










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.32 no.1 Lisboa mar. 2018
ORIGINAL ARTICLE
Hemodialysis arteriovenous fistula outcomes in elderly patients: a single‑centre cohort
Hugo Ferreira1, Hugo Diniz1, Patrícia Martins1,2,3, Luís Coentrão2,3
1Nephrology Department, Centro Hospitalar de São João
2Nephrology and Infectious Diseases Research and Development Group, INEB‑I3S)
3 Faculdade de Medicina da Universidade do Porto
ABSTRACT
The cohort of older age pre‑dialysis patients is growing steadily. However, Fistula First may not always be the best strategy due to poorer arteriovenous fistula outcomes in this population.
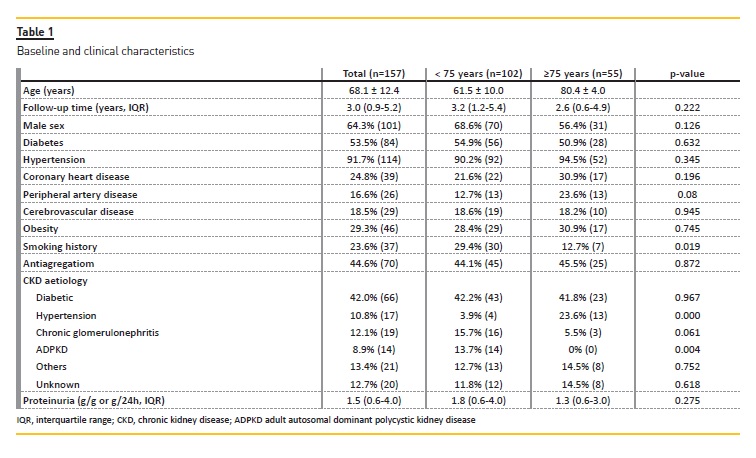
This retrospective cohort study included data from 157 predialysis patients who underwent fistula placement in our centre. Their mean age was 68.1±12.4 years. 64.3% were male and 53.5% were diabetic. The median nephrology follow‑up was 3.04 years (IQR: 0.95–5.17). Two groups were created based on patients age at fistula placement: <75 years (n=102) and ≥75 years (n=55).
Further analysis is shown, for the younger group vs. the elderly group, respectively. The groups differed only in smoking history (29.4% versus 12.7%, p=0.019) and in hypertensive (3.9% versus 23.6%, p<0.001) and autosomal dominant polycystic kidney disease aetiologies (13.7% versus 0%, p=0.004). Mean estimated glomerular filtration rate at referral for fistula placement was 16.1±4.3 vs. 14.5±4.0ml/min/1.73m2 (p=0.026). Primary fistula failure occurred in 17.6% vs. 32.7%, p=0.032 (RR 1.85 [1.05–3.26]): in 4.9% vs. 5.5% due to thrombosis (p=0.881), in 12.7% vs. 25.5% due to maturation failure (p=0.044; RR 2.0 [1.01–3,94]) and in 2.0% vs. 1.8% due to complications which lead to surgical closure (p=1). During the follow‑up period, 52.0% vs. 43.6% patients started hemodialysis (p=0.32). Of these patients, 79.2% vs. 50.0% started hemodialysis with a functioning fistula, p=0.009 (RR 0.63 [0.41–0.96]) while the remaining needed a central venous catheter (RR 2.41 [1.24–4.67]). In multivariate analysis, age ≥75 years and the number of previous fistulawere predictors of failure: OR 3.70 (CI: 1.37–9.98) and 11.65 (CI: 5.04–26.93), respectively.
In conclusion, elderly patients had more primary fistula failure. The need of central venous catheter due to non‑functioning fistula at time of dialysis initiation was higher in the elderly. Older age (≥ 75 years) and the number of previously placed fistulas seem to predict fistula failure.
Key‑words: Arteriovenous fistula; hemodialysis; elderly.
INTRODUCTION
The number of elderly patients receiving hemodialysis (HD) has risen steadily in the last decades1,2.
International guidelines recommend the placement of an arteriovenous fistula (AVF) in all chronic kidney disease (CKD) patients expected to initiate HD, due to better patient and access related outcomes3,4. However, this may not always be the best strategy for the elderly, due to a higher prevalence of comorbidities that contribute to AVF failure5.
