










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
Print version ISSN 0872-0169
Port J Nephrol Hypert vol.31 no.1 Lisboa Mar. 2017
ORIGINAL ARTICLE
24-hour ambulatory blood pressure monitoring in chronic kidney disease and its influence on treatment
Catia Cunha1, Susana Pereira1, João Carlos Fernandes1, Vítor Paixão Dias2
1 Nephrology Department, Centro Hospitalar de Vila-Nova de Gaia, Portugal
2 Internal Medicine Department, Centro Hospitalar de Vila-Nova de Gaia, Portugal
ABSTRACT
Introduction: Chronic kidney disease (CKD) is strongly associated with hypertension (HTN) and each can cause or aggravate the other. Misclassification of BP control is an important problem in hypertensive patients with CKD, making ambulatory blood pressure monitoring (ABPM) an important tool. The aim of our study was to review the influence of ABPM results in antihypertensive treatment and BP control in hypertensive CKD patients.
Methods: Retrospective observational study; inclusion of hypertensive CKD patients stages 1 to 5 not on dialysis who performed ABPM in our department; data collected from clinical records and ABPM reports.
Results: A total of 54 hypertensive CKD patients were reviewed. Reasons appointed for requesting ABPM included suspicion of resistant hypertension (40.7%), uncontrolled hypertension (29.6%), white coat hypertension (16.7%), hypotension (9.2%) and masked hypertension (3.8%). Interestingly, pre-ABPM clinical interpretation of BP control was found inadequate in 55.6% of patients.
Conclusion: Misclassification of BP was a significant problem. As a result of these findings our department incorporated ABPM more routinely as recommended best practice.
Keywords: Hypertension, chronic kidney disease, ambulatory blood pressure monitoring.
INTRODUCTION
Chronic kidney disease (CKD) is strongly associated with hypertension (HTN) and each can cause or aggravate the other. A cohort study from 2010 reported that 86% of CKD patients had hypertension while 58% of those hypertensive were treated with 3 or more medications1. Also, both HTN and CKD are major risk factors for cardiovascular disease2-4.
There is no doubt that blood pressure (BP) control is fundamental to the care of patients with CKD and is relevant at all stages of CKD regardless of the underlying cause5. However, misclassification of BP control when using BP office readings, is a significant issue and was observed in 1 of 3 hypertensive patients with CKD in a cross-sectional study, including 5693 hypertensive patients with CKD, undertaken by the Spanish ambulatory blood pressure monitoring (ABPM) registry, supporting the use of ABPM6. In this study, control of BP during the 24-hour period was much better than that based on office readings, independent of CKD stage. Evaluation of ambulatory BP also showed a remarkable amount of underestimation (white coat hypertension) and overestimation (masked hypertension) of BP control, which could lead to over- and undertreatment, respectively.
The aim of this study was to review the results of ABPM in our CKD patients and the results value in guiding changes in antihypertensive therapy.
METHODS
Study design and study population
This is a retrospective observational study with data collected from clinical records from January 2012 to June 2016 in the Nephrology Department of Hospital de Vila-Nova de Gaia/ Espinho, Portugal. Patients were recruited from those who performed ABPM in our Renal Department during the study period, referred from the General Nephrology Clinic and Hypertension-Nephrology Clinic.This study was designed, implemented, and reported in accordance with ICH guidelines for Good Practice and Declaration of Helsinki 1975, revised Hong Kong 1989. The manuscript was prepared in accordance with the STROBE guidelines for observational studies.
Selection criteria included hypertensive patients with CKD stages 1 to 5 (not on renal replacement therapy), with a valid ABPM performed from January 2012 to June 2016 in our Nephrology department.
Exclusion criteria included invalid ABPM and patients on renal replacement therapy, because most of these were referred from satellite haemodialysis units and access to clinical information was limited.
Data was collected from medical records and ABPM reports.
The number of consecutive cases that met the inclusion criteria within the study period determined the sample size.
