










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.31 no.3 Lisboa set. 2017
ORIGINAL ARTICLE
Predialysis vascular access creation: To whom and when
Rachele Escoli, Ivan Luz, Paulo Santos, Ana Vila Lobos
Nephrology Department, Centro Hospitalar do Médio Tejo, Torres Novas, Portugal
ABSTRACT
Aims: The optimal timing of predialysis vascular access surgery remains uncertain. This study goal was to evaluate the influence of kidney function and clinical characteristics at predialysis vascular access surgery on the likelihood of initiating hemodialysis during follow-up. Methods: Our study retrospectively identified all patients undergoing predialysis arteriovenous fistula creation between 2012–2015. We assessed 3 outcomes: frequency of hemodialysis initiation, death before hemodialysis initiation, and dialysis-free survival after vascular access creation. Multiple variable logistic regression analyzed which factors predicted initiation of dialysis. Results: The study involved 202 patients. Using multiple variable logistic regression, 5 factors were associated with hemodialysis initiation: estimated glomerular filtration rate <10 mL/min/1,73m2 at vascular access placement [OR 4.7, CI: 1.98-8,60, p=0.005], diabetes [OR 2.14, CI: 1.07–4,30, p=0.033], proteinuria>1gr/24 hours [OR 1.88, CI: 0.95–3.71, p=0.049], higher phosphorus levels [OR 6.25, CI: 1.39–13.05, p=0.017] and glomerular filtration rate drop ³3mL/min/1.73m2 in the year preceding vascular surgery [OR 1.67, CI: 0.81–3.45, p=0.016]. Cancer and congestive heart failure were associated with dead before starting dialysis [OR 5.9, CI: 1.15–9.78, p=0.038 and OR 2.4, CI: 1.3–3.9, p=0.021, respectively] and higher hemoglobin (>10g/dL) without erythropoietin stimulating agent levels with survival without needing dialysis [OR 2.34, CI: 1.09-4,58, p=0.028]. Conclusions: Optimizing the timing of vascular access creation in predialysis patients requires consideration not only of the kidney function but also comorbidities such as diabetes, estimated glomerular filtration rate decline in the preceding year and degree of proteinuria.
Key Words: Arteriovenous fistula; Chronic Hemodialysis; Pre-dialysis; Vascular Access
INTRODUCTION
Creating a permanent vascular access (VA) is a significant management step in the clinical pathway of patients with progressive chronic kidney disease (CKD)1 who should be referred early to the nephrologist and vascular surgeon to allow sufficient time for education, planning, access creation and maturation2. However, the optimal timing of predialysis vascular access surgery remains uncertain3. Although clinical practice guidelines are unified recommending native arteriovenous fistula (AVF) as the first vascular access choice for hemodialysis (HD), the majority of patients throughout the Western world commence hemodialysis with a central venous catheter1. Vascular access placement guidelines are not unanimous. European Best Practice Guideline recommend that potential chronic HD patients should be ideally referred to the nephrologist and/or surgeon they reach CKD stage 4 or earlier in case of rapidly progressive nephropathy or specific clinical conditions such as diabetes or severe peripheral vascular disease4. British Guidelines suggest that the exact timing of VA placement will be determined by rate of decline of renal function, co-morbidities and by the surgical pathway5.
Instead, Canadian guidelines propose that VA placement should be stablished when the patient has an estimated GFR of 15 to 20 ml/min and progressive kidney disease6. Taking into account the heterogeneity of the recommendations, this study aimed to study the influence not only of the of the kidney function but also clinical characteristics at the time of pre-end stage renal disease VA surgery on the likelihood of initiating dialysis during 1 year-follow-up.
