










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.31 no.1 Lisboa mar. 2017
ORIGINAL ARTICLE
Survival of hemodialysis patients: A new reality?
Carolina Belino, Augusto Coelho, Susana Pereira, Daniela Lopes, Ana Marta Gomes, Ana Ventura
1 Haemodialysis Centre Hemoatlântico Gaia, Diaverum, Vila nova de Gaia, Portugal
ABSTRACT
Introduction: Survival rates of haemodialysis patients have increased worldwide over the last decade. The purposes of this study were to analyze the 10‑year survival rate and to identify mortality risk factors in a Portuguese cohort. Subjects and Methods: Data was collected from 273 incident patients on facility haemodialysis treatments between 2005 and 2015. Sociodemographic data, medical history, clinical and analytic parameters were collected. A statistical analysis using Kaplan‑Meier survival analysis and Cox regression were performed. Results: Median age was 71 ± 15.5 [22; 91] years, 56.8% were male. Fistula was the first access in 68.5%. Median survival rate was 89 ± 8.8 months. There were 93 deaths (34%). Of the 23 deaths occurring in the first year, 65% (n=15) were during the first 90 days. Mortality risk factors were residence in a nursing home (OR 2.8; p<0.05), coronary heart disease (OR 2.3; p<0.05), central venous catheter use (OR 2.1; p<0.05), history of hospitalizations in year prior to dialysis admission (OR 1.9; p<0.05) and advanced age (OR 1.5; p<0.05). Conclusions: Patients starting haemodialysis in the last decade are mainly elderly and have a prolonged lifespan, reflecting good levels of care. Functional status and dependence, extremes of age, central venous catheter use and high cardiovascular burden are related with greater mortality and should prompt consideration for a more conservative approach.
Keywords: haemodialysis, risk factors, mortality, survival.
INTRODUCTION
Survival rates of haemodialysis patients are increasing worldwide. The global two‑year survival rate of incident haemodialysis patients increased from 80.6% to 82.2% between 2006 and 2010 in Europe1. A 21% reduction in mortality of patients on facility haemodialysis therapy between 2008 and 2012 compared to 1998 to 2002 was shown in a recent analysis of ANZDATA registry2. Similarly, a decrease in mortality of more than 19% from 2003 to 2011 was reported from Medicare and Medicaid centres in the USA3. This study´s aims were to analyze the 10‑year survival rate and to identify risk factors for mortality in a Portuguese cohort.
SUBJECTS AND METHODS
Data from all incident patients in a Portuguese haemodialysis facility between 2005 and 2015 were retrieved using the IT system. Sociodemographic data, functional status, medical history, health resource use, institutionalization, dialysis‑related information and laboratory data were collected.
Patient characteristics were analyzed by standard descriptive statistics. Kolmogorov‑Smirnov test was used to test normality distribution of variables. A Kaplan‑Meier survival analysis was made, taking into account as competing risk events renal transplantation, transfer to another facility and switch to peritoneal dialysis.
Estimates of cumulative incidence function were calculated and survival probabilities were compared using the log‑rank test. Cox regression models were then performed and fitted using backward elimination method to develop the final multivariate model which included all variables with p values < 0.05. All analyses were performed using SPSS Statistics software v19.0.
RESULTS
Characteristics of patients
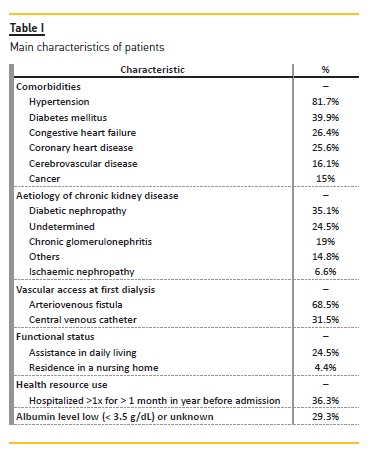
A total of 273 patients were included, one patient black and the others Caucasian. Male patients were 56.8%. Global median age was 71 ± 15.5 [22; 91] years, male median age was 70 ± 16.3 [22; 91] years and female median age was 72 ± 14 [22; 89] years. Table 1 summarizes patients main characteristics.