Measurements
ABPM was performed with Spacelabs Models 90207-30 and 90217A devices. The monitor recorded BP at a 15-minute interval for the daytime period and 30-minute interval for the night-time period. Cuff-size was chosen based on arm circumference and fixed to the non-dominant arm. Recordings were performed on working days and patients were instructed to maintain their usual activities and keep the arm extended and immobile at the time of cuff inflation7. All patients were given a form to record going-to-bed and gettingup times, which defined the daytime and night-time periods in the ABPM analysis. They were also instructed to register any symptom during this period of the test and the times each anti-hypertensive medication prescribed was taken. ABPM measurements were considered valid only if more than 65% of measurements were successful.
Clinical information collected from medical records included age, sex, stage and aetiology of HTN, aetiology of CKD, body mass index, smoking, presence of diabetes, dyslipidaemia, target-organ damage, such as, left ventricular hypertrophy, and associated clinical conditions including coronary heart disease, cerebrovascular disease and heart failure. Data regarding criteria used for ABPM request and anti-hypertensive treatment prescribed pre and post-ABPM was obtained from medical records in clinics.
Definitions
CKD is defined as abnormalities of kidney structure or function, present for more than 3 months. Stage 1 CKD is defined as estimated glomerular filtration ratio (eGFR≥ 90 mL/min/1.73 m2plus elevated urine albumin excretion; in other words, either microalbuminuria (albumin-creatinine ratio of 30-300 mg/g) or macroalbuminuria (albumin-creatinine ratio>300 mg/g) or evidence of structural abnormalities. Stage 2 CKD was defined as eGFR≥60 and<90 mL/min/1.73 m2and elevated urine albumin excretion. Stages 3, 4, and 5 CKD were defined as eGFR ≥30 and<60, ≥15 and<30, and <15 mL/min/ 1.73 m2, respectively8. eGFR was estimated with the MDRD (Modification of Diet in Renal Disease) equation9.
Thresholds for hypertension diagnosis based on ABPM reports followed consensus values: 24-h avera ge ≥ 1 3 0 / 8 0 m m H g ; awa ke ( d ay t i m e ) ave rage≥ 135/85 mmHg; and asleep (night-time) average ≥ 120/70 mmHg10. However, for the purpose of this study, changes in treatment performed by the responsible physician based on ABPM results were used to determine the adequacy of BP control for each patient. This was used instead of a fixed target BP, considering the importance of individualizing targets (according to age, co-existent cardiovascular disease and other comorbidities, degree of proteinuria and other risk factors of CKD progression, presence or absence of diabetic retinopathy and tolerance to treatment)11,12.
White coat effect was defined as the rise in BP that occurs in the medical environment regardless of the daytime ABPM level or the use of antihypertensive drugs7. Masked hypertension was defined as the presence of office BP in target levels with average BP on ABPM above target level. A non-dipping pattern was defined as an average night-time BP drop less than 10% from the daytime average13.
Statistical analysis
Data is presented as mean ± standard deviation for continuous variables, absolute frequencies and percentages for categorical variables. Analysis was performed using the SPSS version 17 (IBM) computer software program.
RESULTS
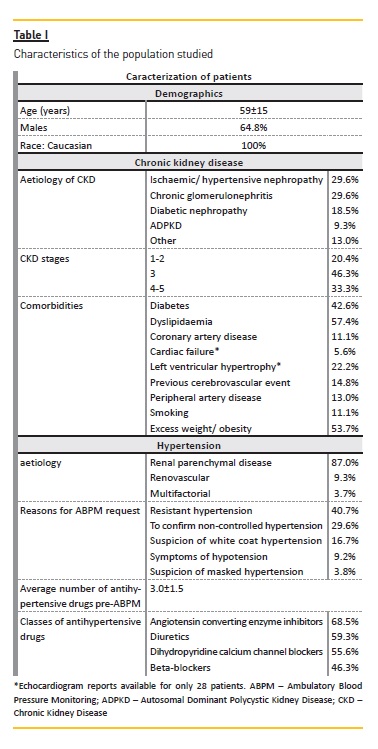
Demographics and clinical characteristics of study population (Summarized in Table I)
A total of 54 patients were included in the study, all Caucasian, 64.8% men. Mean age was 59 (±15) years. Diabetes was present in 42.6%; dyslipidaemia in 57.4%; coronary artery disease in 11.1%; cardiac failure in 5.6%; cerebrovascular disease in 14.8% and peripheral artery disease in 13.0%. A total of 53.7% were overweight or obese and 11.1% were current smokers.