This study aimed to assess if elders at our center have poorer AVF‑ related outcomes than younger counterparts.
MATERIAL AND METHODS
Population, data source and variables
The study population consisted of patients who underwent AVF placement (first or subsequent) from January 2014 to February 2015 in Centro Hospitalar de São João, Porto, Portugal. A total of 157 patients were included. Data were collected from electronic clinical charts. Clinical variables such as previous medical conditions were considered to exist if the diagnosis was mentioned in patients clinical charts. Smoking history was defined as current or former smoking habits. Estimated glomerular filtration rate (eGFR) was calculated using the CKD‑EPI formula.
Study design
This is a retrospective cohort study. For comparison purposes, we divided our patients into two groups, according to their age at AVF placement: < 75 years and ≥ 75 years (study group). Patients were followed during a 24 month‑period or until death or HD initiation.
Statistical analysis
The baseline and clinical variables are reported in average and standard deviation for normally distributed continuous variables, median and interquartile range (IQR) for non‑normally distributed continuous variables, frequencies, and percentages for categorical variables.
The differences between groups were tested using student t‑test, Mann‑Whitney U, and chi‑square, respectively. To compare groups, we calculated relative risks (RR) and 95% confidence intervals (95% CI). Binary logistic regression was used to assess predictors of AVF failure in the whole cohort. All assumed logistic regression was checked and met. All variables with a p level lower than 0.10 in the univariate analysis were included in the multivariate model entry. Then, a method of stepwise backward deletion was applied, in which, after being evaluated one at a time, those variables that did not contribute significantly (less than 10% modification of odds ratio) were deleted from the model.
Statistical significance was defined as p < 0.05. The statistical software package utilized was SPSS 23.0.0.0.
RESULTS
A total of 157 patients underwent AVF placement. Their mean age was 68.1 ± 12.4 years; 101 patients were male (64.3%); two were black (1.3%); 84 had diabetes (53.5%), and the most common CKD aetiology was diabetic nephropathy (42%). The median follow‑up duration by a nephrologist was 3.04 years (IQR: 0.95–5.17) and the mean eGFR at referral for AVF placement was 15.6 ± 4.3ml/min/1.73m2. One hundred and eleven patients were placing their first AVF (70.7%); 35 the second (22.3%), and 11 the third or fourth (7%); data about previous AVF type is not described due to missing information in many patients. Seventy‑seven patients placed a distal AVF (49%). Table 1.
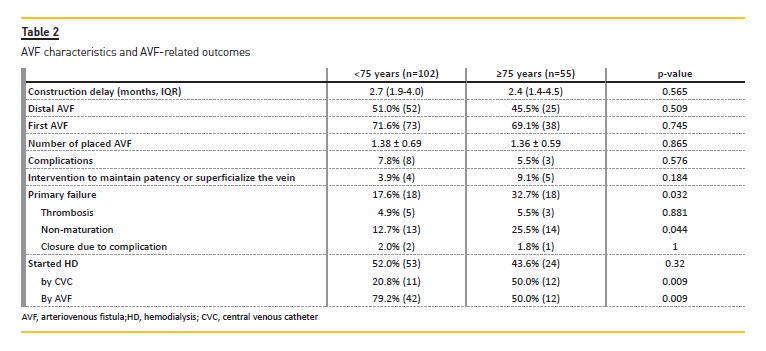
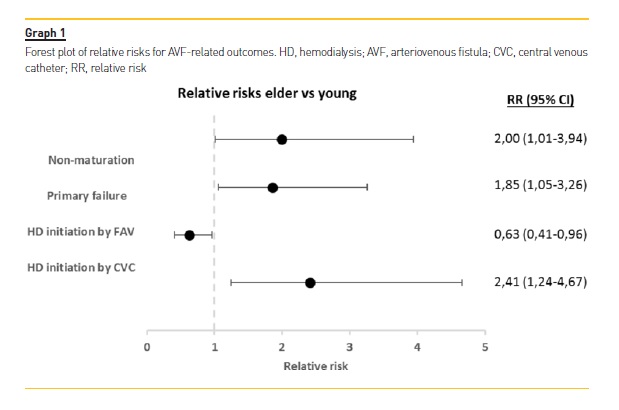
Further analysis is shown, for younger group (n=102) vs. elderly group (n=55), respectively. There were no differences in baseline characteristics between groups, besides smoking history (29.4% vs. 12.7%, p=0.019), hypertensive CKD aetiology (3.9% vs. 23.6%, p<0.001) and autosomal dominant polycystic kidney disease CKD aetiology (13.7% vs. 0%, p=0.004). Mean eGFR at referral for AVF placement was 16.1 ± 4.3 vs. 14.5 ± 4.0 ml/min/1.73m2 (p=0.026) and the median delay from referral to AVF construction was 2.7 (IQR: 1.9–4,0) vs. 2.4 months (IQR: 1.4–4.5), p=0.565. Table 1. The majority placed their first AVF during the follow‑up period (71.6% vs. 69.1%, p=0.745). Radiocephalic AVF type was placed in 51.0% vs. 45.5%, p=0.509. Primary AVF failure occurred in 17.6% vs. 32.7%, p=0.032 (RR 1.85 [1.05‑3,26]): in 4.9% vs. 5.5% due to thrombosis (p=0.881), in 12.7% vs. 25.5% due to maturation failure (p=0.044; RR 2.0 [1.01–3,94]) and in 2.0% vs. 1.8% due to complications which led to surgical closure (p=1). Table 2 and Graph 1.