Outcomes
Median follow‑up time was 44.9 ± 36.3 months. Death was the main cause of loss of follow‑up (n=93; 34.1%), followed by renal transplantation (n= 41; 15%), transfer to other facility (n=10; 3.7%) or switch to peritoneal dialysis (n=3; 1.1%).
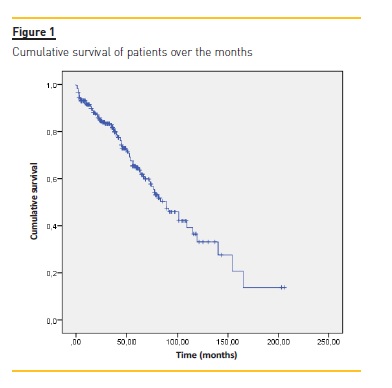
Median survival rate was 89 ± 8.8 months (95% confidence interval [71.6‑106.4]) (figure 1). Cumulative survival rates at 2, 5 and 10 years were 93.4%, 90.6% and 83.5%.
Twenty‑three deaths (24.7%) occurred in the first year of dialysis, which was the year with the highest mortality rate. Of these 23 deaths, 15 occurred in the first three months (65%). Those who died in this early period were mostly men (n=10; 3.6%), with median age 73.5 ± 6.82 years. About 46.7% were dependent; 13.3% lived in nursing homes and 80% had had hospitalizations in previous year.
Cardiovascular comorbidities were frequent: hypertension (66.7%), diabetes mellitus (60%), coronary heart disease (60%), congestive heart failure (40%). Central vascular catheter (CVC) was the first access in 60% of patients.
Risk Factors for Mortality
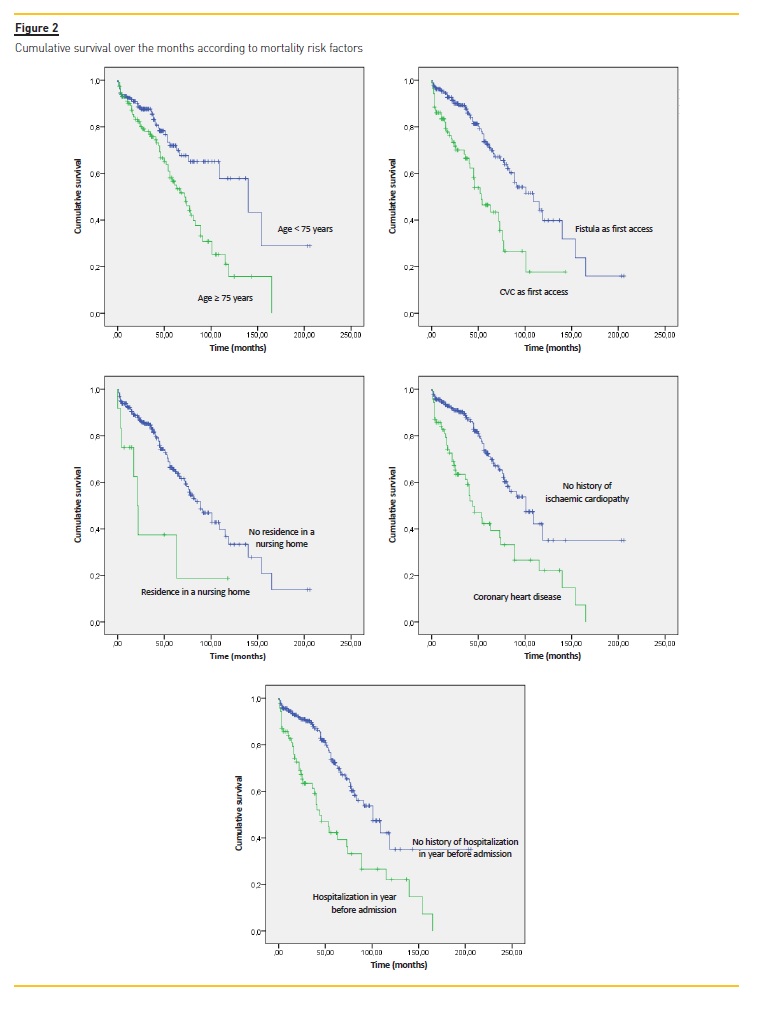
Variables associated with poor survival are described in table II and survival curves are expressed in figure 2.