Almost half of the patients had stage 3 CKD (46.3%); 11 patients were in stages 1 or 2 (20.4%) and 18 patients in stages 4 and 5 (33.3%). Main aetiologies of CKD included ischaemic/ hypertensive nephropathy (29.6%) and glomerulonephritis (29.6%), followed by diabetic nephropathy (18.5%), autosomal dominant polycystic kidney disease (9.3%) and other/undetermined cause (13.0%).
Hypertension aetiology was predominantly related to renal parenchymal disease (87.0%), with 9.3% of cases of renovascular hypertension and 2 multifactorial cases (3.7%). The average number of antihypertensive drugs pre-ABPM was 3.0±1.5, with a predominance of angiotensin converting enzyme inhibitors (68.5%), diuretics (59.3%), dihydropyridine calcium channel blockers (55.6%) and beta-blockers (46.3%). More than half of the patients (51.9%) were classified as having resistant hypertension.
Criteria for ABPM request and results
Reasons appointed for ABPM request were as follows (Table I): to confirm true resistant hypertension (40.7%), uncontrolled hypertension (29.6%), suspicion of WCH (16.7%), symptoms of hypotension (9.2%) and suspicion of masked hypertension (3.8%). Mean valid ABPM measurements was 84.8±9.7 % of total.
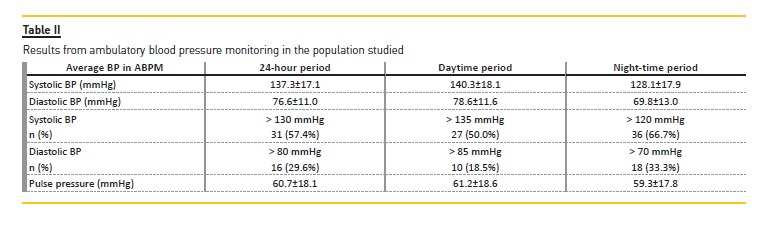
Data from ambulatory BP is listed in Table II. Average 24-hour BP was 137/77 mmHg; 61.0% had 24-hour systolic BP > 130 mmHg and 30.4% diastolic BP > 80 mmHg. Only 13 patients (24.1%) had both average 24-hour systolic and diastolic BP ≤ 130 mmHg and ≤80 mmHg, correspondingly.
Mean pulse pressure was 60.7 (± 18.1) mmHg in the 24-hour period, with 23 patients (42.6%) with a mean pulse pressure over 60. Fifty percent of patients presented a dipper pattern of BP. White coat effect was detected in 22.2% of patients.
Influence of ABPM in treatment and agreement with pre-ABPM clinical evaluation of BP control
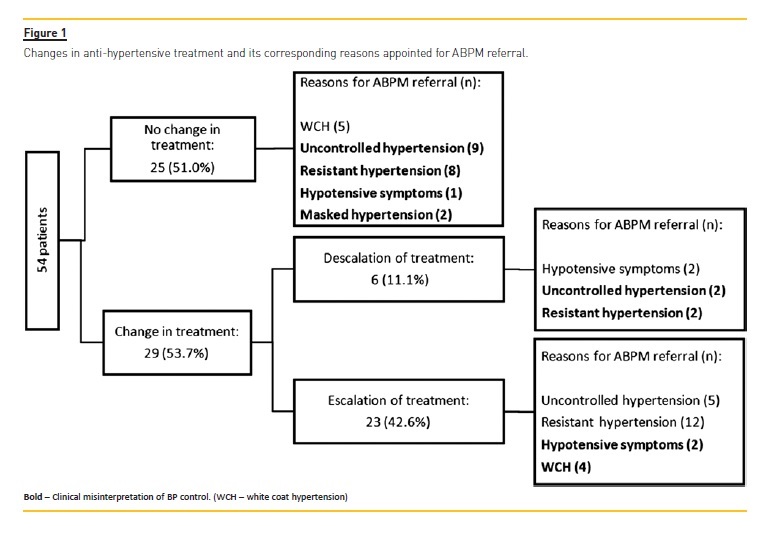
Changes in anti-hypertensive treatment based on ABPM and correspondent reasons for ABPM request are shown in Figure 1. Twenty-five patients (46.3%) required no change in anti-hypertensive treatment; 23 (42.6%) required escalation of anti-hypertensive treatment and 6 (11.1%) had their medication reduced after ABPM results (Figure 1).