During the follow‑up period 52.0% vs. 43.6% patients started HD in each group, p=0.32. Of these patients, 79.2% vs. 50.0% initiated HD with a functioning AVF, p=0.009 (RR 0.63 [0.41–0,96]) while the remaining needed a central venous catheter (CVC) (RR 2.41 [1.24– 4.67]). Complication rates (7.8% vs. 5.5%, p=0.576), need for intervention to maintain patency or to superficialize the vein (3.9% vs. 9.1%, p=0.184) were similar in both groups. Table 2 and Graph 1.
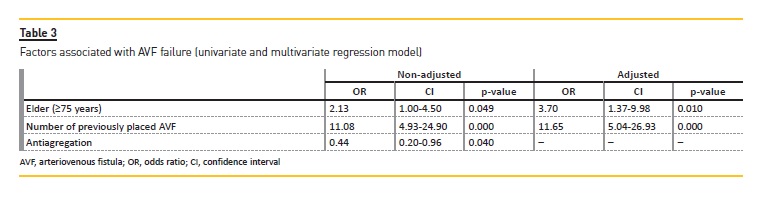
Finally, to assess factors associated with AVF failure, we performed univariate and multivariate logistic regression, Table 3. In univariate analysis, age ≥ 75, anti‑aggregation (protective) and the number of previously placed AVF achieved statistical significance. Older age (≥ 75 years) and the number of previous placed AVF were predictors of failure in the final multivariate model (r square=0.312): odds ratio (OR) 3.70 (CI: 1.37–9,98) and OR 11.65 (CI: 5.04–26.93), respectively.
DISCUSSION
As elderly patients are the fastest growing CKD group1,2, it is vital to recognize if these patients need a different strategy for renal replacement therapy preparation, particularly in terms of vascular access creation. These patients may have a poorer vascular capital due to a higher prevalence of co‑morbidities and repeated vein cannulation, which may lead to a higher rate of AVF non‑maturation and failure. Additionally, mortality is a clear competitive risk to HD initiation which may result in unnecessary interventions in this population6. In the last decade, there is growing evidence supporting that elderly CKD patients need a different vascular access placement strategy.
In our study, we found poorer AVF related outcomes in older predialysis CKD patients. Our cohort represents the reality of CKD outpatient clinics with over one‑third of the patients being 75 years or older. There was a high prevalence of proximal AVF in both groups (younger=49.0% vs. elder=64.5%, p=0.509) and the majority underwent their first AVF placement (younger=71.6% vs. elder=69.1%, p=0.745). This may reflect that in our cohort younger patients were as suitable for proximal AVF as elder counterparts, but it may also reflect our vascular surgeons preference in AVF placement location.
