










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.31 no.2 Lisboa jun. 2017
REVIEW ARTICLE
Diabetic Nephropathy and its two phenotypes: the proteinuric and non-proteinuric
Regina Silva, Catarina Meng, Luís Coentrão
Nephrology and Infectious Diseases Research and Development Group, INEB-(I3S), University of Porto, Porto – Portugal.
ABSTRACT
The typical progression of diabetic nephropathy is from the normoalbuminuric stage to microalbuminuria (urinary albumin creatinine rate, UACR, 30-300 mg/g) to end in overt proteinuria. A growing body of recent evidence has shown an accelerated decrease in glomerular filtration rate predominately seen in normoalbuminuric patients with type 2 diabetes. This discovery raises the the possibility of there being two independent diabetic nephropathy phenotypes.
The aim of this review is to collect, summarize and compare the most relevant data referring to both the classical/proteinuric (UACR>300mg/g) and the non-classical/ non-proteinuric (UACR < 300 mg/g) phenotypes in type 2 diabetic patients.
PubMed research into diabetic nephropathy and both proteinuric and non-proteinuric phenotypes was undertaken. A total of 67 articles were included.
Several studies have shown that diabetic nephropathy may co-exist within a normal range of albumin excretion.
This new emerging phenotype is nowadays extremely frequent in type 2 diabetic patients, and seems to be found more often in female sex, older adults, and patients with metabolic syndrome. Albumin does not seem to be the best marker for this phenotype. New possible markers for early stage renal disease were found. Treatment with Renin-Angiotensin-System inhibitors, according to evidence, might not be the most adequate therapy for non-proteinuric diabetic patients. Prognosis is still unclear.
This new diabetic nephropathy phenotype exists and clinicians should be aware of it, to ensure these patients are not underdiagnosed. More research is needed to clarify this phenotypes epidemiology, pathogenesis, risk factors, diagnosis methods, new biomarkers, best treatment approach and its prognosis.
Key words: Albuminuria; Diabetes mellitus, type 2; Diabetic nephropathies; Glomerular Filtration Rate; Renal Insufficiency, chronic.
INTRODUCTION
The prevalence of type 2 diabetes mellitus (T2DM) is steadily increasing, mostly due to a combination of obesity, urbanization, and ageing population.1,2 In parallel, the prevalence of its macrovascular and microvascular complications, such as diabetic nephropathy (DN), which occurs in 20 to 40% of type 2 diabetic patients, has risen.3,4 Despite efforts made to slow the progression of DN, this is still the most common cause of end-stage renal disease (ESRD) in developed countries.3,5-7
Diabetic renal disease is a clinical syndrome characterized by overt proteinuria (urinary albumin creatinine ratio, UACR> 300 mg/g) and declining renal function.8 In the past, it was believed that DN only had one path of progression – from a normoalbuminuric stage, to microalbuminuria (UACR 30-300 mg/g), to end in overt proteinuria (UACR> 300 mg/g). However, in the last few years a growing body of evidence has shown an accelerated decrease in glomerular filtration rate (GFR) predominately seen in type 2 diabetic chronic kidney disease (CKD) patients with UACR< 300mg/g. This discovery has raised the possibility of their being two independent diabetic nephropathy phenotypes.8,9
The aim of this review is to collect, summarize and compare the most relevant data regarding both the classical/ proteinuric and the non-classical/ non-proteinuric phenotypes in T2DM patients.
PATIENTS AND METHODS
We searched PubMed using the query Non-proteinuric OR nonalbuminuric AND diabetic nephropathy.
Type 1 diabetes mellitus patients were excluded from the study. Classical/proteinuric DN was defined as UACR>300 mg/g and the non-classical/non-proteinuric DN as UACR< 300 mg/g. Articles written up to August 2016, in English or in Portuguese, were included. From the initial research, a manual selection based on the article abstract was made. Articles that were duplicated, had inaccessible full text or were unsuited to this review were excluded.
CLASSICAL PHENOTYPE
The classical phenotype of DN is described as a linear progression from normoalbuminuria to microalbuminuria to macroalbuminuria, eventually ending in ESRD.9
DN progression has been classified into 5 stages. The first stage (pre-nephropathy) is described as normoalbuminuria (UACR<30 mg/g) and glomerular filtration rate (GFR)≥ 30mL/min/1.73 m2 associated with glomerular hyperfiltration and hypertrophy. The second stage (incipient nephropathy) includes microalbuminuria levels (UACR 30-300 mg/g) and GFR≥ 30mL/min/1.73 m2, with renal structure changes, such as thickening of glomerular capillary basement membrane. One third of the patients progresses to the third stage (overt nephropathy), characterized by macroalbuminuria (UACR≥ 300 mg/g Cr) or persistent proteinuria (≥ 0.5g/day), and GFR≥ 30mL/min/1.73 m2. The fourth stage (kidney failure) includes any albuminuria or proteinuria levels and GFR≤ 30mL/min/1.73 m2. The last stage (dialysis therapy/ ESRD) is when uraemia occurs or dialysis therapy is implemented due to DN.1,9-12 In the majority of studies, albuminuria levels were the proven best clinical predictor of kidney function loss, reason why its urinary excretion levels is nowadays the screening test for DN.1,3,6,13,14 It has also been shown that microalbuminuria is a powerful independent risk factor for cardiovascular disease.3,5,15,16 In addition, Mogensen demonstrated that microalbuminuria is a good clinical predictor of overt proteinuria and increased mortality in T2DM patients.17
Risk factors
Many studies have shown that the progression of type 2 diabetic renal disease is associated with some risk factors, such as ethnicity, with American-Hispanics, Asians and African American at greater risk of progression to ESRD than Caucasians.18,19 Other risk factors include family history of diabetic kidney disease, genetic predisposition, male gender, smoking history, severe albuminuria, lower baseline estimated GFR, older age, diabetes duration, obesity, higher systolic blood pressure, poor glycaemic control, bad lipid level control, previous retinopathy and elevated white cell blood count.20-22 Recent evidence has shown gender differences with females at greater risk of renal function decline than males, who are more vulnerable to albuminuria excretion rate progression. The risk of renal function decline in women is associated with systolic blood pressure, age, plasma glucose levels, and increased cholesterol / HDL ratio, whereas triglycerides are associated with better prognosis. In males, urinary albumin excretion rate together with plasma glucose and systolic blood pressure are associated with greater renal decline, whereas waist circumference and cholesterol/HDL ratio are associated with better renal function prognosis.21
According to recent data, the origin of albuminuria has two possible mechanisms. In the traditional model, increases in glomerular permeability lead to increasing amounts of albumin filtered per day, which may be endocytosed by megalin/cubilin receptor, and directed to lysosome, in order to be degraded and returned to blood supply. When filtered albumin level rises above a certain value, this endocytic pathway becomes saturated, leading to a rise in urinary albumin excretion.