We found a pre-ABPM misclassification of BP control in 55.6% of patients (n=30). This includes 20 patients thought to have either uncontrolled or excessive BP control who required no change in treatment; 6 patients referred because of suspicion of excessive BP controlor WCH who actually required intensification of antihypertensive drug and 4 patients suspected of uncontrolled BP who were found to be overtreated. Average number of anti-hypertensive medication post ABPM was 3.1±1.6, similar to the number pre-ABPM.
DISCUSSION
HTN constitutes a very relevant cardiovascular and renal risk factor in patients with CKD. A cohort study from 2010 reported that 86% of CKD patients had hypertension while 58% of those hypertensive were treated with 3 or more medications1. The major outcomes relevant to BP control in CKD patients are kidney disease progression and cardiovascular events, including stroke5. Increasing BP relates with more than 20% increase in risk of end-stage renal disease compared to those with normal BP14.
ABPM is the recognised gold standard for the assessment of hypertension and ABPM patterns have been stablished as having prognostic importance in the general hypertensive population15,16. It detects masked HTN, isolated nocturnal hypertension and non-dipper pattern of BP, conditions of known cardiovascular risk17.
It also detects WCH, avoiding overtreatment and its associated risks. There is evidence that WCH, masked HTN and non-dipper pattern of BP are more frequent in CKD, which makes ABPM of particular importance in this population16-18. Clinical indications for ABPM are well defined in literature10.
KDIGO guidelines on the management of BP in CKD acknowledge the role of ABPM in CKD patients, based on evidence for a better prediction of renal and cardiovascular outcomes with ABPM than with office readings5.
In our study, justifications for ABPM were consonant with the current recommendations: to confirm resistant hypertension (40.7%), uncontrolled hypertension (29.6%), suspicion of WCH (16.7%), symptoms of hypotension (9.2%) and suspicion of masked hypertension (3.8%).
When we consider guidelines based on fixed thresholds for hypertension diagnosis with ABPM10, we found 61.0% of our patients had 24-hour systolic BP > 130 mmHg and 30.4% diastolic BP > 80 mmHg. Control of systolic BP was consistently worse both in daytime and night-time periods, when compared to diastolic BP control. Mean pulse pressure was 60.7 (± 18.1) mmHg in the 24-hour period. This is consistent with literature.
Patients with CKD present significantly elevated ambulatory PP, reflecting increased arterial stiffness and enhanced CVD risk19. Increased arterial stiffening in CKD and end-stage renal disease (ESRD) patients is of multifactorial origin, with extensive arterial calcifications representing a major covariate20. Therefore, CKD patients have an altered night-time pressure profile and higher pulse pressure that translate into a more severe cardiac damage21.
Fifty percent of our patients presented a non-dipper pattern of BP, a proportion slightly lower than described in other studies. The exclusion of patients on dialysis, known for increasing proportion on non-dipper pattern, might explain the difference. A cross-sectional study involving 10271 hypertensive patients, enrolled in the Hygia Project, of which 3227 had CKD, showed a nondipper prevalence of 61% in hypertensive patients with CKD (vs 43% in those without CKD) and a significant increase in the proportion of non-dipper status with increasing stage of worsening CKD19. The incidence is significantly higher in patient on dialysis: 82% in a retrospective study (22) and 80% in the AASK cohort study23. Higher prevalence of non-dipper pattern of BP may be explained by increased sympathetic nervous system activation, more common obstructive sleep apnoea, sedentary lifestyle and poor sleep quality, as well as common concurrent comorbidities13.
In this study, we looked at the influence of ABPM in treatment changes as a marker of adequate or inadequate control of BP for a specific patient, instead of using a fixed BP target for all. This was based on theKDIGO recommendations that it is good clinical practice to assess the risks and benefits of BP-lowering treatment in an individual patient and to tailor therapy accordingly5. There is growing evidence that a strict BP goal of < 130/80 mmHg for individuals with CKD may not be beneficial for renal protection and that low blood pressure has been associated with increased cardiovascular events in interventional studies for cardiorenal protection24-27.