However, despite the similarities in AVF type and number, there were worse AVF patency rates in the elder group. These patients had a higher chance of AVF primary failure, RR 1.85 (1.05–3,26) with a higher risk of non‑maturation (RR 2.0 [1.01–3,94]). These findings are consistent with previous studies that have shown a similar OR for failure in older patients compared to younger counterparts7-9. In accordance, elderly patients had a higher risk of a non‑functioning AVF at time of HD initiation, RR 2.41 (1.24–4.67). There was not a higher prevalence of AVF related complication in elderly patients, namely hemodialysis access‑induced distal ischemia, as shown in previous studies10. Smoking history was more common in the younger group and this could have led to worst AVF outcomes due to peripheral artery disease. However, autosomal dominant polycystic kidney disease (that normally represents healthier patients without significant comorbidities) was also more common in this group. On the other hand, hypertensive CKD aetiology was more common in the elderly group, probably representing longstanding cardiovascular and atherosclerotic diseases and poorer vascular capital, leading to worst AVF survival in this group.
We performed a second analysis to assess other risk factors for AVF failure besides age and overcome potential confounders. Anti‑aggregation was a protective factor for failure but only in the univariate analysis.
Surprisingly, diabetes was not a relevant predictor of AVF failure in the univariate analysis. Only age (≥75 years) and the number of previous placed AVF stand as predictors of AVF failure in multivariate analysis, OR 3.70 (CI: 1.37‑9.98) and OR 11.65 (CI: 5.04‑26.93), respectively. Although female sex, diabetes, peripheral artery disease, and obesity have been associated with AVF failure11 they did not constitute risk factors in our cohort.
In summary, our results showed that patients above 74 years old have a higher chance of having primary AVF failure. For instance, an elderly patient with one failed attempt of AVF placement, the OR for failure would be higher than 15. When considering all patients, age is also a predictor of AVF failure, which has been reported in many other studies11-13. Hence, the benefits of creating an AVF in the elderly may not be as high as in younger patients. As in many other issues in nephrology, again, it seems that one size does not fit all.
Nevertheless, no guidelines are making a different recommendation in this age group. In fact, elderly patients appear to have less risk of CVC related bloodstream infection (CRBI) than younger counterparts, which is a key‑point of AVF over CVC preference. In a recent study, Murea M. and colleagues showed that HD patients ≥ 75 years old have an incidence of CRBI of 0.55 per 1000 CVC days compared with 1.97 in the nonelderly (hazard ratio of 0.33)14. However, the risk of bloodstream infection is undeniable higher with CVC, and its placement may be kept, for instance, to patients with short life expectancy who still benefit with HD initiation or to elderly patients with deplorable vascular conditions (such as diffuse peripheral arterial disease).
The classical intermediate solution in vascular access is the placement of arteriovenous grafts (AVG). They seem to not confer a mortality disadvantage compared with AVF in the elderly population15,16, particularly in patients with high comorbidities burden and poor life expectation17. A recent work highlighted a critical point regarding this issue: the survival advantage conferred by AVF placement in the elderly appears to be surrogate of healthier individuals where AVF are more likely to be placed than an actual survival benefit of AVF itself18.
For elderly CKD patients, it is difficult to have a golden rule as the fistula first policy advises. In our opinion, this is a field where individualized care must take place. Patients characteristics, preferences and life expectancy should be taken into account for the decision of vascular access placement in this particular CKD population.
This study has some limitations that should be acknowledged. The main one comes from its single‑centre, retrospective design and its relatively small number of patients. Lastly, based on the relatively small sample size of our cohort, the study was likely underpowered to detect all the risk factors and the impact of every clinical characteristic on AVF outcomes.
In conclusion, elderly patients had poorer AVF survival with more primary AVF failure, even with a high prevalence of proximal AVF. The need for CVC due to non‑functioning AVF, at time of HD initiation, was also higher in the elderly. Older age (≥ 75 years) and the number of previously placed AVF seem to predict AVF failure. Only about a quarter of our elderly patients benefited from vascular access construction. This means that better predictors of CKD progression are needed to guide proper referral for vascular access.
Also, to enhance the probability of success, vascular mapping before AVF placement is probably even more critical in the elderly. Also, survival advantage and better access related outcomes with AVF are not straightforward in the elderly CKD population – individualization of the arteriovenous access, taking into account not only the patients age but also his/her CKD aetiology, comorbidities and life expectancy, may be the best strategy.