MATERIAL AND METHODS
Data collection
We retrospectively identified all predialysis VA placed from January 1, 2012 to December 31, 2015 in a district hospital. During this period 202 patients with CKD underwent predialysis AV surgery. Each patients medical record was reviewed to collet demographic and clinical information. The eGFR was calculated using the CKD-EPI formula and the trajectory was estimated from the difference between the eGFR one year before the VA construction and the eGFR at the moment of the vascular access placement. Proteinuria was obtained in the 24-hour urine collection (correction of the 24-hour urine collection was not made in this study).
Blood pressure (BP) control was estimated using the first preoperative systolic BP obtained on the VA surgery date. The study had a one-year follow-up. Patients with previous renal replacement therapy, duplicate entries, missing follow-up data and patients younger than 18 years old were excluded.
Statistical Analysis
Baseline patient characteristics were compared between eGFR groups using chi-squared tests for categorical variables, and t-student for continuous variables.
Multiple variable logistic regression analyzed which demographic and clinical factors predicted initiation of dialysis. P values < 0.05 were considered statistically significant. All statistical analysis was performed using SPSS.
RESULTS
Patient Characteristics
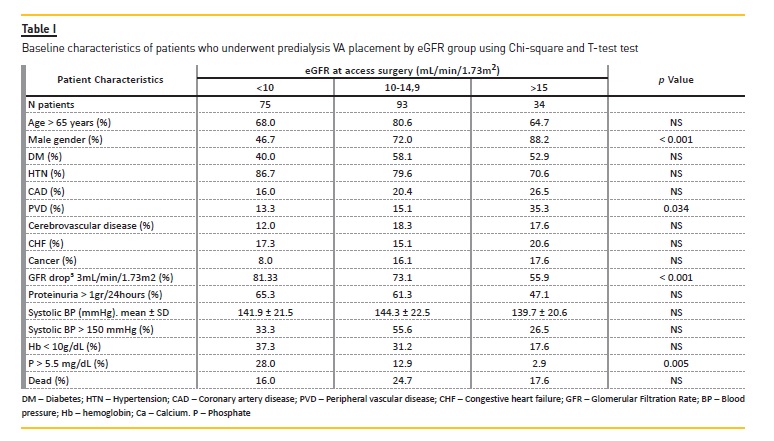
The study cohort involved 202 patients with CKD who underwent predialysis AV placement during a 4-year period. The average age was 70.2 ± 13.7 years, 132 (65.3%) were male and 150 (74.3%) started hemodialysis in an average period of 8.1 ± 7.9 months. The patients were divided into three cohorts on the basis of their eGFR values at the time of surgery (Table I).
Concerning patient characteristics, only male gender, peripheral vascular disease, GFR drop ³ 3mL/min/1.73m2 in the preceding year and higher phosphorus levels differed significantly among the three cohorts. Age, diabetes, hypertension, cerebrovascular disease, congestive heart failure, coronary artery disease, cancer, previous nephrology follow-up and systolic BP were similar in the three groups.
Likelihood of HD initiation, die before starting dialysis and being dialysis free after VA placement
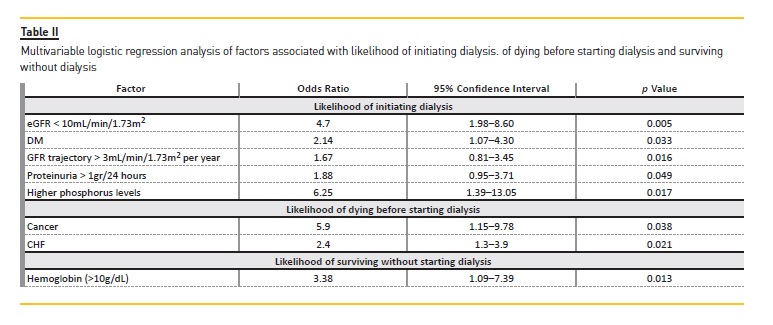
Overall, 150 patients (74%) started hemodialysis; 12 (6%) died before starting dialysis and 40 (20%) were dialysis-free during 1-year of follow-up. Using multiple variable logistic regression, five factors were associated with hemodialysis initiation: the group with the GFR <10 mL/min/1,73m2 at VA creation showed 4.7-fold greater probability of starting dialysis. Also, diabetes, proteinuria >1gr/24 hours, higher phosphorus levels and GFR drop ³3mL/min/1.73m2 in the year preceding vascular surgery were associated with hemodialysis initiation. Cancer and congestive heart failure were associated with dead before starting dialysis. Higher hemoglobin (>10g/dL) without erythropoietin stimulating agents (ESA) levels associated with survival without dialysis (Table II).