The second, and more recent theory, proposes a tworeceptor model. One high capacity low affinity receptor involved in the retrieval pathway (filtered albumin through transcytosis in the proximal tubular cell ends in the blood supply), and other receptor (which has high affinity and low capacity) involved in the degradation pathway (lysosomally process unretrieved filtered albumin). Nephrotic levels of proteinuria occur when retrieval pathway is overloaded.23,24
Histopathological findings
Few studies include kidney biopsies of DN in T2DM patients, but those that do histologically show a heterogeneity of histological lesions characterized by glomerular and tubular basement membrane thickening, mesangial sclerosis that can be diffuse, nodular (Kimmelstiel-Wilson lesion), or both, as well as exudative lesions (intramembranous, sub-capsular, and arteriolar hyalinosis). Kidney biopsies diagnosed as DN can be classified into four classes. Class I includes mild, nonspecific light-microscope changes and basement membrane thickening, which is the earliest structural abnormality in DN; Class II, mesangial expansion, mild (IIa) or severe (IIb) but without nodular sclerosis; Class III has nodular sclerosis at least in one glomerular; Class IV is when more than 50% of global glomerulosclerosis exists with other clinical or pathological evidence that sclerosis is attributable to DN.12,19,25
In a study conducted by Fioretto et al, where DN in T2DM patients histological lesions were classified into 3 classes, 29.4% were classified as Class I (normal or near normal histological renal structure); 29.4% as Class II (typical changes in histopathological DN) and 41.2% as Class III (atypical patterns of injury with absent or only mild diabetic glomerular changes associated with disproportionally severe renal structures changes including important tubule-interstitial with or without arteriolar hialynosis or glomerular sclerosis). HbA1c levels were higher in Classes II and III, which suggests that hyperglycaemia may cause different patterns of renal injury.26
New paradigms on the classical phenotype natural history
Recently, the classical phenotype of DN has been questioned. Microalbuminuria does not invariably progress to proteinuria. In fact, in some patients regression or remission to normoalbuminuria has occurred. In the Araki et al. study, regression of microalbuminuria occurred in 50% of T2DM patients, whereas progression to overt proteinuria occurred in 28% of the patients.5
In another study conducted by Gaede et al with a follow-up of 7.8 years, 46 out of 151 T2DM patients achieved remission to normoalbuminuria; 58 remained microalbuminuric and 47 progressed to overt nephropathy.
Remission to normoalbuminuria was associated with a decreased GFR decline during the follow up period (2.3± 0.4 mL/min/year vs. 3.7± 0.4 mL/min/year in microalbuminuric patients vs. 5.4± 0.5 mL/min/year in patients who progressed to overt proteinuria). This regression was more prone to happen when blood pressure (ideally under 130/80 mmHg) and glycaemic blood levels (ideally HbA1c ≤ 6, 5%) were under control. The use of albumin-renin-aldosterone inhibitors (inhibitors of angiotensin-converting enzyme or angiotensin II receptor antagonist) have also shown significant help in reversion to normoalbuminuria, which explains why this medication should be used when controlling blood pressure in diabetic patients.27 Finally, recent data has shown that the decrease in renal function in diabetic patients can occur when patients have normoalbuminuric levels, suggesting the existence of an alternative pathway.7,18
Non-proteinuric phenotype
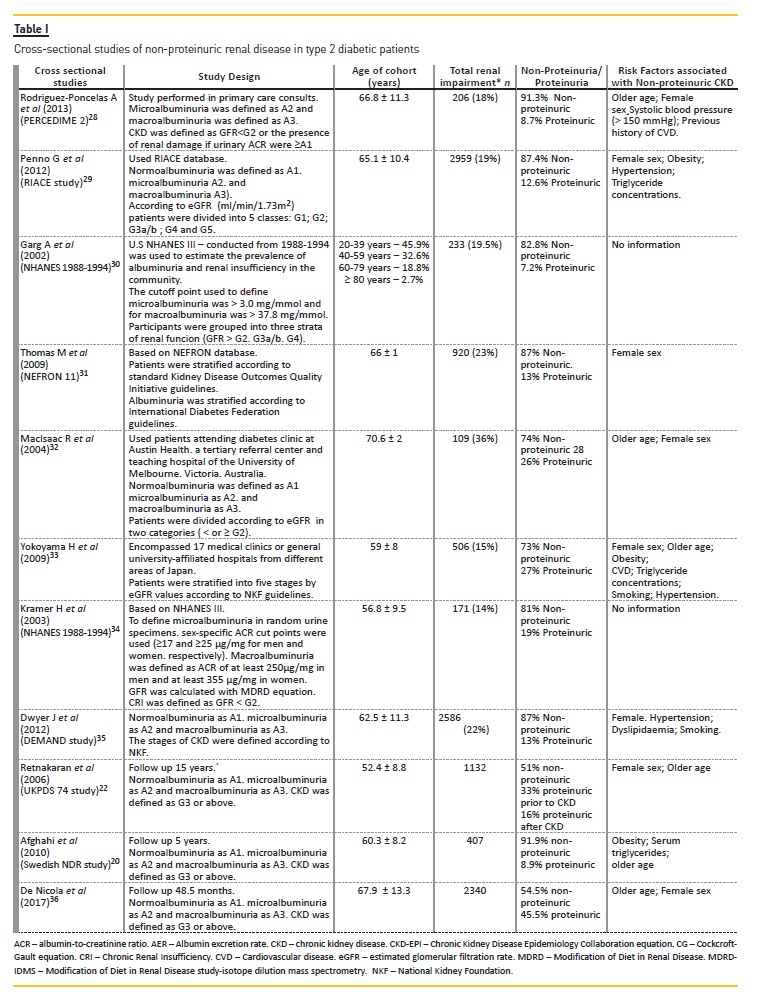
Many studies of the last decade have shown the possibility of a decline in GFR without the presence of proteinuria (UACR > 300 mg/g) in T2DM patients, the so-called non-Classical or non-Proteinuric phenotype (Table I).