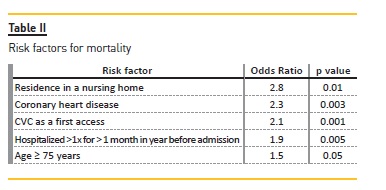
Residence in nursing home was the major risk factor.
DISCUSSION
Major findings of our study were: 1) older age of patients starting haemodialysis; 2) outcomes comparable between genders despite male prevalence; 3) predominance of fistula as the first vascular access; 4) importance of cardiovascular burden and functional status in mortality; 5) high early mortality rates (first 3 months) in elderly; 6) prolonged lifespan of patients.
We will discuss each of these findings. Age of patients starting dialysis is increasing. An age range between 54 years in UK to 62.4 years in Italy was shown in 20046 and a mean age superior to 60 years was already reported by 2013 ERA‑EDTA Registry Annual Report7. The rise in the population´s average age, improvements in disease management, prolonged survival of patients with chronic illnesses and policies accepting older and polymorbid patients for haemodialysis contributed to an older age at time of starting dialysis4,5.
There is a male predominance among incident haemodialysis patients, as reported in the DOPPs study5, where males were 59% of patients, and in other cohorts4,8,9. However, as in this study, outcomes were comparable between genders.
Use of CVC as a vascular access for dialysis is independently associated with greater mortality risk. The NKF KDOQI10 goal of prevalent functional fistula placement rate of greater than 65% of patients was achieved in this cohort and improved survival rates.
As in other cohorts, there was a high prevalence of cardiovascular comorbidities and coronary heart disease was associated with a 2.3 times higher risk for mortality. It is one of the most important diseases to put under tight control and vigilance and improvements in vascular calcification and dialysis efficacy help to reduce associated morbidity and mortality11.
Residence in a nursing home and history of hospitalizations in the year before admission to a dialysis programme were associated with greater mortality risk.
A posterior analysis from the DOPPs study12 showed similar results, with a strong association between greater functional dependence and mortality, dialysis withdrawal and time to first hospitalization.
There was a high mortality in the first three months. Patients who died were older, more dependent and had severe disease. In fact, worldwide, mortality risk is high soon after initiation of haemodialysis13. The first 90 days of treatment is a critical period of physical and psychological adaptation and the choice of modality may not yet be definitive. In 2007, Bradbury et al.14 identified factors associated with early mortality: older age, CVC use, low serum albumin levels (<3.5 g/dL) and phosphorous levels (<3.5 mg/dL) and inadequate predialysis nephrology care. Those findings should prompt a careful evaluation of current dialysis initiation practices. A conservative approach with improvement of functional status for those at extremes of age, with high dependency and multiple comorbidities may provide better quality of life.
Prolonged lifespan of patients is probably associated with technical and procedural innovations in dialysis therapy, better control and treatment of diabetes and cardiovascular complications along with general medical treatment options, with development of new medications having beneficial effects on morbidity and mortality. A holistic approach, patient‑centred, with involvement of a multidisciplinary team of care may also made the difference4,11‑14.
This study is based on a single‑centre experience, so further investigations are necessary in order to determine if the results are applicable to all Portuguese haemodialysis patients. However, this study covers a period of time of ten years and to our best knowledge, this is the only published Portuguese study to date to cover such a large time span.