We found that 44.4% required no change in antihypertensivetreatment after ABPM, even though in 83.3% of these the previous clinical suspicions would have led to unnecessary changes with consequent under-or overtreatment. Additionally, 42.6% of the patients required escalation of anti-hypertensive treatment and 11.1% had their medication reduced afterABPM results. Again, the previous clinical evaluation was inadequate in 34.5% of these patients.
Our results support the important role of ABPM in the correct evaluation of BP control in CKD patients and a valuable guide to anti-hypertensive adjustments, with an inadequate clinical interpretation (over- or underestimation) of BP control in 55.6% of patients. This is consistent with previous published results. A 5693-patient cross-sectional analysis from Spain showed a misclassification of office blood pressure control in 1 of 3 hypertensive patients with CKD because of WCH or masked hypertension (35% misclassification), with an average overestimation of systolic/ diastolic office BP of around 21/11 mmHg6. Similarly, a recent Chinese study also provided evidence of disparate assessment of clinic blood pressure and ABPM in patients with CKD (difference in systolic BP/ diastolic BP between clinic BP and ABPM was 9.8 mmHg and 6.65 mmHg, respectively, with a more substantial difference in older patients mostly due to higher prevalence of masked hypertension)28.
Data demonstrates inconsistent results in office measurements vs ABPM and that information from ABPM can potentially impact future cardiovascular and renal outcomes in patients with CKD29. So, even though it might be time consuming and costly, ABPM is worth considering, particularly in CKD patients.
An important limitation of our study was the small number of patients included. Additionally, adequate BP control is inferred from therapeutic attitudes and so potentially prone to error. Additional useful information would be the re-evaluation of BP control in those submitted to changes in treatment with a second ABPM, but none of these patients repeated this exam.
Our results are consistent with literature and stress the important role of ABPM in BP evaluation in CKD patients. More randomized controlled trials are necessary to determine if routine use of ABPM in CKD actually results in a better prognosis for these patients.
CONCLUSION
ABPM appears as an important tool not only to detect CKD patients who need intensification of antihypertensive treatment but also to identify excessive BP control, both associated with complications. ABPM must be part of the nephrologists clinical practice. In our nephrology department, we have integrated as part of our routine care of hypertension in CKD.
References
1. Munter P, Anderson A, Charleston J, et al. Hypertension awareness, treatment, and control in adults with CKD: results from the Chronic Renal Insuficiency Cohort (CRIC) Study. Am J Kidney Dis. 2010; 55:441-451. [ Links ]
2. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002; 360:1903-1913. [ Links ]
3. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004; 351:1296-1305. [ Links ]
4. Debella YT, Giduma HD, Light RP, Agarwal R. Chronic kidney disease as a coronary disease equivalent – a comparison with diabetes over a decade. Clin J Am Soc Nephrol. 2011; 61385-1392. [ Links ]
5. Kidney Disease: Improving Global Outcome (KDIGO) Blood Pressure Work Group. KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int Suppls. 2012; 2:337-414. [ Links ]
6. Gorostidi M, Sarafidis PA, de la Sierra A, et al. Differences between office and 24-hour blood pressure control in hypertensive patients with CKD: a 5,693-patient cross-sectional analysis from Spain. Am J Kidney Dis. 2013; 62:285-294. [ Links ]
7. OBrien E, Asmar R, Beilin L, et al. European Society of Hypertension recommendations for conventional, ambulatory and home blood pressure measurement. J Hypertens. 2003; 21:821-848. [ Links ]
8. National Kidney Fundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002; 39(Suppl2):S1-S290. [ Links ]