References
1. Canaud B, Tong L, Tentori F, Akiba T, Karaboyas A, Gillespie B, et al. Clinical practices and outcomes in elderly hemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin J Am Soc Nephrol CJASN. 2011;6(7):1651-62. [ Links ]
2. Vachharajani TJ, Moist LM, Glickman MH, Vazquez MA, Polkinghorne KR, Lok CE, et al. Elderly patients with CKD–dilemmas in dialysis therapy and vascular access. Nat Rev Nephrol. 2014;10(2):116-22. [ Links ]
3. Vascular Access Work Group. Clinical practice guidelines for vascular access. Am J Kidney Dis Off J Natl Kidney Found. 2006;48(1):S248-73. [ Links ]
4. Tordoir J, Canaud B, Haage P, Konner K, Basci A, Fouque D, et al. EBPG on Vascular Access. Nephrol Dial Transplant. 2007;22(2):ii88-ii117. [ Links ]
5. Ferreira H, Coentrao L. Vascular access for elderly hemodialysis patients: what should we aim for? J Vasc Access. 2016;17(1):S38-41. [ Links ]
6. Masengu A, Hanko JB, Maxwell AP. Optimizing outcomes in the elderly with end‑stage renal disease–live long and prosper. J Vasc Access. 2015;16(6):439-45. [ Links ]
7. Lok CE, Allon M, Moist L, Oliver MJ, Shah H, Zimmerman D. Risk equation determining unsuccessful cannulation events and failure to maturation in arteriovenous fistulas (REDUCE FTM I). J Am Soc Nephrol JASN. 2006;17(11):3204-12. [ Links ]
8. Lazarides MK, Georgiadis GS, Antoniou GA, Staramos DN. A meta‑analysis of dialysis access outcome in elderly patients. J Vasc Surg. 2007;45(2):420-6. [ Links ]
9. Lok CE, Oliver MJ, Su J, Bhola C, Hannigan N, Jassal SV. Arteriovenous fistula outcomes in the era of the elderly dialysis population. Kidney Int. 2005;67(6):2462-9. [ Links ]
10. Sen I, Tripathi RK. Dialysis access‑associated steal syndromes. Semin Vasc Surg. 2016;29(4):212-26. [ Links ]
11. Ethier J, Mendelssohn DC, Elder SJ, Hasegawa T, Akizawa T, Akiba T, et al. Vascular access use and outcomes: an international perspective from the Dialysis Outcomes and Practice Patterns Study. Nephrol Dial Transplant. 2008;23(10):3219-26. [ Links ]
12. Monroy‑Cuadros M, Yilmaz S, Salazar‑Banuelos A, Doig C. Risk factors associated with patency loss of hemodialysis vascular access within 6 months. Clin J Am Soc Nephrol CJASN. 2010;5(10):1787-92. [ Links ]
13. Hayakawa K, Miyakawa S, Hoshinaga K, Hata K, Marumo K, Hata M. The effect of patient age and other factors on the maintenance of permanent hemodialysis vascular access. Ther Apher Dial Off Peer‑Rev J Int Soc Apher Jpn Soc Apher Jpn Soc Dial Ther. 2007;11(1):36-41. [ Links ]
14. Murea M, James KM, Russell GB, Byrum GV, Yates JE, Tuttle NS, et al. Risk of catheter‑related bloodstream infection in elderly patients on hemodialysis. Clin J Am Soc Nephrol CJASN. 2014;9(4):764-70. [ Links ]
15. DeSilva RN, Patibandla BK, Vin Y, Narra A, Chawla V, Brown RS, et al. Fistula first is not always the best strategy for the elderly. J Am Soc Nephrol JASN. 2013;24(8):1297-304. [ Links ]
16. Chan MR, Sanchez RJ, Young HN, Yevzlin AS. Vascular access outcomes in the elderly hemodialysis population: A USRDS study. Semin Dial. 2007;20(6):606-10. [ Links ]
17. Murea M, Satko S. Looking Beyond Fistula First in the Elderly on Hemodialysis. Semin Dial. 2016;29(5):396-402. [ Links ]
18. Quinn RR, Oliver MJ, Devoe D, Poinen K, Kabani R, Kamar F, et al. The effect of predialysis fistula attempt on risk of all‑cause and access‑related death. J Am Soc Nephrol JASN. 2017;28(2):613-20. [ Links ]
Hugo Ferreira, MD
Nephrology Department, Centro Hospitalar de São João;
Alameda Prof. Hernâni Monteiro, 4200–319 Porto. Portugal
E‑mail: ferreihugo@gmail.com
Disclosure of potential conflicts of interest: none declared.
Received for publication: 20 Sep 2017
Accepted in revised form: 24 Jan, 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}