CONCLUSIONS
Characteristics of haemodialysis patients in Portugal are probably changing. More elderly patients being on dialysis and a prolonged lifespan may be attributable to the better survival of individuals with cardiovascular and metabolic complications, as well as medical and technical advances in dialysis therapy and better vascular access care. Accepting older and polymorbid patients for dialysis is a challenge for the multidisciplinary care team in order to reduce early mortality rates.
The need for reassessment of current dialysis initiation practices is strengthened, helping to design future developments to face increasing prevalence of this epidemic disease.
References
1. Pippias M, Stel VS, Abad Diez JA, et al. Renal replacement therapy in Europe: a summary of the 2012 ERA‑EDTA Registry Annual Report. Clin Kidney J 2015; 8:248–261. [ Links ]
2. Marshall MR, Polkinghorne KR, Kerr PG, Agar JW, Hawley CM, McDonald SP. Temporal changes in mortality risk by dialysis modality in the Australian and New Zealand dialysis population. Am J Kidney Dis 2015;66:489–‑498. [ Links ]
3. Peer Kidney Care Initiative. Recent decrease in death rates among dialysis patients. Am J Kidney Dis 2015;65:A1–‑A93. [ Links ]
4. Lehmann P, Ambul M, Corleto D, Klaghofer R, Ambühl P. Epidemiologic trends in chronic renal replacement therapy over forty years: a Swiss dialysis experience. BMC Nephrology 2012:13:52. [ Links ]
5. Hecking M, Bieber B, Ethier J, et al. Sex‑specific differences in hemodialysis prevalence and practices and the male‑to‑female mortality rate: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Plos One 2014;11: e1001750. [ Links ]
6. Rayner HC, Pisoni RL, Bommer J, et al. Mortality and hospitalization in haemodialysis patients in five European countries: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant 2004;19:108–‑120. [ Links ]
7. Kramer A, Pippias M, Stel VS, et al. Renal replacement therapy in Europe: a summary of the 2013 ERA‑EDTA Registry Annual Report. Clin Kidney J 2016;9:457–469. [ Links ]
8. Carrero J, Mutsert R, Axelsson J, et al. Sex differences in the impact of diabetes on mortality in chronic dialysis patients. Nephrol Dial Transplant 2011;26: 270-276. [ Links ]
9. Portuguese Society of Nephrology 2016 Annual Report. Available at http://www.spnefro.pt/tratamento_da_doenca_renal_terminal/2016/. Accessed October 22, 2016. [ Links ]
10. The National Kidney Foundation Kidney Disease Outcomes Quality Initiative. Available at http://www2.kidney.org/professionals/KDOQI/guideline. Accessed October 22, 2016. [ Links ]
11. Herzog C, Asinger R, Berger A, et al. Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 2011;80:572-586. [ Links ]
12. Jassal S, Karaboyas A, Bieber B, et al. Functional dependence and mortality in the International Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 2016;67:283-292. [ Links ]
13. Noordzij M, Jager K. Increased mortality early after dialysis initiation: a universal phenomenon. Kidney Int 2014;85:12-14. [ Links ]
14. Bradbury BD, Fissel RB, Albert JM, et al. Predictors of early mortality among incident US hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin J Am Soc Nephrol 2007;2:89-99. [ Links ]
Carolina Lã Belino
Department of Nephrology
Vila Nova de Gaia e Espinho Hospital Centre
Rua Conceição Fernandes
4434‑502 Vila Nova de Gaia, Portugal
E-mail: carolinabelino@hotmail.com
Disclosure of potential conflicts of interest: none declared
Contributions: All authors contributed to the drafting of the manuscript, search strategy, data extraction and results interpretation and discussion. All contributed with medical expertise on haemodialysis. CB and SP performed the statistical analysis.
Received for publication: Dec 19, 2016
Accepted in revised form: Mar 8, 2017


{kind=link}