9. Levey AS, Coresh J, Greene T, et al. Using standardized serum creatinine values in the Modification of Diet in Renal Disease study equation for estimation of glomerular filtration rate. Ann Intern Med. 2006; 145:247-254. [ Links ]
10. OBrien E, Parati G, Stergiou G, et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013; 31:1731-1768. [ Links ]
11. Kidney Disease: Improving Global Outcome (KDIGO) Blood Pressure Work Group. KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppls. 2013; 3:1-150. [ Links ]
12. Verbeke F, Lindley E, Van Bortel L, et al. A European Renal Best Practice (ERBP) position statement on the Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline for the management of blood pressure in non-dialysis-dependent chronic kidney disease: an endorsement with some caveats for real-life application. Nephrol Dial Transplant. 2014; 29:490-496. [ Links ]
13. Sinha AD, Agarwal R. The complex relationship between CKD and ambulatory blood pressure patterns. Adv Chronic Kidney Dis.2015; 22:102-107. [ Links ]
14. Klag MJ, Whelton PK, Randall BL, et al. Blood pressure and end-stage renal disease in men. N Engl J Med. 1996; 354:2368-2374. [ Links ]
15. Pickering TG, Shimbo D, Haas D. Ambulatory blood-pressure monitoring. N Engl J Med. 2006; 354:2368-2374. [ Links ]
16. Ruiz-Hurtado G, Gorostidi M, Waeber B, Ruilope LM. Ambulatory and home blood pressure monitoring in people with chronic kidney disease. Time to abandon clinic blood pressure measurements? Curr Opin Nephrol Hypertens. 2015; 24488-491. [ Links ]
17. OBrien E, Parati G, Stergiou G. Ambulatory blood pressure measurement: what is the international consensus? Hypertension. 2013; 62:988-994. [ Links ]
18. Franklin SS, Wong ND. The complexity of masked hypertension: diagnostic and management challenges. Curr Hypertens Rep. 2014; 16:474. [ Links ]
19. Mojón A, Ayala DE, Piñeiro L, et al. Comparison of ambulatory blood pressure parameters of hypertensive patients with and without chronic kidney disease. Chronobiol Int. 2013; 30:145-158. [ Links ]
20. Briet M, Boutouyrie P, Laurent S, London GM. Arterial stiffness and pulse pressure in CKD and ESRD. Kidney Int. 2012; 82:388-400. [ Links ]
21. Fedecostante M, Spanella F, Cola G, et al. Chronic kidney disease is characterized by double trouble higher pulse pressure plus night-time systolic blood pressure and more severe cardiac damage. PLoS One. 2014; 9:e86155. [ Links ]
22. Farmer CK, Goldsmith DJ, Cox J, Dallyn P, Kingswood JC, Sharpstone P. An investigation of the effect of advancing uraemia, renal replacement therapy and renal transplantation on blood pressure diurnal variability. Nephrol Dial Transplant. 1997; 12:2301-2317. [ Links ]
23. Pogue V, Rahman M, Lipkowitz M, et al. Disparate estimates of hypertension control from ambulatory and clinic blood pressure measurements in hypertensive kidney disease. Hypertension. 2009; 53:20-27. [ Links ]
24. Tomlinson LA, Holt SG, Leslie AR, Rajkumar C. Prevalence of ambulatory hypotension in elderly patients with CKD stages 3 and 4. Nephrol Dial Transplant. 2009; 24:3751-3755. [ Links ]
25. Minutolo R, Borrelli S, Scigliano R, et al. Prevalence and clinical correlates of white coat hypertension in chronic kidney disease. Nephrol Dial Transplant. 2007; 22:2217-2223. [ Links ]
26. Berl T, Hunsicker LG, Lewis JB, et al. Impact of achieved blood pressure on cardiovascular outcomes in the Irbesartan Diabetic Nephropathy Trial. J Am Soc Nephrol. 2005; 16:2170-2179. [ Links ]
27. Mann JF Schmieder RE, McQueen M, Dyal Let al. Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multicentre, randomised, double-blind, controlled trial. Lancet. 2008; 372:547-553. [ Links ]
28. Wang C, Gong WY, Zhang J, et al. Disparate assessment of clinic blood pressure and ambulatory blood pressure in differently aged patients with chronic kidney disease. Int J Cardiol. 2015;183:54-62. [ Links ]
29. Cohen DL, Huan Y, Townsend RR. Ambulatory blood pressure in chronic kidney disease. Curr Hypertens Rep. 2013;15:160-166. [ Links ]
Catia Cunha, MD
Nephrology Department
Centro Hospitalar de Vila-Nova de Gaia
Vila-Nova de Gaia, Portugal
E-mail: catiatcunha@gmail.com
Received for publication: Dec 21, 2016
Accepted in revised form: Feb 21, 2017


{kind=link}
{kind=link}
{kind=link}