In PERCEDIME2, a national cross-sectional study, renal impairment was found in 206 subjects with T2DM; of these 188 (91.3 %) were non-proteinuric.28 Another study analysed patients from the RIACE multicentre study and concluded that within patients with renal impairment, 87.4% were non-proteinuric and 12.6% were proteinuric.29 Results based on the cross-sectional NHANES III study show that 82.8% of diabetic patients with GFR <60mL/min/1.73 m2 demonstrated no proteinuria.30 In NEFRON 11, 87% of the patients with low eGFR had an UACR that was persistently in the non-proteinuric range.31 In another cross-sectional study, of 109 patients with renal impairment, 81 (74%) were non-proteinuric and 28 (26%) were proteinuric.32 In a Japanese crosssectional study, 73% of T2DM non-proteinuric patients had low GFR.33 A cross-sectional study based on NHANES III patients showed that of 171 patients with CKD, 81% were non-proteinuric and 19% proteinuric.34 Other studies showed similar results, such as the DEMAND study where CKD was found in 87% of non-proteinuric and 13% of proteinuric diabetic patients.35
Longitudinal studies, such as the UKPDS study, showed that within a 15-year follow-up of 1132 T2DM patients who developed renal impairment, 575 (51%) were always non-proteinuric throughout the study; 33% developed it after having proteinuric levels and 185 (16%) developed it prior to proteinuric levels.22 The Swedish National Diabetes Register (NDR) study showed that among patients who developed renal impairment, 91.9% were non-proteinuric.20 Similar results have also been reported in a more recent prospective cohort by the De Nicola et al study, consisting of 2340 patients with stage III-V of CKD; 54.5% of T2DM patients were non-proteinuric.36
Pathogenesis and risk factors
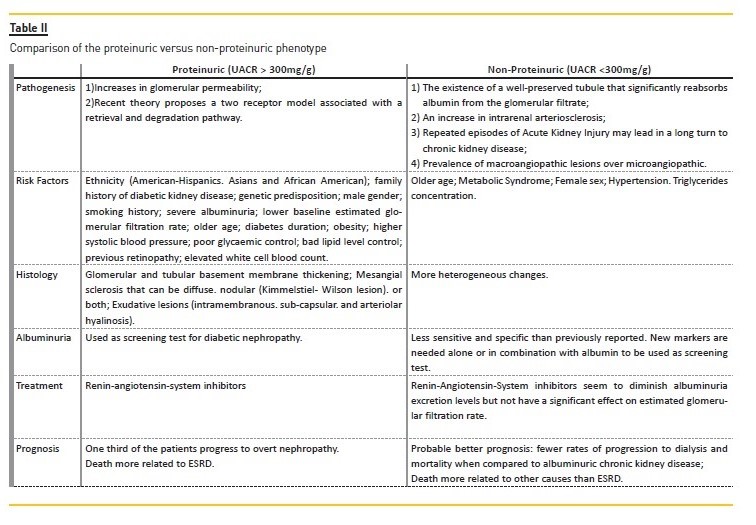
Several pathogenic mechanisms have been proposed to explain the non-proteinuric phenotype of T2DM nephropathy (Table II):
1. The existence of a well-preserved tubule that leads to a significant reabsorption of albumin from the glomerular filtrate, thus resulting in a diminished albumin excretion into normoalbuminuric levels.1 In a review of histological aspects of diabetic nephropathy it was stated that type 2 normoalbuminuric diabetic patients with chronic kidney disease (CKD) had more advanced glomerular, tubulointerstitial and vascular lesions than normoalbuminuric with preserved renal function. Typical glomerular changes were less commonly seen in normoalbuminuric patients than albuminuric, suggesting more heterogeneous changes in normoalbuminuric than albuminuric CKD.2
2. An increase in intrarenal arteriosclerosis as opposed to classical glomerulosclerosis changes present in albuminuric subjects. MacIsacc et al. studied the role of intrarenal vascular disease in the pathogenesis of non-albuminuric renal insufficiency of T2DM patients. His conclusions were against this theory as diabetic patients with renal impairment had similar degrees of intrarenal vascular disease, measured by intrarenal arterial resistance index, regardless of their albumin excretion rate (AER) status.37
3. Diabetic patients are susceptible to repeated episodes of Acute Kidney Injury (AKI). These repeated episodes of AKI may lead in the long-term to CKD, as regenerator potential of tubular progenitors is limited.(38, 39)
4. One of the most compelling pieces of evidence is the prevalence of macroangiopathic lesions over microangiopathic. This is supported by several studies showing a weaker relationship between renal impairment and normal albumin excretion levels with other microvascular complications such as diabetic retinopathy.40 In the Penno et al study the albuminuric CKD phenotypes with (OR 2.967 95% CI 2.473-3.559) and without (OR 2.142 95% CI 1.858-2.468) reduced GFR, were more strongly associated with advanced retinopathy than was the nonalbuminuric phenotype (OR 1.290 95%CI 1.059-1.570).40 Penno et al also showed that neither intraindiviual HbA1c nor HbA1c variability were independently associated with low eGFR and normoalbuminuric stage 3 to 5, suggesting that this phenotype was not related to glycaemic control.41 In addition, the same author reported a higher prevalence of cardiovascular disease (CVD) in normoalbuminuric patients with renal impairment.29 Other studies support the theory that macroangiopathy rather than microangiopathy is the prevailing pathway underlying non-proteinuric CKD.42
This new phenotype was found to be more pronounced in the 60-79 years-old age group where 34% of diabetic subjects with GFR below 30 mL/min per 1.73 m2 demonstrated no albuminuria levels.30 This association with older age raises the question if the decline in GFR isn´t actually the physiological nephron loss that happens with the aging process due to agerelated vascular changes. In Delanaye et als opinion paper, the authors defended the need of an age-calibrated definition of CKD in order to distinguish agerelated from disease related changes in eGFR. Supporting that in patients younger than 40 years, CKD should be defined as below 75 mL/min/1.73m², ages between 40 and 65 years, defined by 60 mL/min/1.73m², and when older than 65 years, without albuminuria or proteinuria, CKD should be defined by eGFR below 45 mL/min/1.73m².This would avoid overestimating CKD (medicalization of senescence) in the elderly and underestimation CKD from potential treatable causes in younger patients.43