DISCUSSION
Selection of the optimal eGFR for access surgery requires finding the optimal balance between placing the access too early or placing it too late3. VA guidelines are not peremptory. Most of them are opinion based, and propose various eGFR thresholds for referral a patient with CKD to the surgeon for access creation6-8. The European guidelines of Vascular Access Society promote that a VA planning should commence when the patient reaches CKD stage 4. A systematic review did not identify any randomized controlled clinical trials investigating whether early referral to prepare for dialysis had any advantage over late referral. However, being referred earlier to a nephrologist resulted in a reduction in mortality and hospitalization, a higher uptake of peritoneal dialysis, a decreased likelihood of requiring temporary vascular access at the start of dialysis and increased likelihood of having an AVF9.
In this study, we suggest that eGFR by itself is a relatively poor predictor to define the timing to start dialysis and therefore the optimal timing of a VA construction may need to take into account not only kidney function but also, other clinical variables. The predictive value of diabetes and magnitude of proteinuria that was pointed out in our study agrees with the observation that CKD progresses faster in patients with diabetes and those with more proteinuria10.
A prospective, population-based cohort study, using the data of the Prevention of Renal and Vascular Endstage Disease (PREVEND) Study, provides importante information on decline in kidney function at the population level. This study evaluated 6894 people over a 4-year period and reported loss in eGFR of 2.3 mL/min/1.73 m2/ 4 years in the whole population; 7.2 mL/min/1.73 m2/4 years in participants with macroalbuminuria and 0.2 mL/min/1.73 m2/4 year in participants with impaired renal function. The rate of eGFR decline was approximately two times higher in participants with proteinuria. Among adults aged 65 and older, progression varied by sex and presence of diabetes. In general studies suggest progression rates of approximately 0.3 to 1 mL/min/1.73 m2/year among participants without proteinuria or comorbidity and rates of approximately two to three times higher among participants with proteinuria or comorbidities11.
The contribution of GFR trajectory to the predictive model is consistent with a recent investigation that examined 22 cohorts to determine the association of past slopes and current eGFR level with subsequent end stage renal disease (ESRD). This investigation reported that both current eGFR level but more importantly the eGFR trajectories were predictors of progression to ESRD in patients with CKD12. Past slopes of eGFR provide an empirical measure of the disease process, which represents the aggregate effect of all known and unknown predictors of kidney disease progression for each patient. Nevertheless, in clinical practice, prediction of ESRD is most important for the immediately foreseeable future, because clinicians need to implement preparations, such as vascular access planning and referral for transplantation, during the 6–12 months preceding ESRD. These results suggest that interventions that slow kidney disease progression and preparations for ESRD should be continuously implemented in patients with CKD stages 4 and 5, even in the absence of demonstrable eGFR decline in the past 1–3 years12.
The finding that a more rapid past eGFR rise is associated with higher ESRD risk is reminiscent of associations between positive slopes and higher mortality in previous studies13,14. The explanation for these seemingly intuitive associations is unclear but could be explained by loss of muscle mass, volume overload, presence of severe illness with an underlying heightened propensity for faster kidney disease progression, or recovery from previous acute Kidney injury events12.
Thus, the last eGFR seems to be a robust predictor of future ESRD, but past trajectory of eGFR over time is also independently associated with ESRD and adds important information, especially in patients with lower eGFR in whom risk of progression to ESRD in the near future is greatest12.
