):5996-6004. [ Links ]
Josefina Santos, MD
Nephrology and Transplant Department, Centro Hospitalar do Porto,
4099-001, Porto, Portugal
E-mail: josefina.sts@gmail.com
Disclosure of potential conflicts of interest: None declared
Received for publication: Jan 29, 2018
Accepted in revised form: Mar 14, 2018


{kind=link}