The female sex seems to be the most related to this non-classical pathway.28,29,31-33,35,44 Metabolic syndrome was also a risk factor only in men younger than 60 years old and postmenopausal women.45,46 Mottl et al showed that non-Hispanic whites had a higher preponderance of non-albuminuric CKD whereas non-Hispanic blacks had greater preponderance of albuminuric CKD.47
Histopathological findings
To date few studies have compared histological findings in patients with CKD and normoalbuminuria versus CKD with albuminuria (micro- or macroalbuminuria).
The Ekinci et al.study classified kidney biopsies of normo-micro-and macroalbuminuric patients according to the Fioretto classification. Considering the normoalbuminuric group of patients, 3 out of 8 were classified as class II (two with mild diffuse mesangial expansion and/or glomerular basement membrane thickening and one with advanced nodular diabetic glomerular sclerosis); another 3 out of 8 patients were classified as Class III (with predominantly interstitial or vascular changes) and the remaining two Class I (nonspecific changes). Microalbuminuric and macroalbuminuric patient biopsies were mainly classified as Class II. Therefore, typical renal structure changes of DN were observed in T2DM patients with elevated levels of albuminuria, whereas in normoalbuminuric renal insufficiency these changes were less frequently seen.48 In another study by Budhiraja et al, kidney biopsies of non-proteinuric T2DM patients, with GFR < 60 mL/min/1.73m² were analysed. On light microscopy, all the 10 non-proteinuric diabetic patients had capillary wall thickening; 2 out of 10 patients had severe diffuse mesangial thickening but no nodules, while 8 patients had Kimmelstiel-Wilson nodules on the biopsy. The tubules and tubule interstitium was relatively well preserved and afferent and efferent arteriolar hyalinosis was also observed.49
Is albumin the best marker?
The existence of this new prevalent non-proteinuric phenotype in DN raises the question if albumin is indeed the best clinical predictor marker and screening test for CKD in diabetic patients. Actual guidelines state that the diagnosis of DN should be made by 2 out of 3 abnormal UACR measures in a morning urine specimen or abnormal albumin level in 24-hour urine.50 In order to be a good clinical test, microalbuminuria should meet two criteria: 1) a measurable rise should occur early enough to allow clinical intervention, and 2) its rise in level should correlate with outcomes. Unfortunately, neither of these conditions is fulfilled by microalbuminuria, as CKD can occur at normoalbuminuric levels and as microalbuminuria can regress to normoalbuminuria.51 Several studies suggest that microalbuminuria is less sensitive and specific than previously reported. In a Japanese study, urinary albumin was found to be an unreliable indicator for renal structure status in Japanese T2DM patients.52 However, in a review concerning this topic, albumin excretion rate was stated to be the best currently available non-invasive means of following the course of kidney disease in nonproteinuric diabetic patients, concurring that it does not predict DN with the accuracy suggested by other studies, as it can be estimated that 40% of dipstick-negative T2DM patients who are ultimately destined to develop proteinuria will be normoalbuminuric at initial screening, whereas 60% will be microalbuminuric.53
Many studies have been conducted with the aim of finding new markers to replace or at least combine with albuminuria. Some investigated the concentration of inflammatory markers of TNF pathway (free TNFα, Total TNFα, TNFR1, TNFR2) and concluded that the risk for ESRD in T2DM was strongly associated with higher concentrations of circulating TNFR1 and TNFR2. This association was stronger in patients without proteinuria than those with proteinuria; thus these two markers are possibly new predictors of ESRD, more revealing than proteinuria.54 A further study showed that urinary liver-type fatty acid-binding protein (L-FABP), a protein expressed in the proximal tubule of the human kidney, accurately reflected the severity of DN and was significantly higher in patients with T2DM who had normoalbuminuria than control subjects. Even though L-FABP significantly correlated with the albumin levels in all patients, it did not correlate with urinary albumin levels in the subgroup with GFR above 60 mL/min per 1.73 m2. So association of albumin and L-FABP could be a good marker, not only for early diagnosis but also for risk stratification.55
Another study into glomerular (IgG) and tubular markers (Proximal – KIM-1; NGAL; NAG; Cystacin C; Distal – H-FABP) in diabetic patients showed that differences between albuminuria categories were more pronounced for glomerular (> 30-fold increase from normoalbuminuria to macroalbuminuria) and distal tubular markers (> 21-fold increase). Differences were less pronounced for proximal tubular markers. After the adjustment for albumin, H-FABP was the only marker associated to eGFR, which makes it a promising marker in combination with albumin to predict the clinical outcome of DN.56