The other variable associated with the initiation of dialysis was phosphate levels. Hyperphosphatemia plays an important role in mineral bone diseases and vascular calcifications, and is associated with increased risk of progression to ESRD, cardiovascular events, and all-cause mortality in CKD patients15. Hyperphosphatemia is not itself immediately harmful and may have numerous underlying causes, and serum phosphate level is not regularly used as an indicator for starting dialysis in clinical practice16. However, our study demonstrated that high serum phosphate level is a strong predictor of dialysis initiation for advanced CKD patients, contributing with a 6.25% greater probability of starting dialysis. Based on these findings, we suggest that clinicians should consider the use of serum phosphate as a laboratory marker in the decision-making process to initiate dialysis in advanced CKD patients.
When analyzing the other outcomes of this study, we found that 6% of this total population died before starting dialysis. The factors predicting death before HD start were congestive heart failure and cancer, which are intuitive variables, when patients who die the most are expected to be patients with more comorbidities. The presence of CKD is associated with poor prognosis in heart failure17. According to one study, the risk of death in heart failure may be more strongly associated with a decline in the GFR than with a decline in the left ventricular ejection fraction18.
In the CHARM trial, patients with chronic heart failure with CKD compared to patients without CKD had increased risk of cardiovascular death or heart failure hospitalization17. In cancer, there was a large cohort that showed a significant graded relationship between the severity of CKD and cancer mortality19 which reflects the negative impact of this comorbidity, even before starting HD.
Finally, 20% of the patients were dialysis-free during the 1-year of follow-up and higher hemoglobin levels (>10g/dL) without erythropoietin stimulating agents (ESA) levels associated with survival without needing dialysis.
Many reasons can be pointed out: higher values of hemoglobin presuppose a less severe stage of CKD, thus a slower progression to end stage renal disease; patients will have better general state, quality of life and thus less hospital admissions; higher levels of hemoglobin lead to lower renal ischemia, and therefore, less oxidative stress in the renal parenchyma, preserving it and delaying the onset of dialysis; anemia also has a negative impact on the immune system, increasing susceptibility to infectious complications and thus increasing the likelihood of worsening renal function and progressing to dialysis; Anemic patients are more malnourished and consequently more inflamed.
Thus, greater hemoglobin levels can be associated with better patient outcomes and higher probability of survival, without the needing HD.
Summarizing, it is clear that the timing of VA creation before dialysis start is important to optimize patient outcomes and health care resources. However, this is dependent on the challenging task of nephrologists and a multidisciplinary team to predict when a patient will need to start dialysis. The VA creation cannot be decided only by the eGFR. It needs to take into account the patient as a whole. The presence of some comorbidities such as age and diabetes mellitus are extremely important and can be associated with a higher likelihood of starting HD after VA construction.
Second is the severity of kidney dysfunction (measured not only by the eGFR but also by the degree of proteinuria) and perhaps more importantly, the trajectory of kidney function decline. At last, underlying patient and provider process factors can further alter the trajectory to dialysis start. This clinical uncertainty and the paucity of data in the literature may be reflected in the heterogeneity of clinical practice guidelines and the simplicity of using the severity of kidney function to guide the timing of AVF placement.
More research and data informing the relationships between vascular access placement, kidney function decline, and dialysis start may provide clarity for future guidelines and help lift the shroud of clinical unpredictability currently present.