Recently Kopf et al. aimed to compare the urinary excretion of albumin and adiponectin as predictors for decline of renal function in patients with T2DM and early kidney disease. After 1 year of follow up they concluded that urinary high molecular weight adiponectin (HMW-adiponectin) excretion might identify diabetic patients at increased risk of progression of kidney disease.57 In recent research into the role of microRNA as possible markers, Chien et al. concluded that DN progressors, which are patients with a more rapid change of eGFR or albumin creatinine ratio (ACR), exhibited significantly greater serological levels of miR-21 and miR-29 family, but not miR-192, in comparison to non-progressors, revealing that miRNAs may serve as early indicators of diabetes mellitus-mediated renal pathology. miR-21 is possibly the most sensitive circulating miRNA to reflect early renal dysfunction.58
In the Narita et al. study, elevated levels of transferrin (a marker of glomerular damage) in non-proteinuric patients was a predictor for proteinuric development.59
The Araki et al. study concluded that high urinary excretion of type IV collagen was associated with deterioration of renal function in T2DM patients without overt proteinuria.60 In the Zurbig et al. cohort study, CKD273 (an urinary proteomics-based classifier), when applied to non-proteinuric patients, was found to identify those patients who would develop diabetic nephropathy during the follow-up period, with a better performance than UACR. Their results showed that this classifier identified progressors in 65% of the case subjects 5 years earlier than when UACR was used.61
Taking all this into consideration, there is still the need for more studies on these new possible markers in order to validate them and include them in guidelines for DN diagnose and monitoring. Until then, clinicians should use for T2DM patients annual measurements of urinary albumin excretion levels in 24 hours-urine or UACR measured in a morning urine specimen plus measurement of GFR by modification of diet in renal disease (MDRD) equation or Chronic Kidney Disease-Epidemiology Collaboration equation (CKD-EPI), blood pressure measurements and funduscopic evaluation so that normoalbuminuric patients with renal impairment can be detected and have a better follow-up.62
Treatment
Another question about this new phenotype: is the treatment used for the classical phenotype the best for the non-classical? Despite efforts, this question is still unanswered, as little evidence exists in this matter.
Interestingly, recent data have questioned the role of renin-angiotensin-system (RAS) inhibitors in the progression of CKD in T2DM patients. MacIsaac et al. found no significant difference in the use of any anti-hypertensive agent, specifically RAS inhibitors, for proteinuric or non-proteinuric patients with GFR below 60 mL/min per 1.73 m2.32 Also, in the DEMAND study, patients with non-proteinuria or proteinuria, with or without treatment with angiotensin-converting-enzyme (ACE) inhibitors (tandalopril or delopril), had similar decreases in measured eGFR.35 This enhances the need for more studies on the subject to better clarify this question and to find new alternatives in order to optimize nonproteinuric patients therapy. Until then clinicians should follow recent 2014 guidelines from American Diabetes Association that recommend the use of RAS blockers (either ACE inhibitors or angiotensin II receptor blocker (ARBs), but not in combination) for non-pregnant patients with modestly raised albumin levels (30-299 mg/day) or above 300 mg/day.63
Prognosis
This seems to be a controversial topic as there are contradictory results. Some studies which attempted to document the natural history of normoalbuminuric CKD suggested a better prognosis, with fewer rates of progression to dialysis and mortality when compared to albuminuric CKD.42 Riggaleau et al. during a followup of 38 months concluded that changes in UACR, serum creatinine and MDRD eGFR did not differ significantly according to baseline albumin level. However, in the normoalbuminuric group, albuminuria and serum creatinine levels persisted during all the follow up period. In contrast, both micro- and macroalbuminuric groups had progressive CKD during follow-up. These results suggest a better outcome in the normoalbuminuric group.64 On the other hand, MacIsacc et al reported that the rate of decline in GFR was not significantly different between non-proteinuric and proteinuric patients.32 Interestingly, in a prospective study conducted by De Nicola et al, over a median follow-up of 48 months, an inverse relative risk of ESRD and death from other causes was observed in the non-proteinuric group, with this group of T2DM patients with higher mortality because of other causes than ESRD (p=0.002) versus the proteinuric group where death was in the majority of cases due to ESRD, rather than other causes (p < 0.0001).36 Also, in the Dreyer et al 5-year retrospective study, a cohort of 3855 diabetic patients, the annual adjusted decline in GFR for those with proteinuria at baseline was 2.05, with both South-Asian and black groups having a significantly rate decline than white groups.65 In a cohort study using a gold-standard method (plasma clearance of iohexol), Ruggenetti et al found no differences in GFR decline between proteinuric and non-proteinuric patients, although the median GFR decrease was still much faster than in the general population.66 Therefore, more longitudinal studies are still needed to try to figure out the natural evolution in non-proteinuric T2DM patients.
Doubts about the real existence of the non-proteinuric phenotype
Despite all the data published in the literature regarding the possible existence of a non-proteinuric phenotype, some authors have raised issues about it.
First, that the MDRD equation underestimates the glomerular filtration rate, creating an artificial non-proteinuric group. However, when the GFR by MDRD equation was compared with the isotopic GFR (i-GFR) the mean MDRD GFR (41.3 ± 13.1 mL/min per 1.73 m2) did not differ significantly from i-GFR (45.6 ± 29.7 mL/min per 1.73 m2). In the non-albuminuric patients, i-GFR did not differ from MDRD GFR, showing that most normoalbuminuric diabetic subjects with CKD according to an MDRD GFR below 60 mL/min per 1.73 m2 do really have that GFR.64 Second, according to what has been previously reported, remission/ regression from microalbuminuria to normoalbuminuric levels is a consequence of treatment (especially due to renin-angiotensin-blockers), rather than a true remission. Therefore, diabetic patients with non-proteinuria may actually be proteinuric patients who have been controlled with anti-hypertensive agents.9,27 In some studies, no significant differences were found in the use of any anti-hypertensive agent, specifically RAS inhibitors for patients with GFR below 60 mL/min per 1.73 m2 and patients with non-proteinuria or proteinuria.32
Another possibility is that the so called non-proteinuric phenotype is actually caused by non-diabetic renal disease (NDRD), that causes GFR decline. The Soleymanian et al study, evaluated 46 T2DM patients. 34.8% had DN and 43.5% NDRD and 21.7% NDRD superimposed with DN. In the NDRD, membranous nephropathy (34%) was the most common. Also, NDRD was more related to a lower frequency of diabetic retinopathy, shorter duration of diabetes, higher range of proteinuria and better kidney survival.67 However more studies, with a larger number of biopsies, are needed to validate these results.
CONCLUSION
Cumulative evidence has shown that microalbuminuria regression/remission is possible and that renal insufficiency may co-exist within a normal range of protein excretion. This new emerging phenotype is quite prevalent in T2DM patients, and found more often in the presence of female sex, older age and metabolic syndrome. The non-proteinuric phenotype probably is due to a distinct pathological pathway, more related to macroangiopathic lesions rather than microangiopathic. Albuminuria is believed to be the best marker of DN. However, tubular markers such as L-FABP, H-FABP or miR-21, CDK273 and transferrin seem promising markers for early stage renal disease.
Also, HMW-adiponectin may be useful in identifying diabetic patients at higher risk of progression of kidney disease. More studies are needed to confirm the possible use of these new markers either alone or in association with albuminuria. Treatment with RAS inhibitors, according to evidence, might not be the most adequate therapy for non-proteinuric T2DM patients. They do not seem to significantly affect GFR decline in this type of patients. Prognosis is still unclear, as contradictory evidence exists, but probably it has a better prognosis when compared to the classical phenotype.
In conclusion, the majority of the medical community is still unaware of this new phenotype, which can lead to the underdiagnosis of DN. Despite every effort to make this new phenotype more widely known, more studies are needed to clarify its epidemiology, pathogenesis, risk factors, diagnostic methods, new biomarkers, best treatment approach and its prognosis.
REFERENCES
1. Chawla V, Roshan B. Non-proteinuric diabetic nephropathy. Curr Diab Rep. 2014;1410:529. [ Links ]
2. Teng J, Dwyer KM, Hill P, et al. Spectrum of renal disease in diabetes. Nephrology. 2014;199:528-36. [ Links ]
3. Kowalski A, Krikorian A, Lerma EV. Diabetes and chronic kidney disease. Dis Mon. 2015;619:378-86. [ Links ]
4. Macisaac RJ, Ekinci EI, Jerums G. Markers of and risk factors for the development and progression of diabetic kidney disease. Am J Kidney Dis. 2014;632:S39-62. [ Links ]
5. Araki S, Haneda M, Sugimoto T, et al. Factors associated with frequent remission of microalbuminuria in patients with type 2 diabetes. Diabetes. 2005;5410:2983-7. [ Links ]
6. Said SM, Nasr SH. Silent diabetic nephropathy. Kidney International. 2016;901:24-6. [ Links ]
7. Yamada T, Komatsu M, Komiya I, et al. Development, progression, and regression of microalbuminuria in Japanese patients with type 2 diabetes under tight glycemic and blood pressure control: the Kashiwa study. Diabetes Care. 2005;2811:2733-8. [ Links ]
8. Porrini E, Ruggenenti P, Mogensen CE, et al. Non-proteinuric pathways in loss of renal function in patients with type 2 diabetes. Lancet Diabetes Endocrinolol. 2015;35:382-91. [ Links ]
9. Pugliese G. Updating the natural history of diabetic nephropathy. Acta Diabetol. 2014; 516:905-15. [ Links ]
10. Haneda M, Utsunomiya K, Koya D, et al. A new classification of Diabetic Nephropathy 2014: a report from Joint Committee on Diabetic Nephropathy. Clin Exp Nephrol. 2015;191:1-5. [ Links ]
11. Mogensen CE, Christensen CK, Vittinghus E. The stages in diabetic renal disease. With emphasis on the stage of incipient diabetic nephropathy. Diabetes. 1983;322:64-78. [ Links ]
12. Robles NR, Villa J, Gallego RH. Non-proteinuric diabetic nephropathy. J Clin Med. 2015;49:1761-73. [ Links ]
13. Fioretto P, Caramori ML, Mauer M. The kidney in diabetes: dynamic pathways of injury and repair. The Camillo Golgi Lecture 2007. Diabetologia. 2008;518:1347-55. [ Links ]