References
1. Polkinghorne KR. E. Lok C. Can we predict the unpredictable after vascular access creation? Clin J Am Nephrol 2016; 11:1729–1731 [ Links ]
2. Polkinghome KR. Lopez-Vargas P. Preparation and placement of vascular access. Kidney Helth Australia. Cari Guidelines 2012;1–10 [ Links ]
3. Al-Balas A. Lee T. Young CJ. Barker-Finkel J. Allon M. Predictors of initiation for predialysis arteriovenous fistula. Clin J Am Soc Nephrol 2016; 11(10):1802-1808 [ Links ]
4. Tordoir J. Canaud B. Haage P. et al. EBPG on vascular access. Nephrology Dialysis Transplantation 2007. 22:ii88–ii117 [ Links ]
5. M. Kumwenda. S. Mitra and C. Reid. Clinical practice guidelines vascular access for haemodialysis. 2011. UK Renal Association [ Links ]
6. Canadian Society of N. Report of the canadian society of nephrology vascular access working group. Semin Dial 2012;25(1):22–25 [ Links ]
7. Ohira S. Naito H. Amano I. et al. 2005 Japanese Society for Dialysis Therapy guidelines for vascular access construction and repair for chronic hemodialysis. Ther Apher Dial 2006; 10(5):449–462 [ Links ]
8. Tordoir J. Canaud B. Haage P. et al. EBPG on vascular access. Nephrol Dial Transplant 2007; 22(2):ii88–ii117 [ Links ]
9. Smart NA. Titus TT. Outcomes of early versus late nephrology referral in chronic kidney disease: a systematic review. Am J Med 2011; 124(11):1073–1080 [ Links ]
10. Ruggenenti P. et al. Chronic proteinuric nephropathies: outcomes and response to treatment in a prospective cohort of 352 patients with different patterns of renal injury. Am J Kidney Dis 2000; 35(6):1155–1165 [ Links ]
11. Halbesma N. Kuiken DS. Brantsma AH. et al. Macroalbuminuria is a better risk marker than low estimated GFR to identify individuals at risk for accelerated GFR loss in population screening. J Am Soc Nephrol 2006; 17(9):2582–2590 [ Links ]
12. Kovesdy CP. Coresh J. Ballew SH. et al. Past decline versus current eGFR and subsequent ESRD risk. J Am Soc Nephrol 2016; 27(8):2447–2455 [ Links ]
13. Al-Aly Z. Zeringue A. Fu J. et al. Rate of kidney function decline associates with mortality. J Am Soc Nephrol 2010; 21(11):1961–1969 [ Links ]
14. Matsushita K. Selvin E. Bash LD. Franceschini N. Astor BC. Coresh J. Change in estimated GFR associates with coronary heart disease and mortality. J Am Soc Nephrol 2009; 20(12):2617–2624 [ Links ]
15. Palmer SC. Hayen A. Macaskill P. et al. Serum levels of phosphorus. parathyroid hormone. and calcium and risks of death and cardiovascular disease in individuals with chronic kidney disease: a systematic review and meta-analysis. JAMA 2011; 305(11):1119–1127 [ Links ]
16. Lua Y. Leea S. Lind H. et al. Serum phosphate as an additional marker for initiating hemodialysis in patients with advanced chronic kidney disease. Biomedical Journal 2015; 38(6):531–537 [ Links ]
17. Ahmed. A. Campbell RC. Epidemiology of chronic kidney disease in heart failure. Heart Fail Clin 2008; 4(4):387–399 [ Links ] Hillege HL. Girbes AR. de Kam PJ. et al. Renal function. neurohormonal activation and survival in patients with chronic heart failure. Circulation 2000; 102(2):203–210 [ Links ]
19. Weng P. Hung K. Huang H. Chen J. Sung P. Huang K. Cancer-specific mortality in chronic kidney disease: longitudinal follow-up of a large cohort. Clin J Am Soc Nephrol 2011; 6(5):1121–1128 [ Links ]
Rachele Escoli. MD
Centro Hospitalar do Médio Tejo. Avenida Xanana Gusmão. Ap 45.
2350-754. Torres Novas.
Telephone: +351 249 810 100
E-mail: rachele_escoli@hotmail.com
Disclosure of potential conflicts of interest: none declared
Received for publication: Jul 25, 2017
Accepted in revised form: Sep 06, 2017


{kind=link}
{kind=link}