14. Mise K, Hoshino J, Ueno T, et al. Clinical and pathological predictors of estimated GFR decline in patients with type 2 diabetes and overt proteinuric diabetic nephropathy. Diabetes Metab Res Rev. 2015;316:572-81. [ Links ]
15. Bakris GL, Molitch M. Microalbuminuria as a risk predictor in diabetes: the continuing saga. Diabetes Care. 2014;373:867-75. [ Links ]
16. Ninomiya T, Perkovic V, de Galan BE, et al. Albuminuria and kidney function independently predict cardiovascular and renal outcomes in diabetes. J Am Nephrol. 2009;208:1813-21. [ Links ]
17. Mogensen CE. Microalbuminuria predicts clinical proteinuria and early mortality in maturity-onset diabetes. N England J Med. 1984;3106:356-60. [ Links ]
18. Parving HH, Lewis JB, Ravid M, Remuzzi G, Hunsicker LG, DEMAND investigators. Prevalence and risk factors for microalbuminuria in a referred cohort of type II diabetic patients: a global perspective. Kidney Int. 2006;6911:2057-63. [ Links ]
19. Tonolo G, Cherchi S. Tubulointerstitial disease in diabetic nephropathy. Int J Nephrol Renovasc Dis. 2014;7:107-15. [ Links ]
20. Afghahi H, Cederholm J, Eliasson B, et al. Risk factors for the development of albuminuria and renal impairment in type 2 diabetes--the Swedish National Diabetes Register (NDR). Nephrol Dial Transplant. 2011;264:1236-43. [ Links ]
21. Halbesma N, Brantsma AH, Bakker SJ, et al. Gender differences in predictors of the decline of renal function in the general population. Kidney Int. 2008;744:505-12. [ Links ]
22. Retnakaran R, Cull CA, Thorne KI, Adler AI, Holman RR, Group US. Risk factors for renal dysfunction in type 2 diabetes: U.K. Prospective Diabetes Study 74. Diabetes. 2006;556:1832-9. [ Links ]
23. Comper WD, Hilliard LM, Nikolic-Paterson DJ, Russo LM. Disease-dependent mechanisms of albuminuria. Am J Physiol Renal Physiol. 2008;2956:F1589-600. [ Links ]
24. Russo LM, Sandoval RM, McKee M, et al. The normal kidney filters nephrotic levels of albumin retrieved by proximal tubule cells: retrieval is disrupted in nephrotic states. Kidney Int. 2007;716:504-13. [ Links ]
25. Tervaert TW, Mooyaart AL, Amann K, et al. Pathologic classification of diabetic nephropathy. J Am Soc Nephrol. 2010;214:556-63. [ Links ]
26. Fioretto P, Mauer M, Brocco E, et al. Patterns of renal injury in NIDDM patients with microalbuminuria. Diabetologia. 1996;3912:1569-76. [ Links ]
27. Gaede P, Tarnow L, Vedel P, Parving HH, Pedersen O. Remission to normoalbuminuria during multifactorial treatment preserves kidney function in patients with type 2 diabetes and microalbuminuria. Nephrol Dial Transplant. 2004;1911:2784-8. [ Links ]
28. Rodriguez-Poncelas A, Garre-Olmo J, Franch-Nadal J, et al. Prevalence of chronic kidney disease in patients with type 2 diabetes in Spain: PERCEDIME2 study. BMC Nephrol.2013;14:46. [ Links ]
29. Penno G, Solini A, Bonora E, et al. Clinical significance of nonalbuminuric renal impairment in type 2 diabetes. J Hypertens. 2011;299:1802-9. [ Links ]
30. Garg AX, Kiberd BA, Clark WF, Haynes RB, Clase CM. Albuminuria and renal insufficiency prevalence guides population screening: results from the NHANES III. Kidney Int. 2002;616:2165-75. [ Links ]
31. Thomas MC, Macisaac RJ, Jerums G, et al. Nonalbuminuric renal impairment in type 2 diabetic patients and in the general population (national evaluation of the frequency of renal impairment cO-existing with NIDDM [NEFRON] 11). Diabetes Care. 2009;328:1497-502. [ Links ]
32. MacIsaac RJ, Tsalamandris C, Panagiotopoulos S, Smith TJ, McNeil KJ, Jerums G. Nonalbuminuric renal insufficiency in type 2 diabetes. Diabetes Care. 2004;271:195-200. [ Links ]
33. Yokoyama H, Sone H, Oishi M, et al. Prevalence of albuminuria and renal insufficiency and associated clinical factors in type 2 diabetes: the Japan Diabetes Clinical Data Management study (JDDM15). Nephrol Dial Transplant. 2009;244:1212-9. [ Links ]
34. Kramer HJ, Nguyen QD, Curhan G, Hsu CY. Renal insufficiency in the absence of albuminuria and retinopathy among adults with type 2 diabetes mellitus. JAMA. 2003;28924:3273-7. [ Links ]
35. Dwyer JP, Parving HH, Hunsicker LG, Ravid M, Remuzzi G, Lewis JB. Renal dysfunction in the presence of normoalbuminuria in type 2 diabetes: results from the DEMAND Study. Cardiorenal Med. 2012;21:1-10. [ Links ]
36. De Nicola L, Provenzano M, Chiodini P, et al. Epidemiology of low-proteinuric chronic kidney disease in renal clinics. PLoS One. 2017;122:e0172241. [ Links ]
37. MacIsaac RJ, Panagiotopoulos S, McNeil KJ, et al. Is nonalbuminuric renal insufficiency in type 2 diabetes related to an increase in intrarenal vascular disease? Diabetes Care. 2006;297:1560-6. [ Links ]
38. Kline J, Rachoin JS. Acute kidney injury and chronic kidney disease: its a two-way street. Ren Fail. 2013;354:452-5. [ Links ]
39. Romagnani P, Remuzzi G. Renal progenitors in non-diabetic and diabetic nephropathies. Trends Endocrinol Metab. 2013;241:13-20. [ Links ]
40. Penno G, Solini A, Zoppini G, et al. Rate and determinants of association between advanced retinopathy and chronic kidney disease in patients with type 2 diabetes: the Renal Insufficiency And Cardiovascular Events (RIACE) Italian multicenter study. Diabetes Care. 2012;3511:2317-23. [ Links ]
41. Penno G, Solini A, Bonora E, et al. HbA1c variability as an independent correlate of nephropathy, but not retinopathy, in patients with type 2 diabetes: the Renal Insufficiency And Cardiovascular Events (RIACE) Italian multicenter study. Diabetes Care. 2013;368:2301-10. [ Links ]
42. Solini A, Penno G, Bonora E, et al. Diverging association of reduced glomerular filtration rate and albuminuria with coronary and noncoronary events in patients with type 2 diabetes: the renal insufficiency and cardiovascular events (RIACE) Italian multicenter study. Diabetes Care. 2012;351:143-9. [ Links ]
43. Delanaye P, Glassock RJ, Pottel H, Rule AD. An age-calibrated definition of chronic kidney disease: rationale and benefits. Clin Biochem Rev. 2016;371:17-26. [ Links ]
44. Drury PL, Ting R, Zannino D, et al. Estimated glomerular filtration rate and albuminuria are independent predictors of cardiovascular events and death in type 2 diabetes mellitus: the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) study. Diabetologia. 2011;541:32-43. [ Links ]
45. Kramer CK, Leitao CB, Pinto LC, Silveiro SP, Gross JL, Canani LH. Clinical and laboratory profile of patients with type 2 diabetes with low glomerular filtration rate and normoalbuminuria. Diabetes Care. 2007;308:1998-2000. [ Links ]
46. Yu M, Ryu DR, Kim SJ, Choi KB, Kang DH. Clinical implication of metabolic syndrome on chronic kidney disease depends on gender and menopausal status: results from the Korean National Health and Nutrition Examination Survey. Nephrol Dial Transplant. 2010;252:469-77. [ Links ]
47. Mottl AK, Kwon KS, Mauer M, Mayer-Davis EJ, Hogan SL, Kshirsagar AV. Normoalbuminuric diabetic kidney disease in the U.S. population. J Diabetes Complication. 2013;272:123-7. [ Links ]
48. Ekinci EI, Jerums G, Skene A, et al. Renal structure in normoalbuminuric and albuminuric patients with type 2 diabetes and impaired renal function. Diabetes Care. 2013;3611:3620-6. [ Links ]
49. Budhiraja P,Thajudeen B, Popovtzer M. Absence of albuminuria in type 2 diabetics with classical diabetic nephropathy: Clinical pathological study. J Biomed Sci Eng. 2013;6:20-5. [ Links ]
50. Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD.Am J Kidney Dis. 2014;635:713-35. [ Links ]
51. Tabaei BP, Al-Kassab AS, Ilag LL, Zawacki CM, Herman WH. Does microalbuminuria predict diabetic nephropathy? Diabetes care. 2001;249:1560-6. [ Links ]
52. Moriya T, Moriya R, Yajima Y, Steffes MW, Mauer M. Urinary albumin as an indicator of diabetic nephropathy lesions in Japanese type 2 diabetic patients. Nephron. 2002;912:292-9. [ Links ]
53. Caramori ML, Fioretto P, Mauer M. The need for early predictors of diabetic nephropathy risk: is albumin excretion rate sufficient? Diabetes. 2000;499:1399-408. [ Links ]
54. Niewczas MA, Gohda T, Skupien J, et al. Circulating TNF receptors 1 and 2 predict ESRD in type 2 diabetes. J Am Soc Neprol. 2012;233:507-15. [ Links ]
55. Kamijo-Ikemori A, Sugaya T, Yasuda T, et al. Clinical significance of urinary liver-type fatty acid-binding protein in diabetic nephropathy of type 2 diabetic patients. Diabetes Care. 2011;343:691-6. [ Links ]
56. Nauta FL, Boertien WE, Bakker SJ, et al. Glomerular and tubular damage markers are elevated in patients with diabetes. Diabetes Care. 2011;344:975-81. [ Links ]
57. Kopf S, Oikonomou D, von Eynatten M, et al. Urinary excretion of high molecular weight adiponectin is an independent predictor of decline of renal function in type 2 diabetes. Acta Diabetol. 2014;513:479-89. [ Links ]
58. Chien HY, Chen CY, Chiu YH, Lin YC, Li WC. Differential microRNA profiles predict diabetic nephropathy progression in Taiwan. Int J Med Sci. 2016;136:457-65. [ Links ]
59. Narita T, Hosoba M, Kakei M, Ito S. Increased urinary excretions of immunoglobulin g, ceruloplasmin, and transferrin predict development of microalbuminuria in patients with type 2 diabetes. Diabetes Care. 2006;291:142-4. [ Links ]
60. Araki S, Haneda M, Koya D, et al. Association between urinary type IV collagen level and deterioration of renal function in type 2 diabetic patients without overt proteinuria. Diabetes Care. 2010;338:1805-10. [ Links ]
61. Zurbig P, Jerums G, Hovind P, et al. Urinary proteomics for early diagnosis in diabetic nephropathy. Diabetes. 2012;6112:3304-13. [ Links ]
62. Vassalotti JA, Centor R, Turner BJ, et al. Practical approach to detection and management of chronic kidney disease for the primary care clinician. Am J Med. 2016;1292:153-62. [ Links ]
63. American Diabetes A. Standards of medical care in diabetes--2014. Diabetes Care. 2014;371:S14-80. [ Links ]
64. Rigalleau V, Lasseur C, Raffaitin C, et al. Normoalbuminuric renal-insufficient diabetic patients: a lower-risk group. Diabetes Care. 2007;308:2034-9. [ Links ]
65. Dreyer G, Hull S, Mathur R, Chesser A, Yaqoob MM. Progression of chronic kidney disease in a multi-ethnic community cohort of patients with diabetes mellitus. Diabet Med. 2013;308:956-63. [ Links ]
66. Ruggenenti P, Porrini EL, Gaspari F, et al. Glomerular hyperfiltration and renal disease progression in type 2 diabetes. Diabetes care. 2012;3510:2061-8. [ Links ]
67. Soleymanian T, Hamid G, Arefi M, et al. Non-diabetic renal disease with or without diabetic nephropathy in type 2 diabetes: clinical predictors and outcome. Ren Fail.2015;374:572-5. [ Links ]
Regina Silva
Al. Prof. Hernani Monteiro, 4200-319, Porto, Portugal
E-mail: regina_silva30@hotmail.com
Disclosure of potential conflicts of interest: none declared.
Received for publication: Jan 3, 2017
Accepted in revised form: May 22, 2017


{kind=link}
{kind=link}